Despite of fair discrimination power, current study suggests that EuroSCORE II underestimate mortality risk in all scoring category in this population. This result is supported by a multi-center study done by Kurniawaty, et.al conducted at Dr. Sardjito Hospital, Kariadi Hospital, and Abdul Wahab Sjahranie Hospital, which stated that EuroSCORE II had a poor predictive value and led to an underestimation of mortality risk in patients undergoing major cardiac surgery, though some parameters included in the scoring system did have significant association with patient outcomes. Diabetes, history of previous cardiac surgery, left ventricular dysfunction, history of myocardial infarction, and procedure status which each had a significant OR in this study were found to have no significant association in this multi-center study. It should be emphasized that these studies involved several types of cardiac surgical procedures, and the majority were non-coronary procedures [10].
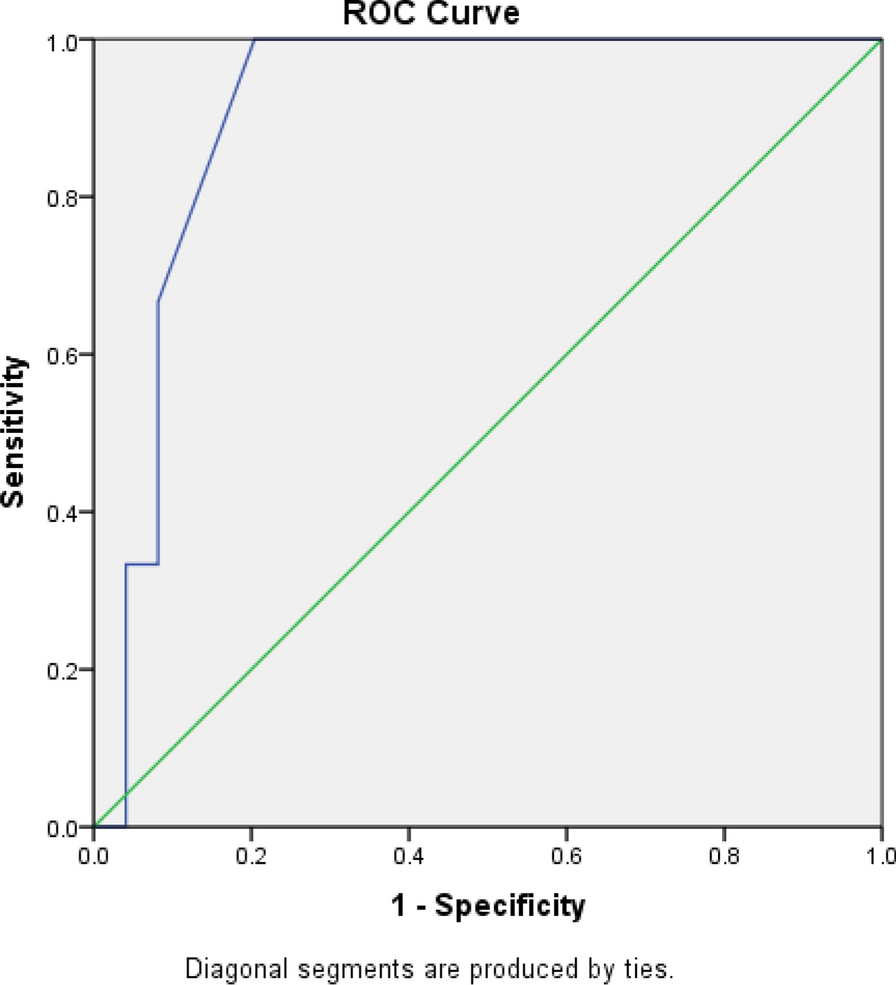
In contrast, Sembiring, et.al found a slightly different results where EuroSCORE II had good calibration as a predictor for mortality in patients undergoing major cardiac surgery (including surgery, heart tumor surgery, aorta surgery, or a combination of these surgeries) based on the Hosmer–Lemeshow analysis (p = 0.55), and the area under the ROC curve is 0.85 which indicates a good discriminant value. However, this study actually overestimated mortality in EuroSCORE II. An additional finding obtained from that study was that this scoring system tends to overestimate the risk of death for the group of patients with EuroSCORE II < 1.3% and underestimate the risk of death for the group of patients with EuroSCORE II > 2.3% [8]. Another study that also used samples undergoing isolated CABG in Medan also found a statistically significant association with EuroSCORE II stratification on mortality. Moreover, EuroSCORE with a value of > 3.31 could be used to predict major cardiovascular events after CABG with a sensitivity of 90% and a specificity of 90%. Unfortunately, the study did not validate the accuracy of the use of EuroSCORE II itself [11].
The patient’s overall characteristics in this research were not significantly different from those of the original EuroSCORE II study. The only significant difference between the two studies was that endocarditis was not found in any of the patients in this study [3]. Patients with endocarditis are more likely to undergo concurrent valve surgery procedures; whereas, this study focused on patients undergoing CABG alone. Stroke (OR 2.28; 95% CI 1.331–3.903) and hypertension (OR 1.62; 95% CI 1.039–2.511) were found to significantly increase the risk of mortality in this study. These two comorbidities had not been considered in the original EuroSCORE II study, although Herlitz, et.al already suggested in their study that hypertension increases the risk for direct post-procedural complications and two year mortality rate [3, 12]. The effect of stroke on the increased risk of death in this study may because patients with a history of stroke also have poor mobility. Bottle, et.al found that history of stroke before CABG did not affect the outcomes of the procedure unless accompanied by other morbidities [13]. In this study, the onset of myocardial infarction was also found to influence the mortality risk in patients. In the original EuroSCORE II study, similar results were found with onset category of < 72 h, 72 h—three months, and more than three months. This parameter was not included in the final scoring system because it was considered to have the same value as the patient's procedure status, and when reanalyzed by the regression method, the association of onset with mortality risk was significantly reduced [3].
In Asia, the use of EuroSCORE II as a mortality predictor in post-cardiac surgery patients is still being debated. Studies in Malaysia and Bangladesh that were also conducted in isolated CABG populations found that EuroSCORE II was good enough to predict mortality in their research population. Musa, et.al found no significant difference between predicted mortality based on EuroSCORE II and observed mortality, which indicates a good model calibration [6]. Ranjan et.al who found that EuroSCORE have an important role in predicting early prognosis and end outcome also support the previous study, even though there’s a little discrepancy between the expected mortality and the observed mortality in their result [14]. In India, EuroSCORE II is considered not ideal for predicting mortality in post-major cardiac surgery patients according to a cohort study which found that the scoring system only correctly predicted the low and moderate risk patients, but overestimated the high risk group [7].
Research conducted in Greece, Serbia, the Netherlands, Argentina, as well as meta-analysis studies in America and the UK suggest that EuroSCORE II has improved the previous scoring system and is quite valid to predict mortality in post-heart surgery patients, either isolated CABG, valve surgery, or combined surgery [5, 15,16,17,18]. An interesting finding from a multi-center study in Argentina stated that EuroSCORE II showed adequate performance in terms of discrimination and calibration for all types of surgery, although it was somewhat lower for coronary surgery [15]. According to H.L. Blum’s theory, the degree of a person's health can be determined by 40% of environmental factors, 30% of behavioral factors, 20% of health care factors, and 10% of genetic factors [19]. In addition, there are several factors other than health services that may be the reason for the differences in the validity of EuroSCORE II in Indonesia and abroad.
There may be some possible limitations in this study. This study was conducted at a national heart center where many patients were referred by the smaller hospital and tend to have other comorbidity that could worsen patient’s outcome. It should be noted that in this study several variables were not taken into account in EuroSCORE II, but had significant associations with mortality such as the onset of infarction and hypertension. Inaccurate patient comorbid history measured in EuroSCORE II due to patient misunderstandings during history taking can also contribute to this difference since our data based on patient anamnesis when they first brought to the ER. For example, in this study, 3.6% of patients who were not diagnosed with diabetes had HbA1C > 6.5% with 53.4% missing HbA1C data. Whereas according to research by Zheng, et.al, HbA1c levels were potentially associated with an increased risk of all-cause death, myocardial infarction, and stroke in diabetic subjects undergoing CABG surgery [20]. Research by Soewondo, et.al which examined several data sources available in Indonesia also stated that the prevalence of diabetes was 5.7%, with 70% of cases being undiagnosed [21]. Further research is needed to establish a more accurate scoring system for the Asian population, especially Indonesia, by taking into account these variables and possibly other variables that have not been taken into account in this study.



Comments (0)