Primary bladder adenocarcinomas comprise 0.5–2% of all bladder neoplasms. Primary signet-ring cell carcinoma of the bladder is particularly rare, accounting for only 0.24% of all bladder malignancies [2, 3]. In many cases, the tumor has already progressed by the time of diagnosis and the prognosis is poor. In a series of 54 cases in Japan, the median age of diagnosis was 61.2 years, with a male dominance of 3:1; additionally, 46% had stage IV disease. The overall survival rate at 2 years was 43%; further, no patients with stage IV disease at diagnosis were alive at 2 years [4].
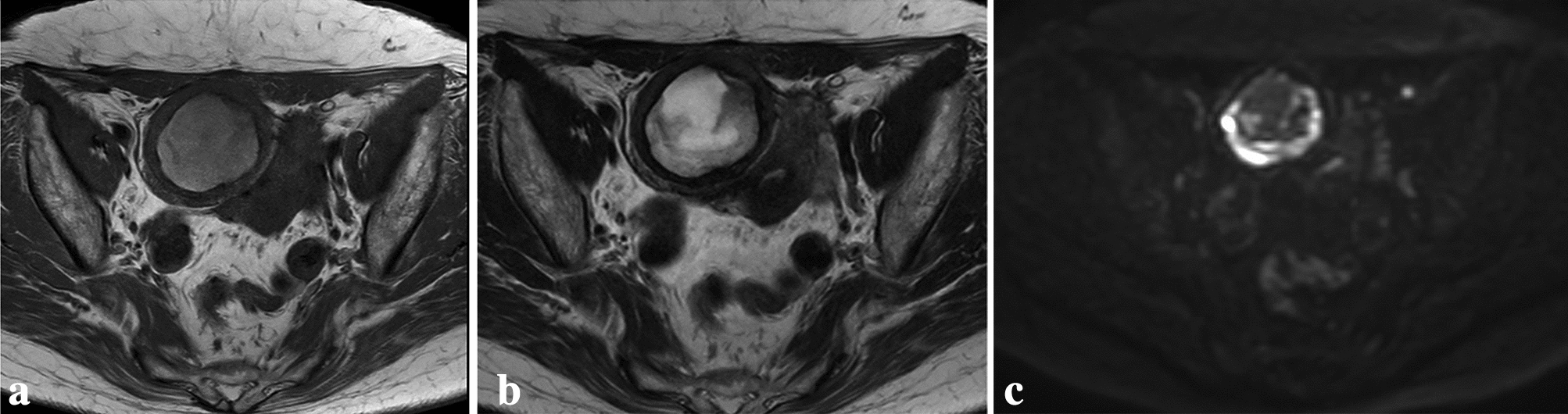
When diagnosing primary adenocarcinoma of the bladder, including signet-ring cell carcinoma, it is necessary to exclude metastatic tumors, urachal carcinoma, and prostate cancer. In the present case, the tumor was located in the dome of the bladder and urachal carcinoma was initially suspected. However, the tumor was growing into the lumen rather than outside the bladder and there were no urachal remnants or a suprapubic mass. Thus, it did not meet Wheeler and Hill’s criteria for urachal carcinoma [5]. Immunohistochemically, the tumor was positive for AE1/AE3, cytokeratin 7, and cytokeratin 20, indicating that it had originated from the urothelium. Investigations for a primary tumor elsewhere were negative. Therefore, the patient was diagnosed with primary signet-ring cell carcinoma of the bladder.
Some primary signet-ring cell carcinomas of the bladder are associated with high serum carcinoembryonic antigen and carbohydrate antigen 19–9 concentrations. These are reportedly useful biomarkers for assessing prognosis or treatment efficacy [4, 6]. However, in our case, both were within the reference range.
There is no established treatment; however, radical cystectomy is recommended when the tumor is localized [4]. In a report comparing open and laparoscopic radical cystectomy (LRC), although LRC was associated with longer operative time, amount of blood loss, length of hospital stay, need for blood transfusion, amount of narcotic analgesia required, and time to ambulation and regular diet for LRC were superior to open radical cystectomy. There was no significant difference in local recurrence rate or disease-free survival [7]. The range and accuracy of lymphadenectomy associated with radical cystectomy are controversial; however, there is agreement that the number of dissected lymph nodes is an important indicator. It is recommended that 20 or more lymph nodes be dissected [8]. In the present case, 25 lymph nodes were removed, suggesting that the surgical procedure was adequate. Because LRC has few complications, an additional advantage is that chemotherapy can be commenced immediately after surgery if considered necessary. To the best of our knowledge, there are no published reports on the patient performed with LRC for bladder signet-ring cell carcinoma. Our patient was discharged 23 days postoperatively without major complications and has been free from recurrence ever since. Robot-assisted surgery is now available and there is a shift toward minimally invasive surgery. We believe that reporting this case of complete cure after minimally invasive surgery will be helpful.
Various chemotherapy regimens have been reported, including gemcitabine with cisplatin and the combination of methotrexate, vinblastine, doxorubicin, and cisplatin, both of which are prescribed for standard urothelial carcinoma. Use of drugs used for advanced gastric cancer, such as S-1 (tegafur/gimeracil/oteracil) has also been reported. However, there is currently no standard chemotherapy regimen. Furthermore, the usefulness of NAC for UC with variant histology is not clear. In regards of neoadjuvant therapy, its usefulness for UC with variant histology as well as pure UC has been reported [9]. We considered that NAC is also effective for this case with signet ring cell carcinoma, which is one of variant of UC. Table 1 shows the regimens used in 12 cases of bladder signet-ring cell carcinoma treated with chemotherapy [4, 6, 10,11,12,13,14,15,16,17,18]. However, these reports were not about neoadjuvant therapy, but about adjuvant therapy or systemic therapy for metastatic disease. In addition, these reports were all about regimens that urologists do not normally use or associated with severe adverse events. We selected PCG therapy as neoadjuvant chemotherapy for our patient because of its high grade compared with the usual urothelial carcinoma and a report that PCG therapy prolonged overall survival compared with gemcitabine with cisplatin in patients with advanced urothelial carcinoma [19]. Furthermore, since we are accustomed to usage paclitaxel, we thought that it would be possible to deal with adverse events if paclitaxel was added to gemcitabine and cisplatin. The reported regimen consisted of paclitaxel 80 mg/m2 (days 1 and 8), cisplatin 70 mg/m2 (day 2), and gemcitabine 1000 mg/m2 (days 1 and 8) in 3-week cycles. However, in this case we adopted a 4-week cycle because of adverse events. Although the patient required granulocyte colony stimulating factor for management of neutropenia, two courses were administered. Histopathological examination of the operative specimen confirmed the efficacy of the treatment. The optimal number of courses of preoperative chemotherapy remains controversial. However, we have identified no postoperative recurrences in our patient, suggesting that PCG therapy is an effective treatment for primary signet-ring cell carcinoma of the bladder.
Table 1 Characteristics of 12 cases of bladder signet-ring cell carcinoma treated with chemotherapyIn conclusion, this patient with primary signet-ring cell carcinoma of the urinary bladder, which generally has a poor prognosis, was administered PCG as neoadjuvant therapy, then underwent LRC and achieved a prolonged complete response.


Comments (0)