Our study highlighted the epidemiological and clinical features of HF in a Tunisian care center. This pathology mainly affects elderly and male subjects. Patients are seen at an advanced stage of HF. We noted a predominance of ischemic etiology, and a satisfactory rate of the triple combination (BB + MRA + ACEi). However, the optimal doses were not reached, and the prescription of new molecules recently prescribed (SGLT2i and Sacubitril/Valsartan) was low and few patients were on the 4 molecules as recommended in ESC guidelines. It also revealed our deficiency in patient care, in particular the readaptation and the realization of cardiac transplantation. We demonstrate also a poor prognosis with huge mortality and iterative rehospitalizations.
The mean age of heart failure was 70 years in Framingham study [5]. Other studies reported an average age of patients at the time of HF diagnosis of 65–75 years [6,7,8,9]. In our series, the average age of our patients was comparable to that reported in these different studies: 64 years. It was similar to the average age found in our NATURE-HF register with an average age of 63.6 years [4].
The predominance of males was reported in several studies [10, 11]. In our study, 73.8% were male which is concordant with the results of NATURE-HF (70.9%) [4] and the European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT)(71.2% for chronic heart failure and 62.6% for acute heart failure) [12].
The major cardiovascular diseases associated with heart failure were smoking, hypertension, and diabetes. In fact, two-thirds of patients with HF have a history of hypertension [12]. Using data from the Framingham cohort, Levy [13] showed that the risk of heart failure was mainly linked to hypertension and myocardial infarction in men, and to myocardial infarction and diabetes in women. In our study, we found a rate of 48% of hypertensive patients joining our national register which reveals a rate of 42.1% [4]. Diabetic patients were at risk of developing heart failure regardless of coronary lesions [14]. The Framingham study showed that diabetic patients were twice at risk of developing HF in men and five times at risk in women [5]. In our NATURE-HF registry, the rate of diabetic patients was 37, 8% [4] and in our series, we found a high rate of 48%. 50% of patients were smokers in our study, and a lower rate was found in our NATURE-HF register [4] (27.3%) and in ESC-HF-LT (11.2% for chronic heart failure and 16% for acute heart failure) [12].
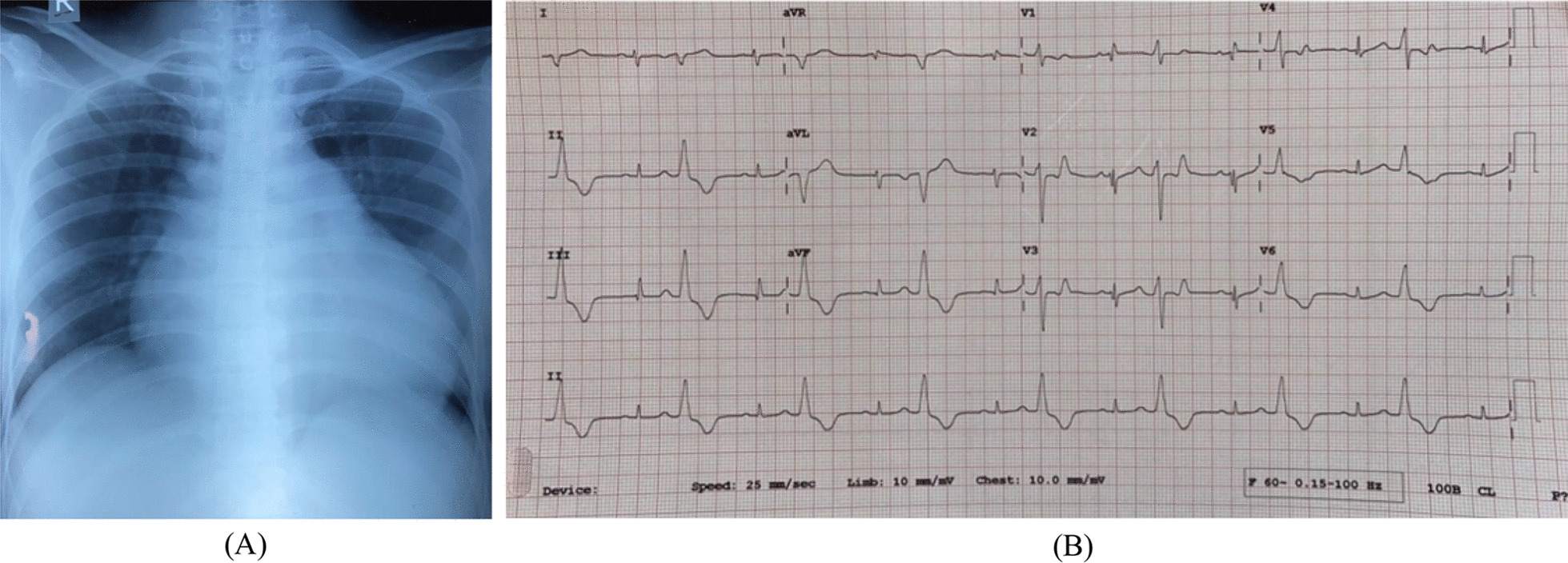
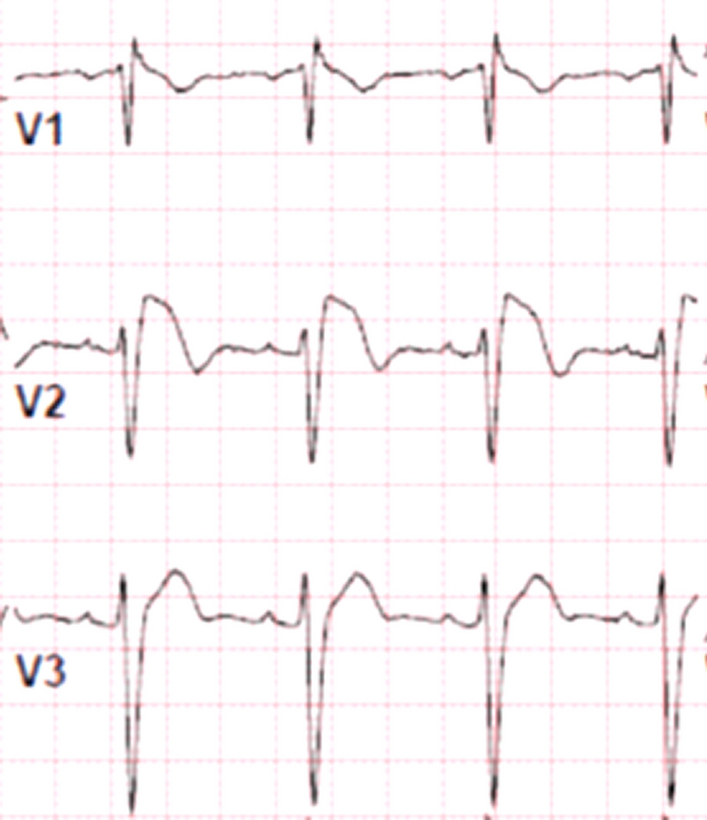
In the literature, the average HR reported was 82 ± 21 according to Gotsman [15] and 93.5 ± 25 according to Macin [16], It was 90.82 ± 25.27 for acute heart failure and 72.7 ± 15.29 for chronic heart failure in ESC-HF-LT [12] and 96 ± 20 bpm in our study series joining our NATURE-HF registry where the mean HR was around 80 ± 17 bpm [4]. AF is the most common arrhythmia seen in heart failure. A frequency ranging from 23 to 40% has been reported in the literature [17, 18]. It was observed in 40% of patients in our series, 30.6% according to our NATURE-HF register [4], 44% in acute heart failure, and 37.7% in chronic heart failure in ESC-HF-LT [12].
LBBB was a frequently noted sign during heart failure [19]. It was observed in 40.6% of patients in Macin's study [16]. We reported a rate of 28.5% in our study. It was higher than the rate in the NATURE-HF register, which was around 11.1% [4].
In our study, 28.5% of patients were anemic, approaching the rate found in our NATURE-HF register, which was 23.6% [4] while 47% in REPORT-HF [20].
In Western countries, coronary disease was the most common cause of heart failure in 60–70% of cases [21]. It is followed by hypertensive disease (20–30%), cardiomyopathy (5–10%), and valvular disease (3–10%).
In our NATURE-HF registry, ischemic etiology was observed in 52.4% followed by primary DCM with a rate of 15.5%, valvular heart disease with 9.9%, and HCM 1.3% [4].
In ESC-HF-LT [12], ischemic heart disease was seen in 53.8% of acute heart failure and in 43% of chronic heart failure, and in 48% in REPORT-HF [20].
The prevalence of renal deficiency in patients with heart failure was around 26% in ESC-HF-LT [12]. This is also found in our series where 22.8% of patients had renal failure concordant with the rate found in our NATURE-HF register: 25% [4].
Over the last 20 years, HF management has been codified thanks to recent updates of European recommendations of 2021 and the American guidelines. In our study, the most commonly used drugs were diuretics (mainly furosemide), angiotensin-converting enzyme inhibitors (ACE-I), beta-blockers (BB), mineralocorticoid receptor antagonists (MRA), Sodium-glucose cotransporter 2 inhibitors (SGLT2i) and Sacubitril/Valsartan.
In Mahler's study including patients with HFrEF from six European countries, 87% of patients received an ACE Inhibitor or an Angiotensin Receptor Blockers (ARB) [22]. Comparable rates have been observed in the multicentric study ESC-HF Pilot [23] including 5118 patients with heart failure where ACE Inhibitors or ARBs were prescribed in 88.5%, BB in 86.7%, Spironolactone in 43.7% and loop diuretics in 82.8%. Higher rates than those reported in this study were observed in our series, in fact, ACE Inhibitor or ARBs were prescribed in 86.6%, BB in 88.6%, and Spironolactone in 35, 7%. In our National nature-HF register, there were rates similar to our study with ACE inhibitors prescribed at 80.5%, BB at 80%, and Spironolactone at 50.5% [4]. According to the REPORT-HF [20], 70% of patients were on ACE inhibitors, 86% on loop diuretics, 76% on BB, and 59% on MRA.
In our study, the triple combination ACEI + BB + MRA was prescribed in 75 patients (35.7%). The quadruple combination (ACEI + BB + MRA + SLGT2i) was prescribed in 17 patients (8.1%).
The prescription of drugs for HF is not optimal as the prescription of the triple combination was only 35% in the ESC-HF Pilot [23] and the number of patients treated with appropriate doses was low. Different factors have been identified to explain this including age, sex, and comorbidities, especially renal deficiency. In our study, the recommended optimal doses for each class were reached only in 21 patients (10%) for ACE-I, in 30 patients (16%) for BB, and in 15 patients (20%) for MRA. ACEi/ARB/ARNi was prescribed in optimal dose in 22% of low-income countries vs. 28% in high-income countries β-blockers in 7% of low-income countries vs. 32% in high-income countries and MRA in 14% of low-income countries vs. 9% in high-income countries in the REPORT-HF [24]. The non-optimal treatment was explained in our study by arterial hypotension, worsening renal function, and exacerbation of heart failure symptoms in some patients.
In our study, only Captopril and Bisoprolol were used as drugs. This can be explained by the fact that these two drugs are provided by the hospital and are part of the hospital formulary.
Despite their effect proven in several studies on mortality and rehospitalization in heart failure [25, 26], we noted a reduced prescription of Sodium-glucose cotransporter 2 inhibitors (SGLT2i) or Sacubitril/Valsartan. Besides, in the Nature-HF register, 0.2% of patients were on Sacubitril/Valsartan, and no patients were on SGT2i [4].
This can be explained by the fact that the registry was conducted before the introduction of SGLT2i in our country and Sacubitril/Valsartan was newly introduced.
The number of patients under quadruple combination and triple combination decreased after 1-year follow-up from 8 to 7.8% and from 35 to 26% respectively. 37% of patients were on the triple combination at discharge and 34% at 6 months of follow-up in the REPORT-HF [24].
Non-pharmacological treatment that can improve the prognosis (resynchronization and defibrillator) remains weak. Indeed, in our study cardiac resynchronization was performed only on 30 patients (9%) and implantable cardioverter defibrillator on 15 patients; The explanation for the non-implantation of these devices were: patient refusal, problems of logistics and cost, and low percentage of patients eligible for resynchronization. Cardiac transplantation is not often performed due to its high economic cost and its logistical problems. No case of transplantation was reported in our study.
Strong evidence from clinical trials and meta-analyses indicates that physical training improves exercise tolerance and quality of life in patients with heart failure. Moreover, several meta-analyses suggest that it reduces hospitalizations for all causes, including heart failure, although uncertainty remains regarding its effects on mortality [27].
In the Framingham study [5], which included 652 subjects, the median survival duration was 1.66 years for men and 3.17 years for women. Survival rates at 1, 2, 5, and 10 years were 57%, 46%, 25%, and 11%, respectively, for men, and 64%, 56%, 38%, and 21%, respectively, for women. The age-adjusted mortality rate, or more precisely, fatality rate, was lower in women than in men. Mortality rates increased with age in both sexes, by 27% per decade in men and 61% per decade in women.
In our study, hospital mortality was around 3.8%, comparable to that reported in other registers where it varied from 4 to 7% [28]. The Alarm-HF study [29] reported higher hospital mortality (11%).
Mortality at 1 year was around 19.8% in our study, 13% in our National Nature-HF register [4], and 23.6% among acute heart failure patients in ESC-HF-LT [12]. It was 20% in REPORT-HF [20].
The rate of readmission at 1 year in our study was around 42.2%, this rate is almost comparable to that noted in the Astronaut register: 27.6% in North America and 22.5% in Western countries [30].
Many studies have reported the ischemic origin of heart failure as an unfavorable prognostic factor [31]. We should note that precipitating factors can influence rehospitalization and mortality rates.
Our study has demonstrated that the distribution of readmissions over 1 year is unequal, with the highest rate occurring in the first 3 months at 61.73%, and this rate decreases over time. Similar findings have been observed in other studies: Wideqvist et al. found that 60.1% of readmission rates occurred in the first quarter, 17.2% in the second quarter, 15.4% in the third quarter, and 7.3% in the fourth quarter [32].
This rate of mortality can be explained by the lack of use of new drugs which has demonstrated their efficacy in reducing mortality and rehospitalizations, in addition to the non-optimization of doses of medical treatment, the weak implantation of devices, and the absence of cardiac rehabilitation.



Comments (0)