
Remember me




There were no notable differences in most aspects between all NHANES stroke survivors and those with complete information needed to be included in this analysis; the exceptions were that those included in the analysis were younger and had longer follow-up time and lower proportion of death (Supplementary Table 1).
Patient characteristicsThe average age of the stroke patients was 67.0 years, and 50.2% were women, of whom 8.1% were Mexican American, 6.1% other Hispanic, 51.7% White, 27.3% Black, and 6.9% other races and ethnicities. There were 277 deaths (30.2%) in this stroke survivor cohort over a median follow-up time of 5.3 (2.8–8.6) years. The average total magnesium intake across all patients was 251.0 (184.5–336.5) mg/d. According to EFSA recommended standard, 321 (70.2%) males and 339 (73.7%) females had insufficient magnesium intake. After considering energy intake, the average total magnesium intake was 14.5 (12.0–18.4) mg/(100 kcal*d). The quartiles of total magnesium intake levels were Q1 (≤ 12.0 mg/(100 kcal*d)), Q2 (12.1–14.5 mg/(100 kcal*d)), Q3 (14.6–18.4 mg/(100 kcal*d)), and Q4 (≥ 18.5 mg/(100 kcal*d)). Compared with survivors, those who died during follow-up were older, had higher PIR, serum creatinine, and total potassium and calcium intakes levels, had a higher proportion of hypertension, congestive heart failure, and coronary heart disease, and had lower BMI and total energy intake levels (all p < 0.05, Table 1).
Table 1 Clinical characteristics of patientsTotal magnesium intake and all-cause mortalityIn the univariate analysis, there was no notable difference of total magnesium intake between patients who died and those who survived (15.2 vs. 14.3 mg/(100 kcal*d), p = 0.20, Table 1). However, in any multivariate model that adjusted for potential confounders, total magnesium intake levels had an independent inverse association with all-cause mortality risk. After fully adjusting for potential confounding factors, each 1-mg/(100 kcal*d) increase in total magnesium intake was associated with a 3% reduced risk of all-cause mortality (HR, 0.97; 95% CI, 0.94–1.00; p = 0.017; Table 2). Patients in the fourth quartile of total magnesium intake showed a statistically significant decline in all-cause mortality risk compared to those in the first quartile (HR, 0.60; 95% CI, 0.38–0.94; p = 0.024). In the multivariable-adjusted Kaplan–Meier curves, a substantially lower risk of death was observed among patients with the highest quartile of total magnesium intake (Fig. 2). The multivariable-adjusted spline regression model further confirmed that the inverse association between total magnesium intake and all-cause mortality risk was linear (p-nonlinear = 0.69, Fig. 3). Stratified analyses showed that the statistically significant association between total magnesium intake and all-cause mortality was observed in patients who were older, female, without hypertension, and had smoking, normal renal function, and adequate energy intake (Table 3). The multivariable Cox regression model showed that total sodium, potassium, and calcium intakes were not related to all-cause mortality risk (Supplementary Table 2).
Table 2 Cox regression analysis to identify the association between total magnesium intake and all-cause mortalityFig. 2
The Kaplan–Meier curve for the study participants with different total magnesium intake. The curve was adjusted for the same confounding variables as in Model 4
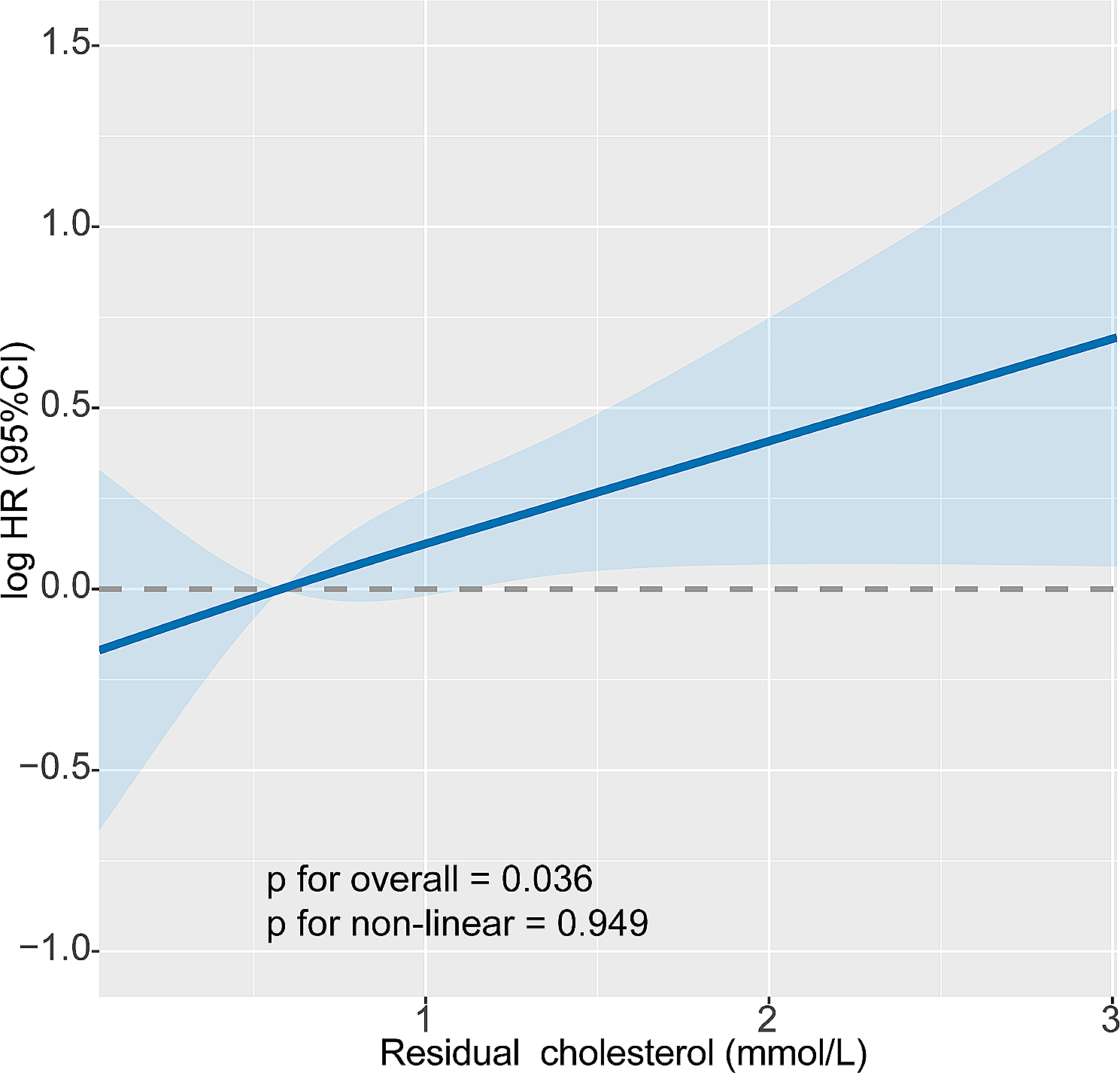
Fig. 3
Restricted cubic spline regression model of the relationship between total magnesium intake and risk of all-cause mortality after stroke. The model was adjusted for the same confounding variables as in Model 4. CI, confidence interval; HR, hazard ratio
Table 3 Stratified analyses to identify variables that may modify the association between total magnesium intake (per 1-mg/(100 kcal*d) increase) and all-cause mortalityDietary magnesium intake and all-cause mortalityAmong the included stroke patients, only approximately one-third of participants (276/917) had magnesium intake from dietary supplements. Thus, we additionally analyzed the relationship between dietary magnesium intake and all-cause mortality. The average dietary magnesium intake across all patients was 13.7 (11.5–16.8) mg/(100 kcal*d). Dietary magnesium intake was inversely associated with all-cause mortality risk in Models 1 and 2 (HR per 1-mg/(100 kcal*d) increase, 0.95; 95% CI, 0.91–0.99; p = 0.012; Supplementary Table 3). However, when dietary factors or past medical history was considered, the above association became insignificant (HR per 1-mg/(100 kcal*d) increase, 0.96; 95% CI, 0.91–1.01; p = 0.13).
DiscussionIn this cohort study of nationally representative sample of stroke survivors, a linear inverse association was found between total magnesium intake and risk of all-cause mortality. All-cause mortality decreased by 40% during follow-ups after a median of 5.3 years in the participants with the highest quartiles of total magnesium intake (≥ 18.5 mg/(100 kcal*d)). Dietary magnesium intake alone was not related to all-cause mortality. No statistically significant associations were observed between dietary sodium, potassium, or calcium intake and all-cause mortality.
Insufficient magnesium intake was found in approximately three quarters of stroke survivors, indicating that magnesium deficiency is quite common. Almost 64–67% of the US adults consumed less than the recommended standard of magnesium from food in 2001–2002, and the estimate decreased to 53–56% in 2005–2006 [11]. Magnesium intake level was 31% below the dietary reference intakes in the French adult in 2006–2007, and the figure reduced to 19% in 2014–2015 [12]. Although magnesium consumption in the population is gradually increasing, it is still far below the reference level, particularly in patients with stroke.
The results on the association between magnesium intake and all-cause mortality are in line with previous findings that focused on community populations or cancer patients. In a nationally representative sample of US adults, adequate intake of magnesium was associated with reduced all-cause mortality during a median follow-up of 6.1 years [13]. Another study conducted in the Mediterranean adults with high cardiovascular risk in Spain reported that participants in the highest tertile of dietary magnesium intake had a 37% reduction in all-cause mortality risk compared to those in the lowest tertile [14]. Two studies conducted in Chinese community populations showed decreased all-cause mortality in the individuals with a higher dietary magnesium intake; however, this association depended on dietary quality and the ratio of calcium to magnesium intake [15, 16]. An inverse association between total magnesium intake and all-cause mortality has also been observed in patients with breast and colorectal cancers [17, 18]. Our study provides new evidence for this inverse association in the stroke population and confirms that this association is linear.
It is plausible that the beneficial effect of high magnesium intake on all-cause mortality in stroke survivors could be due to neuroprotective role of magnesium. A drawback of our study was that the serum magnesium concentration was not measured. A multicenter study revealed that acute ischemic stroke patients with the lowest serum magnesium levels (< 0.82mmol/L) had two-fold increase in the risk of in-hospital mortality [19]. Magnesium levels in cerebrospinal fluid were also lower in patients with acute ischemic stroke who died within seven days than in those who survived [20]. Magnesium has several crucial roles in neuroprotection, including blockade of N-methyl D-aspartate (NMDA) receptor–mediated excitotoxic injury, calcium antagonism, vasodilatation, and antiplatelet effect [21]. The protective effect of magnesium was particularly evident in some subgroups of stroke patients, such as the elderly and those who smoked. Aging [22] and smoking [23] are associated with elevated levels of inflammation in the human body. Magnesium has anti-inflammatory effects and magnesium intake is inversely associated with serum C-reactive protein and interleukin-6 levels [24, 25]. Thus, ensuring sufficient magnesium intake is important for these subgroups. Total energy intake exceeding 2000 kcal per day ensures sufficient daily magnesium intake.
Total calcium intake independent of magnesium intake was not associated with all-cause mortality. Some studies have reported an association between calcium intake and all-cause mortality; however, most have not considered magnesium intake [26]. Calcium is essential for intracellular signalling, cardiac and vascular smooth muscle contraction, and coagulation pathway, but high levels may also contribute to atheromatous plaques [27].
Some limitations should be acknowledged in our study. First, the participants of this study were stroke survivors rather than acute stroke patients. The length of time from stroke onset to the first dietary recall interviews was unclear. Second, the diagnosis of stroke was determined by participants’ self-reports, which might introduce a false reporting. The survey questionnaire also did not distinguish between ischemic and hemorrhagic stroke. Third, serum magnesium concentration was not measured in this study. It is unclear whether the impact of total magnesium intake on all-cause mortality is mediated by serum magnesium levels. Fourth, some important confounding variables (e.g., stroke severity and adherence to secondary prevention of stroke) that might influence mortality were not available. Fifth, subgroup analysis was exploratory and the results need to be validated in an independent cohort.
Comments (0)