
記住我


A 74-year-old male, 167 cm in height and 55 kg in weight (BMI 19.7), suddenly collapsed and was transferred to the Emergency Rescue department. On admission, his blood pressure was 48/31 mmHg, heart rate was 120 beats/min, SpO2 99% (5L mask), and he presented as E4V4M6. Despite extracellular fluid resuscitation, there was no response, prompting immediate initiation of the massive transfusion protocol with pumping blood transfusion. Contrast-enhanced CT revealed extensive right hemothorax with contrast leakage (Fig. 1).
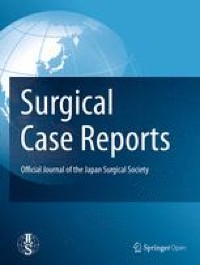
Fig. 1
Contrast-enhanced CT. Contrast-enhanced CT reveals massive pleural effusion with high CT attenuation, suggestive of a blood component, along with contrast agent leakage within the pleural cavity. Initially, the source of bleeding was suspected to be the right subclavian artery (yellow arrow)
Just before the placement of the drain, he lost consciousness, and the radial artery pulse became impalpable. The patient had concomitant distension of the jugular vein; thus, tension massive hemothorax was suspected, prompting urgent decompression drainage. Initially, we suspected bleeding from the subclavian artery and placed a drain in the second intercostal space on the midclavicular line, considering the possibility of conversion to open thoracotomy in the supine position.
Decompression was achieved, however, consciousness did not return. We expanded the incision anteriorly in the second intercostal space and performed emergency open thoracotomy; however, there was no bleeding from the thoracic apex, and the subclavian artery was intact. On the dorsal side, a large hematoma had accumulated, obscuring the bleeding point. An additional lateral thoracotomy in the fifth intercostal space was performed urgently while maintaining the supine position. Although the hematoma was significantly drained, the right lower lobe remained tense and was immobile, resulting in poor visibility. Upon re-observing the intracavity from the second intercostal incision, we observed sustained pulsatile bleeding from the fifth intercostal artery near the vertebral body. We cauterized this bleeding, which restored blood pressure and obviated the need for pumping. When we reviewed the CT for a moment before thoracotomy, it was initially thought that the diffused contrast agent was flowing out from the right subclavian artery. However, it turned out that this was the distal end of the contrast, and the actual upstream source was the contralateral side near the vertebral body, in other words, the intercostal artery.
After his condition stabilized, we learned that the patient was undergoing second-line chemotherapy with docetaxel (DTX) + ramucirumab for invasive mucinous adenocarcinoma of the right lower lobe (Fig. 2). The last dose had just been administered for the third cycle 17 days before the hemothorax onset. He also had a history of stroke and was taking cilostazol started 8 years ago.
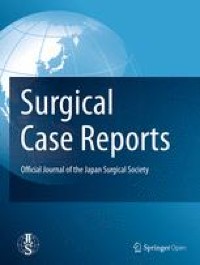
Fig. 2
CT; one month before the onset of hemothorax. The invasive mucinous adenocarcinoma occupies a significant portion of the right lower lobe. The mobility of the lung is extremely limited
As blood pressure increased, bleeding from the incision edge escalated. Given the patient's medical history, it was judged that natural hemostasis would be difficult to achieve. Consequently, we performed surgery under general anesthesia, ligating the dissected lateral thoracic artery, followed by intracavity cleansing and closure. The patient's overall condition stabilized. From visit to the end of surgery, a total of 5.5 h had elapsed, during which fluid and blood transfusions consisting of 12 units of red blood cell (RBC) A type, 10 units of RBC mismatched O type, 16 units of fresh frozen plasma, 20 units of platelets, and 3850 mL of extracellular fluid had been administered.
The patient's medical history was reviewed in detail postoperatively. The CT scan taken one month before onset revealed that the bleeding site of the fifth intercostal artery were almost contact with the staple line from a prior right spontaneous pneumothorax surgery that was performed 11 years before (Fig. 3a–c). Comparing with the contrast-enhanced CT at onset, the bleeding point was consistent with the crossing point of the staple line (Fig. 3d, e). The surgical record at the time revealed that right S6 bullectomy was performed using an endostapler once (Echelon Flex Endopath with a 60 mm blue cartridge; Ethicon, Johnson & Johnson, NJ, USA) without reinforcements or covering materials.
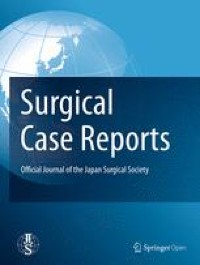
Fig. 3
Relationship between the bleeding site of the fifth intercostal artery and the staple line. a Frontal view, b right anterior oblique view showing the relationship between the staple line (white) and the fifth intercostal artery (light green) reconstructed based on the CT scan from one month before hemothorax onset. c Sequential axial images showing the staple line (blue arrow) and the fifth intercostal artery originating from the aorta (light green arrowhead) crossing each other. d Frontal view, e right anterior oblique view of reconstructed contrast-enhanced CT scan at onset showing the disrupted fifth intercostal artery and the contrast medium leaking into the thoracic cavity. The intact part of the fifth intercostal artery indicated by white line, and the bleeding point indicated by white arrowhead. The staple line from the past pneumothorax surgery aligns with the fifth intercostal artery, and the bleeding point was exactly the same location. Despite a shock vital with BP 50/30 and HR 120, an approximate blood loss of 40 mL/min was measured. All of the contrast medium leaked out at the bleeding point, and the peripheral fifth intercostal artery beyond the bleeding point was not visualized
Postoperative progress was favorable, and the patient was discharged on postoperative day 13 (Fig. 4). Chemotherapy was resumed on postoperative day 26, using DTX monotherapy to avoid bleeding events.
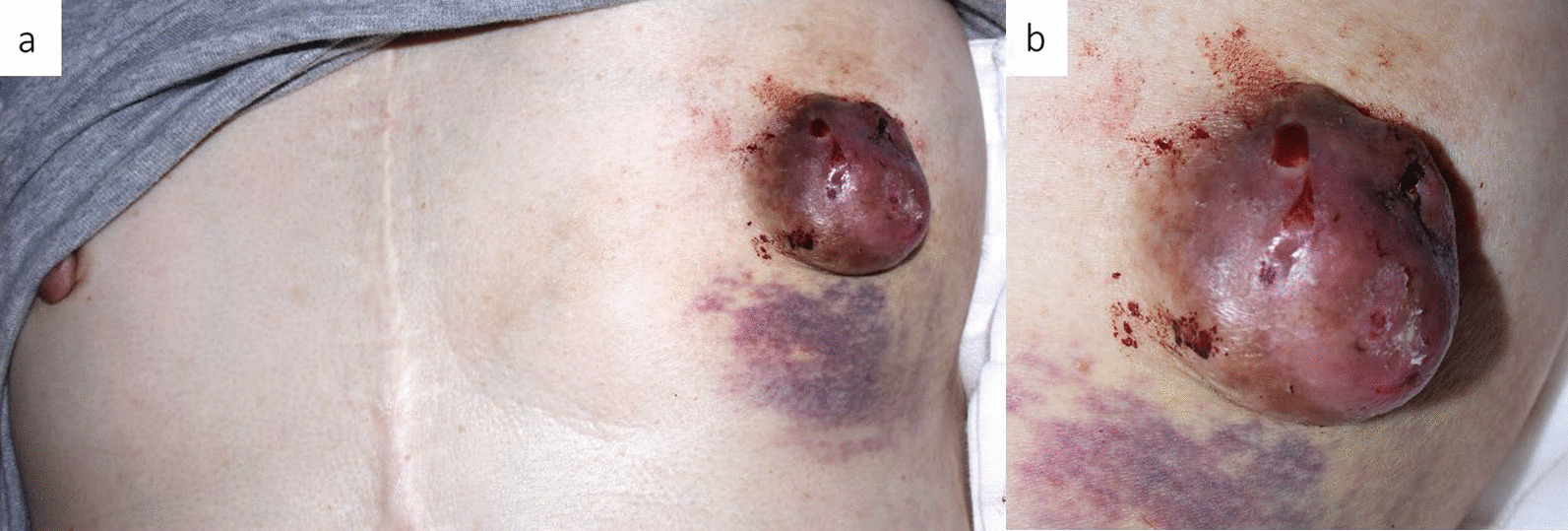
Fig. 4
Postoperative scars. Anterior thoracotomy in the second intercostal space and lateral thoracotomy in the fifth intercostal space are used
留言 (0)