
Remember me






In their seminal paper, “The Concept of Access: Definition and Relationship to Consumer Satisfaction,” Penchansky and Thomas1 propose 5 dimensions of access (ie, affordability, availability, accessibility, accommodation, and acceptability), suggesting a holistic view of access to health care. Their definition of access broadened the policy discussion by encouraging policymakers to acknowledge the importance of nonfinancial aspects of access.2 This is particularly meaningful in the prior context of health policy where affordability (ie, insurance coverage) has long been perceived as a fundamental aspect of access.3 Furthermore, the holistic view on access has critical implications for the implementation of the Affordable Care Act (ACA), which attempts to address both financial and nonfinancial barriers to health care to maximize policy impact.3
Strengthening population access to health care services is a core mission of the ACA.4 In particular, Section 1557 of the ACA highlighted the long-standing prohibition of discrimination in health care access, enhancing Title VI of the Civil Rights Act of 1964. The enactment of Title VI required medical providers under Federal financial assistance to ensure all individuals have access to care regardless of color, sex, age, disability, and national origin.5,6 One notable example is the provision of language services for people with Limited English Proficiency (LEP) who have experienced limited access to health care due to a lack of such accommodation.7–10 Before the ACA, however, no clear implementation of the rules had existed, given that about 30% of hospitals nationwide failed to offer language services.11 Compared to previous legislations, the ACA clarified that such failures might be subject to legal action and further augmented the level of access to LEP services to be “meaningful” for the people with LEP (eg, free of charge, use of qualified interpreters).
Partial compliance of health organizations on the provision of language services may be attributable to a lack of physician awareness and reimbursement policy. A misperception of high cost among physicians restricts their active use of LEP services.12 In fact, the expenses could be trivial compared to the potential gains from reduced resource utilization, and improved quality of care and patient safety.13 The studies by Jacobs and colleagues14,15 report that approximate costs of using in-person and video/phone language services vary between $3 and $79 or $11 and $42 per encounter, respectively. It is also possible that the physicians’ misperception stemmed from challenges of obtaining reimbursement due to the absence of the policy mandating the reimbursement for language services.16 Although the Center for Medicare and Medicaid Services provides higher reimbursement rates for the utilization of the services in expansion states, only 15 states currently offer reimbursement to Medicaid patients since there is no obligation to match the costs by states.17,18
Increased coverage of behavioral health services is another pronounced benefit of the ACA. Through the extension of the Mental Health Parity and Addiction Equity Act of 2008, over 27 million previously uninsured people have gained access to mental health and substance abuse treatment (SAT) services.19 Moreover, following the Medicaid expansion, many behavioral health providers accepted more patients under Medicaid.20 Thus, access to health care may have been improved, vis-à-vis improved affordability and availability, among low-income adults with behavioral disorders in the era of the ACA.21,22
Historically, Medicaid and uninsured populations have experienced a higher rate of mental health and substance use disorders (SUDs) than the general population.23 Therefore, it seems reasonable to hypothesize that demand for behavioral health services would increase in response to the implementation of the ACA, which lowered the cost to access health care services using Medicaid coverage expansion and increased the scope of covered behavioral health services. Specifically, considering that the Medicaid enrollment rates are significantly high in the LEP populations, 74% (ie, 6.4 million out of a total 8.7 million in 2014),24 this group may receive prominent benefits from the increased Medicaid coverages for behavioral health services. However, it is also possible that the expanded insurance coverage may yield only limited impacts on improving access to health care services for the LEP populations if the provision of language services is not guaranteed in behavioral health facilities.
Presently, there is a lack of evidence on the availability of language services and their changes after the implementation of the ACA at behavioral health facilities. In addition, little is known about the policy impact on Medicaid acceptance among these facilities. Therefore, to address these critical gaps in knowledge, we examine the effect of ACA Medicaid expansions on Medicaid acceptance in SAT facilities and the availability of language services using the National Survey of Substance Abuse Treatment Services (N-SSATS) dataset. We test 2 hypotheses: First, the ACA implementation would increase Medicaid acceptance rates among the SAT facilities in expansion states. Second, among the facilities receiving Federal supports (eg, participation of Medicaid programs), availability of the LEP services would also increase in the expansion states due to the legal obligations. This study seeks to deepen our understanding of access barriers to SAT services in low-income LEP populations from an organizational and structural perspective.
METHODS Data SourcesTen waves of data (2010–2019) from the N-SSATS are compiled into a repeated cross-sectional dataset. The N-SSATS, administered annually by the Substance Abuse and Mental Health Services Administration (SAMHSA), is designed to collect information on all US public and private SAT facilities operating specialty units or programs for SUD treatment.25 The characteristics of individual facilities, including facility type, clinical and ancillary services offered (eg, language interpreter), number of clients served, and available payment options are obtained in the survey. The average survey response rates are generally over 90% among the eligible facilities. The N-SSATS is a point-prevalence survey that reflects the information of a facility on the reference date (ie, the end of March). We also use American Community Survey (ACS) 2010–2019 and the University of Kentucky Center for Poverty Research National Welfare Data to illustrate the state-level characteristics, such as the proportion of LEP population and poverty rate.26,27
Outcome MeasuresThe outcomes of interest are 2-fold: availability of SAT services in languages other than English and acceptance of Medicaid patients at the facility. The survey includes multiple questions about whether the facility provides services in different languages through either a staff counselor or an on-call interpreter. Specifically, the first question in the language section of the survey identifies the availability of services in a language other than English at the facility (ie, yes/no). Then, in the second question, respondents select the primary mode of delivering the services from the 3 options: a staff counselor, an on-call interpreter, or both. If the facility offers the language services only via the interpreter, the respondents skip the remaining questions to proceed to the next section; otherwise, they answer questions asking details on languages provided in the facilities (eg, Spanish, Chinese, Native American).
Using the language-related questions in the survey, we further categorize SAT facilities in the sample into 4 groups based on their scopes of language services: (1) interpreter services only; (2) Spanish; (3) other languages; and (4) both Spanish and other languages. It is important to note that the publicly accessible N-SSATS dataset does not include information on the primary mode of language services. Therefore, we operationalize the facilities providing the language services through on-call interpreters only using questions that summarize the availability of different languages. For example, despite their count of any languages being offered in the facility being zero, when observations have “yes” in the question on the availability of services in a language other than English, they are identified as the facilities with interpretation services only.
To determine the availability of Medicaid as a payment source at the facility, we use the questions that report the types of payments and insurance being accepted by the facility. Since each payment source (eg, Medicare) counts a single variable in the dataset, we focus on the binary variable indicating Medicaid acceptance.
Medicaid ExpansionsWe group the facilities by their ACA implementation status since 2014 (ie, 2014, 2015, 2016, 2019, and nonexpansion), matching the implementation dates for each state to the N-SSATS survey day of the corresponding years (ie, March 31 of each year).28 We characterize the 6 states that expanded their Medicaid programs between 2010 and 2013 (California, Connecticut, Minnesota, New Jersey, Washington, and the District of Columbia) based on the year of ACA implementation since our focus is to assess its comprehensive effects.29
Statistical AnalysisTo analyze the annual trend of availability of language services in SAT facilities, we calculate the proportion of each of the 4 language service categories (ie, interpreter services only, Spanish, other languages, and Spanish and other languages) from 2010 through 2019. Moreover, we graph these proportions at the state level, comparing the period before and after the ACA implementation to identify the variability of language services offered in the facilities across the states. For nonexpansion states, we use 2014 as a baseline year for comparison.
We estimate a difference-in-differences (DiD) model with staggered treatment timings using Callaway and Sant’Anna’s (CS) estimator.30 Their DiD estimator allows us to avoid the issues with the classical two-way fixed effects (TWFE) approach when measuring the treatment effects of policy events spanning multiple time periods.31 Interpretation of TWFE estimator can be unintuitive because the TWFE estimator (ie, a weighted average of multiple 2-by-2 estimators) would include 2-by-2 estimators with negative weights. The DiD estimators developed by Callaway and Sant’Anna are robust to variations in treatment timings and dynamic treatment effects, thereby producing unbiased average treatment effects.30,32
We use a DiD linear probability model specification with standard errors clustered by state. Estimates from the DiD models are presented based on the event study framework in the following equation:
Yi,s,t=θs+τt+∑lμl1+Fi,s,tα1+Si,s,tα2+εi,s,t.
The dependent variable, Yi,s,t, is an indicator for the availability of language services or Medicaid acceptance in facility i in state s by year t. The variable Ei indicates the year of implementing the ACA. The coefficients, μl, are estimated differently depending on the years before and after the event. For instance, for t≥Ei, a reference period is Ei−1 (ie, −1 on the x-axis of the event study plot), whereas for t<Ei, the preceding year t−1 is used for a reference period. It is worth noting that unlike the classical TWFE event studies that use an omitted base period to anchor the differences between treatment and control groups at 0, the CS estimator does not require such a process. Fi,s,t is a vector of facility-level characteristics, such as ownership (for-profit/nonprofit), types (hospital/residential/outpatient) and Medicare and/or Medicaid acceptance. Si,s,t is a vector of state-level characteristics, such as proportions of Black, Hispanic, Asian, and Governor’s political party. Note that we also control the state-level characteristics separately by the outcomes—proportions of LEP population and college graduates for the language service availability and poverty and unemployment rates for Medicaid acceptance. Including state-level characteristics helps us further control confounding from different levels of exposure to socioeconomic factors across states.
We aggregate group-time average treatment effects from the DiD models by groups with the same ACA implementation year to identify heterogenous effects across groups. Additionally, we present simple weighted average results from the models. The states that never implemented the ACA as of 2019 (ie, the never-treated group) are served as the comparison group. For the language service availability outcome model, we restrict our analysis to the sample consisting of the only facilities under Federal assistance (ie, the SAT facilities accepting payments from Medicare, Medicaid, or Federal military insurance).
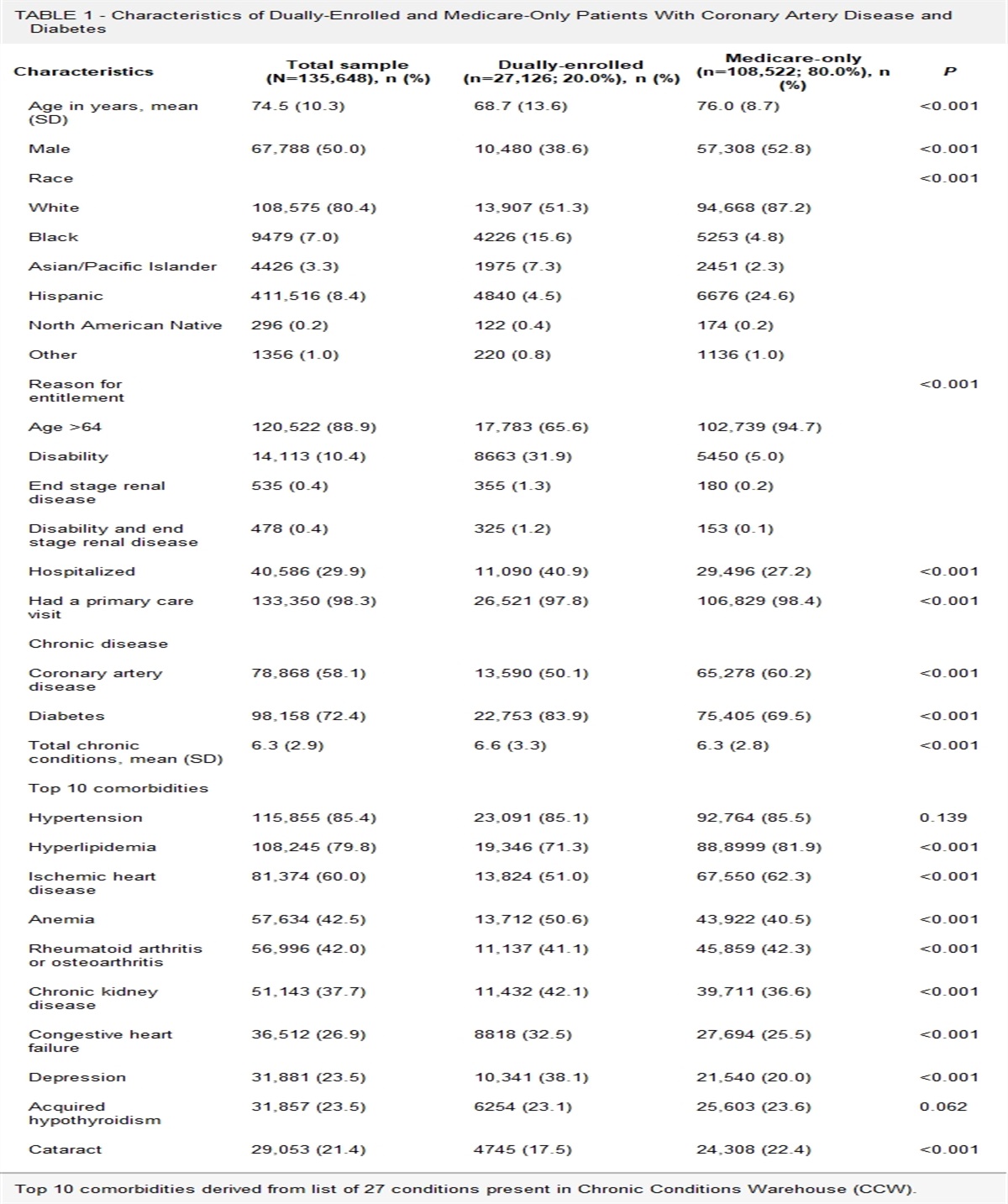
RESULTS Sample CharacteristicsThe total number of SAT facilities included in the study sample is 140,776 (Table 1). Nonexpansion states have a higher proportion of for-profit facilities and hospitals than expansion states. Regarding state characteristics, nonexpansion states have a lower proportion of LEP populations and Democratic governors than their counterparts.
Table 1 - Comparison of Facility and State Characteristics Between Medicaid Expansion and Non-expansion States Expansion states 2010-2013 Expansion states 2014-2019 Non-expansion states 2010-2013 Non-expansion states 2014-2019 N (Total: 140,776) 39,381 61,182 15,450 24,763 Facility characteristics (%) Ownership For-profit 29 34 37 42 Not-for-profit 71 66 63 58 Type Hospital 12 11 17 16 Residential 17 16 13 13 Outpatient 72 73 70 72 Insurance acceptance Medicaid 58 65 58 61 Medicare 34 36 32 33 LEP service Interpreter only 13 21 20 27 Spanish 20 20 16 18 Other 2 2 1 1 Spanish and other 7 5 4 3 Total 41 48 40 49 State characteristics (%) Race/Ethnicity Black 11 11 16 16 Hispanic 16 16 14 15 Asian 7 8 3 3 Education/Economy/Policy LEP population 9 8 6 6 College graduate 30 33 26 29 Poverty rate 14 12 15 13 Unemployment rate 9 5 8 4 Democratic governor 63 59 21 11LEP indicates Limited English Proficiency.
The proportion of SAT facilities that provide services in languages other than English continues to increase from 40% in 2013 to 53% in 2019 (Fig. 1). Specifically, this trend is primarily attributed to the increase in interpreter services, which almost doubled in 2019 compared to the pre-ACA period (ie, from 14% to 27%). The proportions of other categories, such as Spanish, other languages, and both Spanish and other languages, remain constant throughout the study period.
 FIGURE 1:
FIGURE 1: Annual trend of proportions of language service availability in substance abuse treatment facilities 2010–2019.
In Figure 2, we observe that the proportions of the facilities providing their services in different languages (all 4 groups) are heterogeneous across states, ranging from approximately 20% to 70%. Every state experienced an increase in the proportion of facilities offering language services after the ACA (ie, after 2014 for nonexpansion states) but Utah. The states with the highest and lowest proportion are New Mexico and Massachusetts (69%) and North Dakota (20%), respectively, both of which mandated Medicaid expansion in 2014. In addition, we find opposing patterns in the Spanish (ie, aggregated with the Spanish and other languages category) and interpreter services category (Figures A1, Supplemental Digital Content 1, https://links.lww.com/MLR/C729 and A2, Supplemental Digital Content 2, https://links.lww.com/MLR/C730). First, while nearly half of states experienced a slight decline in their proportion of facilities providing services in Spanish after ACA, the proportion of facilities providing interpreter services increased in all the states after ACA. Second, the proportion of the Spanish category is generally lower than 25% among nonexpansion states with a few exceptions, such as Utah, Florida, and Texas. In contrast, in the proportion of interpreter service category, more than half of nonexpansion states record over 30% after the ACA.
 FIGURE 2:
FIGURE 2: Comparison of proportions of substance abuse treatment facilities providing services in languages other than English by state before and after Affordable Care Act (ACA) implementation. The year of 2014 is a baseline year for nonexpansion states.
Effects of Medicaid ExpansionsResults from the weighted averages of the group-time treatment effects indicate that the ACA Medicaid expansions are not associated with changes in the availability of language services in SAT facilities with Federal financial assistance. Medicaid acceptance in the expansion states increased by 4.9 percentage points (P<0.05) after the implementation of ACA in the parsimonious model. When adjusting facility and state characteristics, however, the effect is attenuated with deleting statistical significance (Panel A in Table 2).
Table 2 - Effects of Medicaid Expansions on Language Service Availability and Medicaid Acceptance in SAT Facilities 2010-2019 Language services Medicaid Model 1† Model 2‡ Model 1† Model 2‡ Panel A: Simple weighted average Medicaid expansion −0.025 −0.019 0.049* 0.026 (−0.07, 0.02) (−0.08, 0.042) (0.012, 0.086) (−0.033, 0.085) Observations 98,544 98,544 140,776 140,776 Panel B: Event study Expansion year −0.021 −0.017 0.006 −0.02 (−0.051, 0.009) (−0.11, 0.076) (−0.028, 0.04) (−0.147, 0.107) 1 year post expansion −0.026 −0.032 0.028 0.001 (−0.072, 0.02) (−0.113, 0.049) (−0.023, 0.079) (−0.143, 0.145) 2 years post expansion −0.027 −0.029 0.038 0.016 (−0.09, 0.036) (−0.178, 0.12) (−0.021, 0.097) (−0.056, 0.088) 3 years post expansion −0.016 0.006 0.057 0.045 (−0.087, 0.055) (−0.08, 0.092) (−0.004, 0.118) (−0.041, 0.131) 4 years post expansion −0.019 −0.008 0.075* 0.067 (−0.098, 0.06) (−0.089, 0.073) (0.019, 0.131) (−0.034, 0.168) 5 years post expansion −0.044 −0.036 0.099* 0.055 (−0.15, 0.062) (−0.187, 0.115) (0.043, 0.155) (−0.07, 0.18) Observations 98,544 98,544 140,776 140,776 Panel C: Group-specific effects 2014 −0.032 −0.022 0.052* 0.027 (−0.089, 0.025) (−0.094, 0.05) (0, 0.104) (−0.042, 0.096) 2015 0.013 −0.007 0.028 0.024 (−0.06, 0.086) (−0.158, 0.144) (−0.085, 0.141) (−0.08, 0.128) 2016 0.037 0.049 0.061* 0.061 (−0.269, 0.343) (−0.226, 0.324) (0.026, 0.096) (−0.008, 0.13) 2016 (LA)c −0.076* 0.036 0.004 −0.021 (−0.108, −0.044) (−0.19, 0.262) (−0.015, 0.023) (−0.062, 0.02) 2019 −0.04 −0.083* 0.017 −0.123 (−0.081, 0.001) (−0.139, −0.027) (−0.006, 0.04) (−0.392, 0.146) Observations 98,544 98,544 140,776 140,776*Indicates 95% confidence interval does not cross 0. Never treated group is used as the control group. SAT; substance abuse treatment.
†Covariates are not included in the model (i.e., unadjusted model).
‡Covariates, facility-level and state-level characteristics, are adjusted in the model.
§Since the Affordable Care Act (ACA) was effective on July 1, 2016 in Louisiana (LA), we separate this state from other states that implemented the ACA in the early 2016 given the survey timing, March 31, 2016.
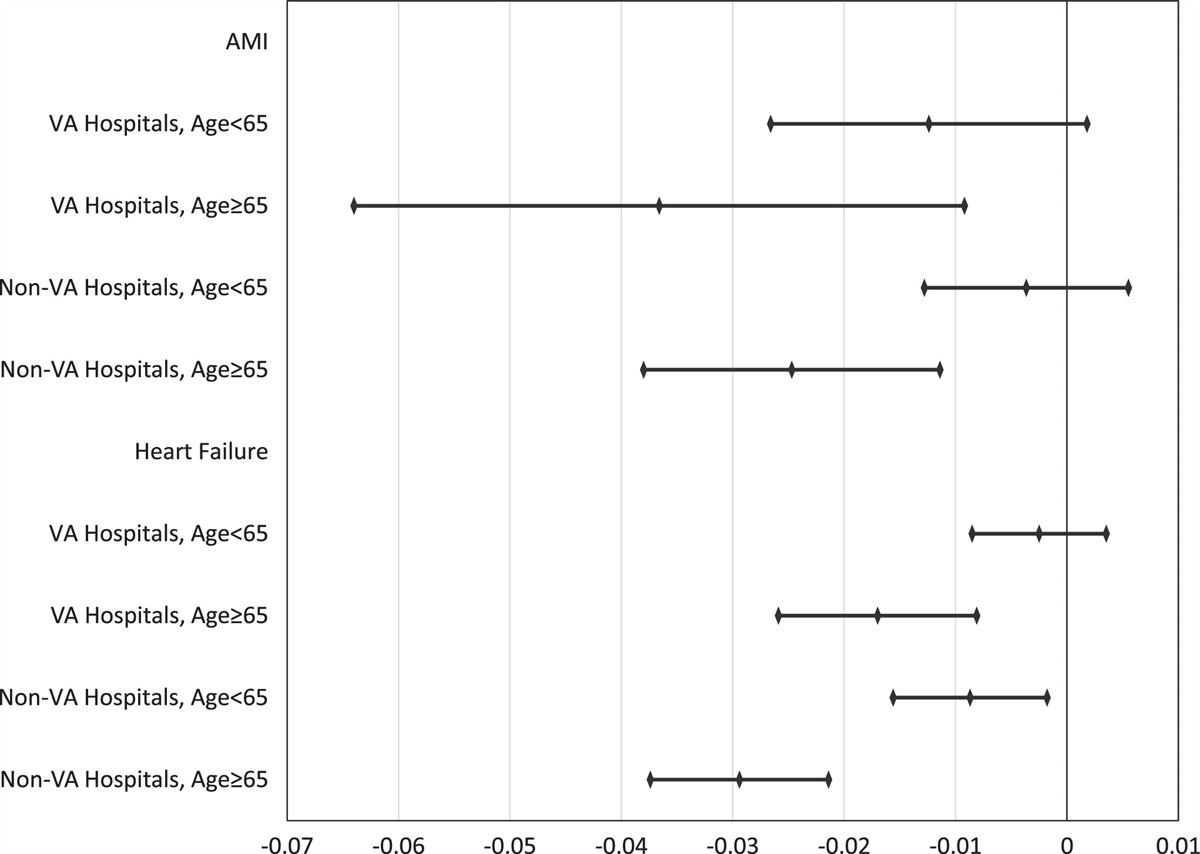
Estimates from the event study provide detailed information on the dynamic effects of the policy (Panel B in Table 2). The event study plot (Fig. 3A) suggests the parallel trends assumption holds for the DiD models for language service availability and Medicaid acceptance. Moreover, the results of a Wald pre-test of the assumption confirm the visual inspection. There are no statistically significant trends observed from the language service and Medicaid models with facility and state characteristics controls. Yet, we notice that estimates of Medicaid acceptance in the expansion states generally increased after the ACA implementation.
 FIGURE 3:
FIGURE 3: Effects of Medicaid expansion on language service availability and Medicaid acceptance in substance abuse treatment facilities 2010–2019 (A: event study plot, B: group-specific effects). The never-treated group is used as the control group. ACA indicates Affordable Care Act.
Results of group-specific effects demonstrate a mixed pattern for both availability of language services and Medicaid acceptance (Panel C in Table 2, Fig. 3B). The SAT facilities in states that adopted the ACA in 2019 decreased their provision of language services by 8.3 percentage points (P < 0.05) compared to those in nonexpansion states.
Sensitivity AnalysisWe conduct multiple sensitivity analyses to evaluate the robustness of our findings. First, to address the issue of the event study with different compositions of the groups in each period of exposure to the event, we restrict our sample based on length of exposure (ie, 2 to 5 years postexpansion). The results from this exercise are comparable to the prior findings (Tables A1, Supplemental Digital Content 3, https://links.lww.com/MLR/C731 and A2, Supplemental Digital Content 4, https://links.lww.com/MLR/C732). Second, we repeat the main analysis with a different control group replacing the never-treated group with the “not-yet-treated” group. Overall, the results are compatible with our primary estimates (Table A3, Supplemental Digital Content 5, https://links.lww.com/MLR/C733 and Figure A3, Supplemental Digital Content 6, https://links.lww.com/MLR/C734). Third, we additionally adjust the facility size with the number of patients on the survey reference date. Since the N-SSATS did not collect the patient count information in 2014 and 2018, we omitted the samples from these 2 years. Adjusting the patient count information has no influence on our prior interpretation of the results (Table A4, Supplemental Digital Content 7, https://links.lww.com/MLR/C735). Fourth, to capture potential delays in state policy adoption, we perform the same analysis after dropping the years of ACA implementation for each group. Similarly, this exercise does not lead to different consequences (Table A5, Supplemental Digital Content 7, https://links.lww.com/MLR/C735). Fifth, we compare estimates from the main analysis to those from the conventional TWFE approach. We observe that overall effects are analogous to each other, although there is statistical significance for some of the estimates from the TWFE model only (Table A6, Supplemental Digital Content 7, https://links.lww.com/MLR/C735).
DISCUSSIONOur results demonstrate that ACA Medicaid expansion did not increase the availability of language services and Medicaid acceptance in SAT facilities. Regarding the decrease of language service availability in states that implemented the ACA in 2019, it may reflect facilities’ economic behaviors prioritizing services with higher margins, thus allocating less resources to unprofitable services (eg, language services), to make up for the potential loss from Medicaid patients. However, this scenario is less likely because Medicaid acceptance in these states was also reduced following the policy implementation. Given the reference date of the survey, the end of March, it seems premature to determine the impacts of the ACA implementation for this group based on the 3 months period in the sample.
Interpretation of the findings on the availability of language services and Medicaid acceptance in the SAT facilities requires caution. Importantly, our findings do not preclude potential benefits of the ACA Medicaid expansion on language service availability despite the null effects from the DiD models. For example, the proportion of SAT facilities offering LEP services has increased yearly since 2014 (Fig. 1), and service availability expanded after 2014, albeit in the nonexpansion states (Fig. 2). Therefore, we consider this null policy effect as the positive spillover of the ACA Medicaid expansion to the nonexpansion states rather than nonadherence to the policy in the expansion states. Also, it is conceivable that a higher proportion of facilities in the expansion states had already complied with the requirements prior to the enactment of ACA. Regarding the Medicaid acceptance outcome, CS and TWFE estimators produced different implications for the policy impact—that is, their magnitude of the estimates is similar, but results of 95% confidence intervals do not lead to the same conclusions (Table A6, Supplemental Digital Content 7, https://links.lww.com/MLR/C735). Given the advantage of the CS estimator over the TWFE estimator in the multiple time periods setting, the null outcomes from the former model could be more reliable than those from the latter model.30
The evidence from our study provides a clue to the previous findings on the impact of ACA on health care utilization among people with SUDs.33,34 The studies by Creedon and Cook and Olfson and colleagues show that the ACA Medicaid expansion has no effect on the utilization of SAT services despite the increase in the insurance coverage of people with SUDs. Based on Penchansky and Thomas’s proposal on access, increased Medicaid coverage only (ie, affordability) may be less sufficient to facilitate the use of SAT services among low-income adults with SUDs. It is possible that a lack of accessibility and acceptability hampers their access to SAT services. Our findings affirm that secured access to SAT services cannot be achieved merely through expanding the insurance coverage if without a simultaneous increase in Medicaid acceptance in the facilities. However, it should be noted that our findings based on the N-SSATS are limited to specialty treatment programs owing to the limitation of data. Thus, we expect future studies may further investigate access to SAT services via other providers, such as primary care physicians, given their active participation in treatments for people with SUDs.35
Presently, although facilities are mandated to ensure accessibility to services for LEP patients, they have significant flexibility over their scope of services. There is no explicit national requirement guiding the mandated collection of information related to accessibility for LEP patients; however, national surveys such as the N-SSATS managed by SAMHSA do collect some information on accessibility for LEP. Yet, it is important to note that N-SSATS is a voluntary survey, so there are potential disincentives for facilities to report if they miss their accessibility benchmarks.
Recognizing this systemic surveillance challenge, the Department of Health and Human Services (HHS) recently proposed relaunching its Language Access Steering Committee to meet language accessibility obligations outlined in recent executive action from the Biden-Harris administration and the HHS Equity Access Plan.36,37 Furthermore, the Department of Justice has recently submitted a memo directing the Civil Rights Division to hire a language access coordinator in an effort to improve the monitoring of language accessibility across all federal agencies.38 While this is an incredible step to ensure the mandates under past executive orders, the Civil Rights Act and the ACA are being enforced, it does not yet direct punitive action to be taken against offending institutions. That all being said, this is an important step in improving surveillance toward the goal of improving language accessibility for patients with LEP.
Our study has several limitations. First, the N-SSATS does not provide facility-level identifiers; therefore, we could not disentangle whether the observed effects were derived from existing providers or providers entering and leaving the market. Second, relatedly, we could not control community-level socioeconomic characteristics reflecting heterogeneous needs for LEP services across the service areas of facilities. This limitation hinders our ability to determine the effectiveness of the availability of LEP services based on local needs and circumstances. Third, it is possible that interpretation services are offered by persons other than staff counselors or on-call interpreters, such as community health workers. However, this is unlikely to impact our analysis due to our use of a study design that focuses on the presence of certified medical interpreters. Fourth, this study only focuses on the availability of interpretation services on an extensive margin (ie, available vs. not available) and does not examine the number of staff counselors due to data limitations. Last, the facilities offering interpreter services were identified indirectly, thus, our estimates are subject to bi
Comments (0)