We report a rare case of metastatic esophageal cancer originating from signet-ring cell carcinoma of the cecum. We discuss characteristics of esophageal metastasis from colorectal cancer by comparing our case with previously published cases.
Metastatic esophageal cancer was first reported in 1942 by Gross and Freedman [2]. Subsequently, many cases of the cancer have been reported. A common first symptom of esophageal metastasis is dysphagia. Mizobuchi et al. reported that esophageal stenosis covered with intact mucosa was endoscopically characteristic of metastatic esophageal cancer [1]. Mechanisms of esophageal metastasis include lymphatic or hematogenous spread of the primary cancer in a distant organ. Metastatic esophageal cancer is often located in the submucosal layer covered with intact mucosa, which makes the diagnosis of the cancer difficult [3]. Differential diagnoses of metastatic esophageal cancer include esophageal submucosal tumors and rare types of primary esophageal cancer (e.g., basaloid squamous cell carcinoma, sarcoma, lymphoma). Ultrasonography has been reported to be useful for making a diagnosis of metastatic esophageal cancer [4]. The cancer is commonly treated with standard chemotherapy for the primary site. Esophageal stent placement is a treatment option for patients with malignant esophageal stenosis. However, the outcome of treatment is poor in most cases of esophageal metastasis.
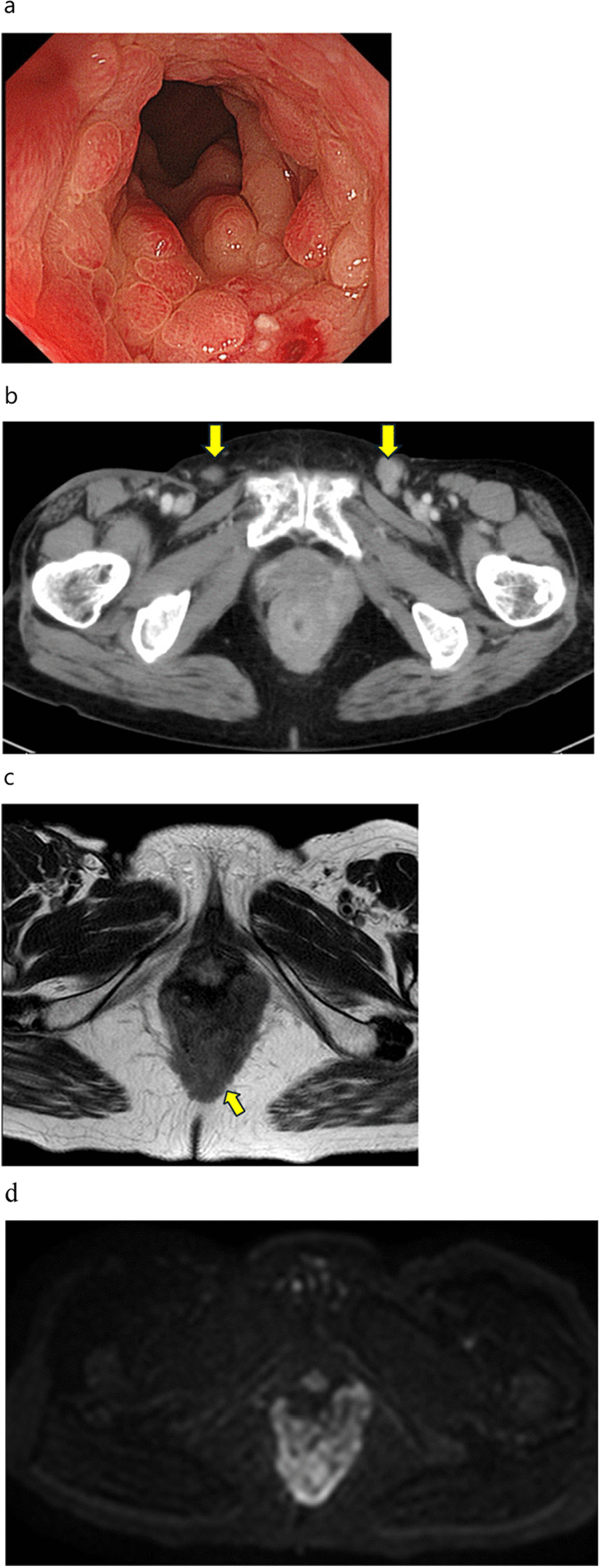
In our case, the patient experienced no symptoms of esophageal stenosis, such as vomiting, dysphagia, and difficulties in eating. Although esophageal stenosis covered with intact mucosa has been known as a characteristic endoscopic finding of metastatic esophageal cancer, no such stenosis was found in our patient. She had multiple longitudinal submucosal tumors with erosions on their surfaces and with non-neoplastic epithelia on their edges. This finding is different from typical endoscopic findings of primary esophageal cancer or esophageal submucosal tumors, which usually occur as a single tumor.
Multiple longitudinal tumors of the esophagus have been found in patients with intramural metastasis from primary esophageal cancer. Watson et al. referred to longitudinal intramural metastasis from primary esophageal cancer [5]. Intramural metastasis of the esophagus is defined as “metastatic lesions in the esophageal, pharyngeal, or gastric wall macroscopically (clearly) separate from the primary tumor” in the Japanese Classification of Esophageal Cancer 11th Edition proposed by the Japanese Esophageal Society [6]. In our case, esophagoscopy showed that multiple submucosal tumors with mucosal changes extended longitudinally and discontinuously. This finding is similar to a common endoscopic finding of intramural metastasis from primary esophageal cancer. We consider that the multiple longitudinal submucosal tumors with mucosal changes are a notable feature of our case.
According to Takubo et al. [7], frequent lymph node metastasis in patients with intramural metastasis from primary esophageal cancer suggests that intramural metastasis is a secondary lesion of the affected lymph nodes as well as the primary cancer. In our case, many regional lymph node metastases and severe lymphatic invasion were found in the resected colon specimens. Signet-ring cell carcinoma of the colon has been reported to tend to severely invade lymphatic vessels in the abdomen [8]. We thus consider that our patient’s colon signet-ring cell carcinoma metastasized into the esophageal wall via the abdominal lymph flow from lymphatic vessels invaded severely by the colon cancer. The intramural metastasis could have appeared as multiple longitudinal submucosal tumors of the esophagus.
Metastatic esophageal cancer is typically covered with intact mucosa, which often makes differential diagnosis difficult. In our case, however, no magnifying endoscopy or ultrasonography was performed on the esophagus. Tumor biopsy enabled us to diagnose the esophageal condition.
In patients with esophageal metastasis from the gastrointestinal tract, the most common primary lesion is the stomach [1]. Esophageal metastasis from colorectal cancer is rare. A PubMed search of case reports found only 6 patients with such metastasis between 1976 and 2021 [9,10,11,12,13,14] (Table 1). The pathological diagnosis of primary colorectal cancer was compared in the 6 patients; 4 had moderately or poorly differentiated adenocarcinoma, 1 had mucinous adenocarcinoma, and 1 had no available data. None of the 5 patients with pathological data had primary signet-ring cell carcinoma of the colon. To the best of our knowledge, the present report documents the first case of metastatic esophageal cancer originating from signet-ring cell carcinoma of the colon in the English language.
Table 1 Cases of esophageal metastasis from colorectal cancer identified on literature reviewOf the 6 patients, 4 had mucosal changes of the esophagus found by endoscopy. Two patients had esophageal stenosis. These results suggest that esophageal metastasis from colorectal cancer is likely to cause mucosal changes rather than stenosis of the esophagus. None of the 6 patients had multiple longitudinal tumors of the esophagus, which differs from our case. Five patients had lymph node metastasis in the abdomen. This finding confirms that the lymphatic spread is a common route for esophageal metastasis from colorectal cancer.
Primary signet-ring cell carcinoma of the colon is as rare as 0.1–2.4% of all colorectal cancers and has a poor prognosis [15]. In contrast, primary signet-ring cell carcinoma of the stomach is common, including minute signet-ring cell carcinoma [16]. For the identification of the primary site of metastatic cancer, immunohistochemistry using CD7, CD20, and CDX2 has become a useful examination [17, 18]. In our case, immunohistochemical examination was performed to differentiate colorectal signet-ring cell carcinoma from gastric signet-ring cell carcinoma as the primary site, although upper gastrointestinal endoscopy showed no notable abnormality in the stomach. Both the colorectal lesion and the esophageal tumors showed the CK7−/CK20 + /CDX2 + staining pattern, which suggests that the esophageal tumors originated from colorectal cancer [17, 18]. We found that immunohistochemistry using CD7, CD20, and CDX2 helpful for differentiating colon signet-ring cell carcinoma from gastric signet-ring cell carcinoma to identify the primary site of metastatic esophageal cancer.
Since the absence of esophageal stenosis and the results of immunohistochemical examination suggested that our patient’s metastatic esophageal cancer originated from signet-ring cell carcinoma of the colon, the esophageal lesion was treated with systemic chemotherapy and molecular targeted chemotherapy for the treatment of unresectable advanced or recurrent colorectal cancer in compliance with the Japanese treatment guidelines for colorectal cancer [19].
However, there were 2 major limitations of her treatment. First, anti-EGFR therapy could not be administered. The resected specimen of the colon cancer had wild-type KRAS mutation, indicating that the patient was a candidate for anti-EGFR therapy. However, she refused the therapy because of its potential adverse effects, such as acne-like rash. In addition, her primary tumor was right-sided colon cancer. Anti-EGFR therapy has been known to be less effective for right-sided colon cancer than for left-sided colon cancer [20]. Therefore, she was treated with FOLFOX/BV therapy. Second, neither BRAF mutation test nor MSI mutation test could be performed to identify effective treatment regimens for colon cancer. Both gene panel tests were not yet covered by the national health insurance and thus were not clinically available when we treated the patient.



留言 (0)