
記住我


A 63-year-old man presented to the emergency department by ambulance with sudden right chest pain and dyspnea. In the emergency department, he had 60% O2 pulse oximetry on room air and started using 10 L of reservoir mask oxygen. A chest X-ray (Fig. 1a) showed obstruction of the right bronchus and extensive atelectasis in the right lung, and chest CT (Fig. 1b, c) showed that there was infiltration into the right main bronchi and the right pulmonary artery. On the day of admission, ampicillin/sulbactam were started for obstructive pneumonia, and he was put on NPPV. At night, AF tachycardia and hypotension thought to be derived from sepsis were observed, and since the systolic blood pressure had fallen to the 70s, continuous administration of landiolol 15 mg/h and norepinephrine 0.3γ was started. Tracheal intubation was performed the next day.
Fig. 1
a–c Chest X-ray and CT at the first admission. a Atelectasis of the right lung. b Right main bronchus invasion (red arrows). c Right pulmonary artery invasion (red arrows)
On the third day of hospitalization, massive hemoptysis was observed, and blood flowed into the unaffected lung, leading to severe respiratory failure. Bronchoscopy revealed hemorrhage and a protruding mass from the right upper lobe to the right main bronchus (Fig. 2). A biopsy was impossible due to bleeding, but tissue adhered when the intubation tube was replaced, and the patient was diagnosed with primary lung adenocarcinoma of clinical stage T2bN3M0 (Stage IIIB, UICC 8th) after the examinations of whole-body and head contrast-enhanced CT. And as a result of pathological diagnosis, programmed death ligand 1 expression was high (Tumor Proportion Score > 95%). Since it was difficult to maintain oxygenation and cardiac arrest was imminent, V-V ECMO was first urgently introduced, and separated lung ventilation was performed to protect the unaffected lung, and deep sedation was also started. V-V ECMO was initiated with femoral extraction and jugular return. As a result of the multidisciplinary joint conference, due to low lung function and malnutrition, surgery was not indicated. And, IVR was not indicated due to bleeding from the tumor invading the pulmonary artery. Radiation therapy aimed at hemostasis and improvement of right atelectasis takes long time, but it was judged possible even under ventilator control. Fortunately, after the introduction of V-V ECMO, partial improvement in respiratory condition was obtained. After switching the intubation method to tracheostomy, it was decided to start radiotherapy. A tracheostomy was performed while V-V ECMO was in use, and a 7.5 mm endotracheal intubation tube was inserted into the left bronchus to continue isolated lung ventilation for the purpose of protecting the unaffected lung, and V-V ECMO was withdrawn. The total amount of transfusion used from the first day to the ninth day of hospitalization was 16 units of RBC, 24 units of FFP, and 50 units of PC.
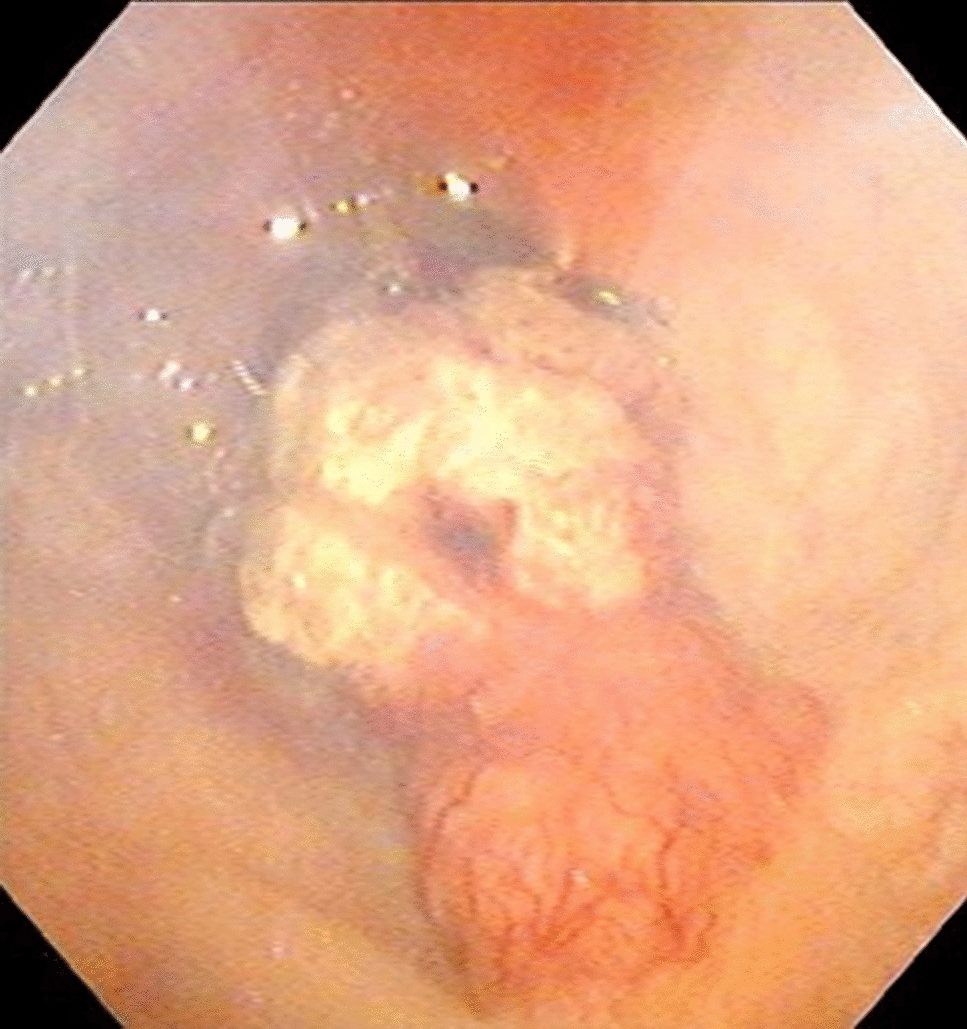
Fig. 2
Bronchoscopy showed bleeding from a tumor in the right main bronchus
Radiotherapy was then started at 30 Gy/10 fr. Three-dimensional conformal radiation therapy (3D-CRT) was used as the irradiation method. The purpose of irradiation was to stop bleeding and improve atelectasis in the right lung, and Clinical Target Volume (CTV) was focused only on the primary tumor (Fig. 3a, b). Because the position of the tumor shifted due to increased pleural effusion and atelectasis, Image-Guided Radiotherapy (IGRT) was used for each treatment, and position correction was performed using cone beam CT (Fig. 3c). Each irradiation was carried out under strong sedation as a countermeasure against body movement, and emergency department staff and a clinical engineer were present. From the start until about the third day after the start of irradiation, the patient continued to produce approximately 5 ml of bloody sputum per hour. Thereafter, the amount of bloody sputum gradually decreased, and by about the fifth day after the start of irradiation, it had changed to a normal yellow sputum. At the end of radiotherapy, almost no bloody sputum was drawn even with aspiration.
Fig. 3
a–c Radiotherapy. a Planning target volume is red contouring area. b 3D-CRT planning. c Cone beam CT
One week after the end of radiotherapy, the atelectasis in the right lung improved to some extent. In addition, thromboembolism of both pulmonary arteries was observed, and heparin was started, but recurrence of airway bleeding was not observed. About 1 month after the end of radiotherapy, the patient was completely weaned from the ventilator, and CT showed a reduction in the primary tumor of lung cancer and an improvement in air content in both lungs (Fig. 4). The speech cannula was removed about 2 months after the end of radiotherapy, and he was discharged ambulatory. The lung cancer treatment was continued on an outpatient basis, and additional irradiation of 30 Gy/10 fr to the shrinked primary tumor followed by treatment with pembrolizumab. The patient died of cancer 1 year and 1 month after the initial hospitalization due to an increase in peritoneal dissemination and associated complications of ileus. During the follow-up, recurrence of hemoptysis was not observed until death.
Fig. 4
Chest CT 1 month after radiotherapy showed that atelectasis in right lung improved and the primary lung cancer shrank
留言 (0)