
記住我





A 64-year-old man with a history of diabetes mellitus and alcoholic hepatitis was diagnosed with early stage esophageal cancer after a regular medical examination that included an upper gastrointestinal endoscopy. Further diagnostic imaging revealed a primary tumor, 23 cm from the incisor, confined to the esophagus without regional or distant metastases. The patient underwent video-assisted thoracoscopic (VATS) esophagectomy with mediastinal lymph node dissection, laparoscopic gastric tube formation, prophylactically thoracic duct ligation, and reconstruction with esophagogastrostomy at the neck level. The surgery was uneventful, and a right chest tube and abdominal Jackson-Pratt (JP) drain were left for drainage.
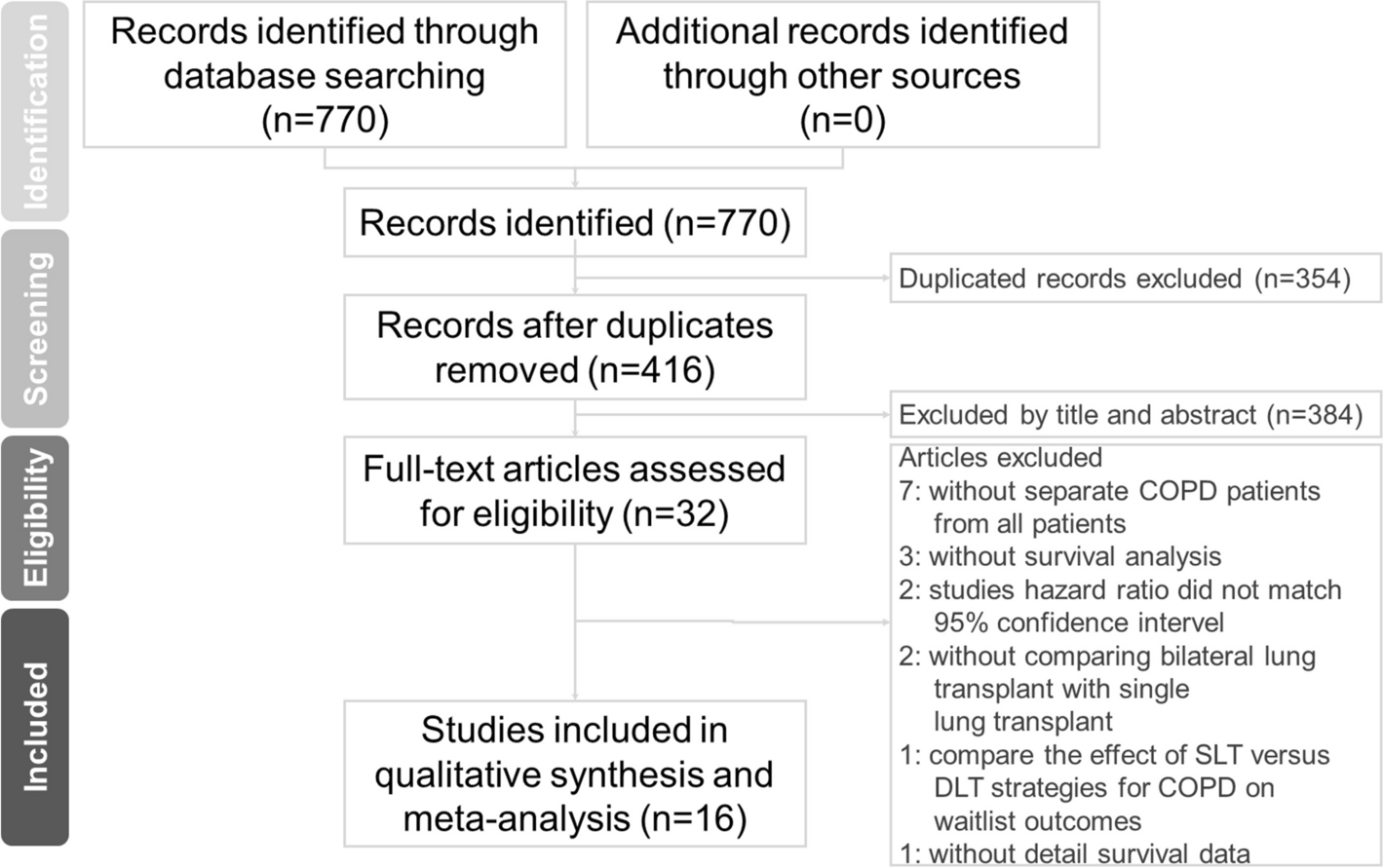
On the postoperative day (POD) 2, a chest radiograph revealed a massive left pleural effusion. A chest tube was inserted in the left thoracic cavity and about 1200 mL of effusion was drained. As the effusion was a clear yellow fluid, a wait-and-see approach was taken, but large volumes of pleural and abdominal drainage persisted during the early hospital course. However, the triglyceride concentrations in the drainage fluid were < 110 mg/dL, and the diagnosis of chylothorax was delayed. The right chest tube was removed on POD 17 followed by the left chest tube and the abdominal JP drain on POD 21. Figure 1 shows the total drainage and the drainage amounts from the left and right chest tube drainages (CTD), abdominal JP drain, and a pigtail catheter in the right thoracic cavity during the hospitalization period.
Fig. 1
Total fluid output and output volumes from the right chest tube drainage (CTD), left CTD, abdominal Jackson-Pratt drain, and right thoracic pigtail catheter during the postoperative period
Upper endoscopy on POD 6 showed suspected leakage at the anastomotic site, but esophagography on POD 19 showed no leakage, and the patient began to drink water on POD 20. Then, on POD 22, a chest radiograph revealed a large amount of right pleural effusion, and the pigtail catheter was inserted in the right thorax. The triglyceride content of the fluid was 262 mg/dL, meeting the criterion for chylothorax (> 110 mg/dL). Lymphangiography was performed on the same day.
After the diagnosis of chylothorax, conservative management began with oral midodrine on POD 23 and intravenous octreotide acetate infusion on POD 25, but the chylous leak was not controlled. The patient was kept nil per os (NPO), and total parenteral nutrition (TPN) was administered through a central venous catheter until POD 34. After several sessions of thorough consultation with the patient and his family, the patient was scheduled for VATS thoracic duct ligation and mechanical pleurodesis on POD 35 (Fig. 2B), during which a chylous leak was identified at the diaphragm (Fig. 2A). Even after the operation, the chylous leak persisted, and a second lymphangiography was performed on POD 40, followed by attempts at thoracic duct embolization on POD 41 and 42, but the effusion did not decrease (Fig. 3).
Fig. 2
Intraoperative findings: (A) visible chylous leakage at the diaphragm (white arrow); (B) the thoracic duct after ligation (yellow arrow)
Fig. 3
Thoracic duct embolization
Finally, we decided on a trial of radiotherapy, and informed consent was obtained from the patient. The clinical target volume encompassed the entire lymph node station, and a daily dose of 2 Gy was administered from POD 43 to POD 50 (14 Gy in 7 fractions). The patient had no acute adverse effects during RT, and the volume of pleural effusion gradually decreased. The right thoracic pigtail catheter was finally removed on POD 64, and the patient was discharged on POD 89. The patient was alive and well at 60 months postoperatively and no late toxicity related to RT was observed.
留言 (0)