RHD is the long-term effect of ARF, which is brought on by an autoimmune response to an infection with Group A beta-hemolytic Streptococcal (GAS). Poor hygiene, a crowded home, and limited access to quality medical care are among the predisposing factors that are frequently present in middle-class and lower-class populations [7]. This report illustrates the case of latent RHD due to echocardiographic proof of RHD but no documented history of ARF. Until it manifests in adulthood, latent RHD is typically clinically quiet. More severe RHD consequences, such as heart failure are commonly seen in adults which made the patient admitted to the hospital [7].
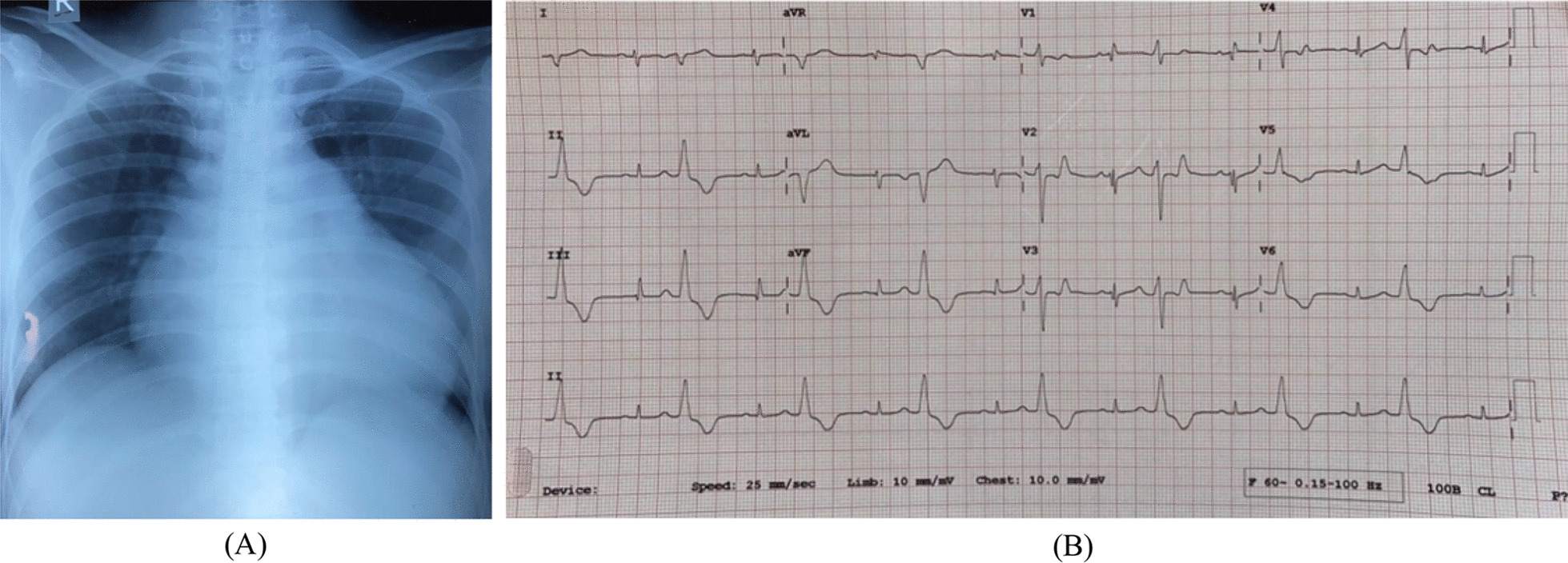
Tricuspid regurgitation may arise from an inherent flaw in the valve itself or, more frequently, as a result of an associated issue with the MV. Tricuspid regurgitation rarely occurs alone and is often not detected or causing any symptoms. Patients typically seek medical attention with the onset of heart failure symptoms. Despite normal left-sided valve function, pulmonary pressures, and LV systolic performance, patients with isolated severe TR will have RHF. Increased central venous pressure, visible jugular vein distension, and may occur in organ dysfunction as well as peripheral edema or ascites following the presentation of right heart failure due to backward failure [8]. Right ventricular failure causes systemic congestion due to blood flow issues. Severe cases cause the right side to expand, inhibiting the LV function, resulting in forward failure with low blood pressure and inadequate flow [4, 9]. Exertional dyspnea is caused by low effective operating compliance of the LV due to heightened ventricular interaction with dilated RV. Low perfusion pressure and venous congestion lead to hepatic and renal failure, which demonstrates elevated SGOT, SGPT, urea, and creatinine levels. In cases of chronic RV failure, ECG typically displays RAD due to the enlargement of the RV [8].
Rheumatic carditis is a condition that is marked by inflammation of the endocardium, specifically the valvular endocardium. The predominant manifestation of carditis is the inflammatory condition of the endocardium, which is characterized by valvulitis. Valvulitis primarily affects the mitral valve, resulting in MR [10]. The occurrence of isolated right-sided cardiac valve involvement, particularly TR, without any accompanying MV disease that results in RV failure, is an exceptionally rare discovery, especially during screening. As a result, it is excluded from the guidelines [6].
Due to the high sensitivity of echocardiography, carditis can be ruled out in a patient with a murmur if there is no regurgitation on color Doppler. Furthermore, echocardiography can easily identify murmurs brought on by endocarditis, congenital anomalies, or myxomatous mitral valve disease. The Jones criteria and echocardiogram were concordant (both positive or both negative) 83% of the time in a study of 333 patients with suspected clinical carditis. Patients with “subclinical” or “latent” carditis, in whom an echocardiogram shows characteristics suggestive of valvulitis but the clinical examination is negative, are the subject of controversy. In the Utah outbreak, only 14 out of 74 individuals (19%) had carditis found by echocardiography. Seventeen percent of patients in a meta-analysis with 1700 cases had subclinical carditis as their occurrence. The primary cause of the notable variations in study results is the use of different echocardiographic standards to diagnose carditis. The WHO criteria are as follows: (1) regurgitant jet length > 1 cm; (2) regurgitant jet visualized in at least two planes; (3) mosaic jet with peak velocity > 2.5 m/s; and (4) pansystolic mitral or pandiastolic aortic regurgitation. However, some have suggested raising the minimum jet length of mitral or aortic regurgitation to 2 cm to increase specificity; and still others require additional morphological valvular abnormality to decrease the number of carditis diagnoses [11].
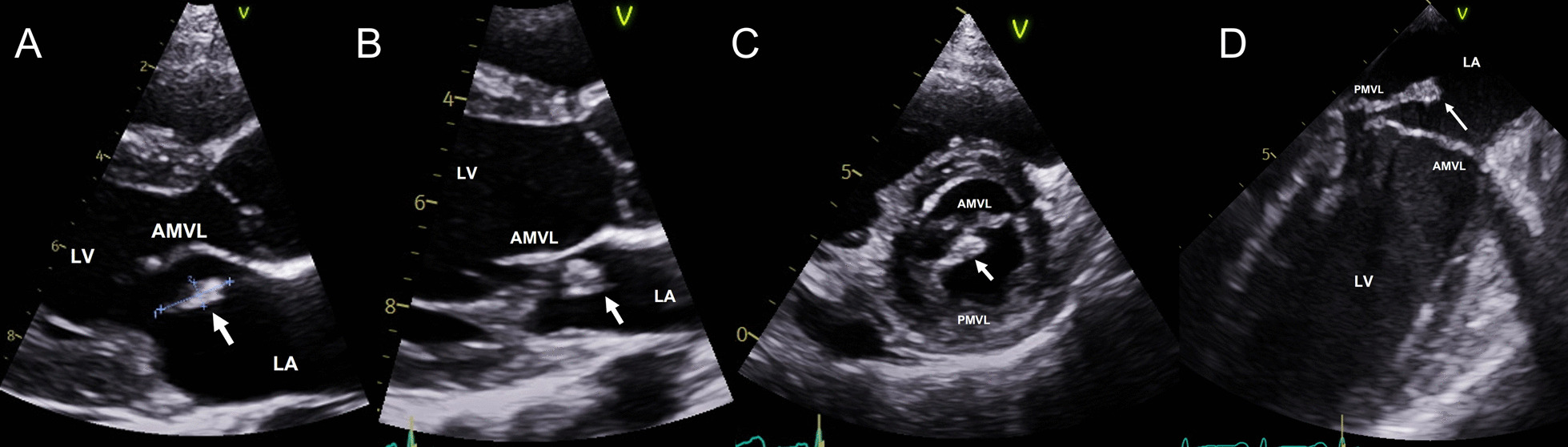
Ten percent of adult instances of TR are related to primary valvular disease. Myxomatous prolapse, atrioventricular abnormalities, and Ebstein’s abnormality are examples of primary TV illnesses that can occur in patients with congenital disease. Trauma-induced flail leaflets, carcinoid, rheumatoid arthritis, and endocarditis are examples of acquired primary diseases [8, 12]. Echocardiography revealed no congenital heart anomalies or primary pulmonary hypertension as the cause. Instead, we discovered IRTR with thickened leaflets, calcification of all leaflets, and partial prolapse posterior leaflets in the nonsignificant abnormalities in the other valves [13].
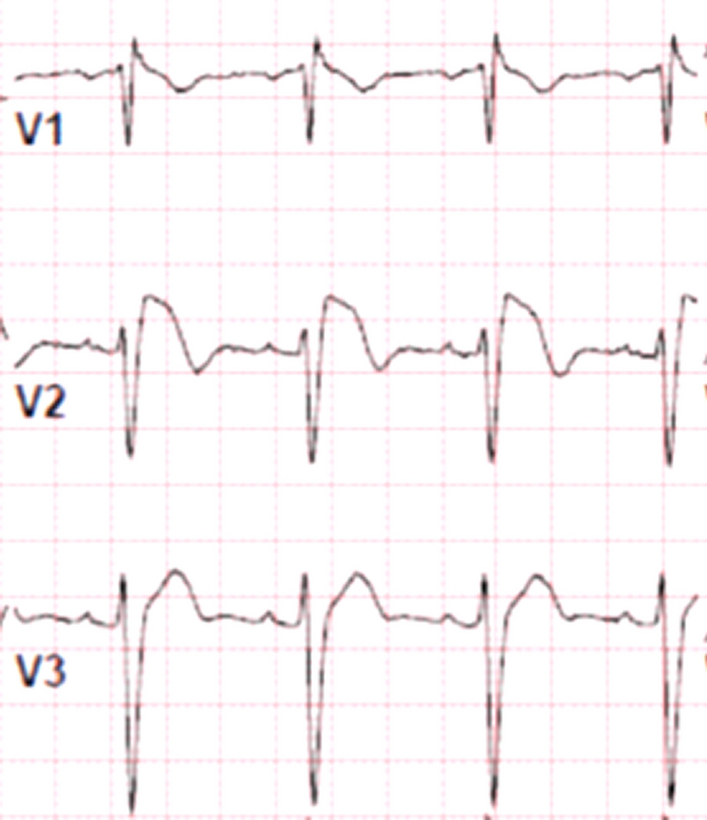
Rare RHD symptoms such as isolated severe TR are little documented in the literature. The current guidelines regarding echocardiographic characteristics of rheumatic carditis exclusively emphasize aortic and mitral valve abnormalities, disregarding rheumatic TV conditions [6, 10]. We establish that the echocardiographic observations of IRTR exhibit similarities to those documented for rheumatic MR. Through the use of continuous wave Doppler, this case study illustrates how the echocardiographic findings of isolated rheumatic MR and rheumatic TR are similar in terms of leaflet thickening, presence in at least two views, and a pansystolic jet. The high-velocity jet is the outlier, most likely because of the right side of the heart’s low pressure [1].
The majority of individuals with symptomatic TR are treated with diuretics to reduce volume overload and medicines aimed at the underlying illness process. Diuretics can temporarily slow down symptoms, but it is not known if this will change how the disease progresses, especially in those with primary valve disease [2, 8]. TV surgery is therefore the only effective treatment for severe symptoms. European Society of Cardiology Recommendations 2012 Class I recommendation for tricuspid valve surgery for severe primary or secondary TR at the time of left-sided valve surgery (level of evidence C) and symptomatic isolated severe primary TR without evidence of right ventricular dysfunction (level of evidence C) [5]. AHA/ACC Recommendations 2014 Class I recommendation for severe primary or secondary TR at the time of left-sided valve surgery (level of evidence C) and Class II recommendation for severe primary TR in patients unresponsive to medical therapy surgery may be appropriate (level of evidence C) [14]. Whereas 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease give Class IIa recommendation for isolated tricuspid valve surgery that may be helpful to patients with severe primary TR (Stage D) and right-sided HF signs and symptoms to lessen symptoms and hospital readmissions [15].
The majority of recommendations are intended for patients having simultaneous mitral or aortic surgery. Based on the observation that the TV's size and design do not consistently revert to baseline following the reduction of RV overload, these recommendations have been made. Patients who have severe annular dilatation, a history of unsuccessful TV repair, or abnormalities in the leaflets may need to have their TVR [8]. In this instance, surgical intervention should be taken into consideration as our patient exhibits severe isolated TR along with indications of right heart failure. Transcatheter treatments may manage functional TR but not organic TR like leaflet flail, prolapse, rheumatic disease, carcinoid disease, or endocarditis. Surgical replacement may be preferable due to suspected partial prolapse in the posterior leaflet [8, 16].
Isolated tricuspid valve replacement is a rare procedure with poor outcomes in patients with RHD and previous mitral valve replacements. It is associated with high post-operation problems and poor short and long-term prognosis. Only in specific circumstances after a thorough clinical and hemodynamic examination should it be performed. The scarcity of cases has limited data on its results [17]. Secondary antibiotic prophylaxis has been demonstrated effective in slowing the development of latent rheumatic heart disease [3].



Comments (0)