
記住我
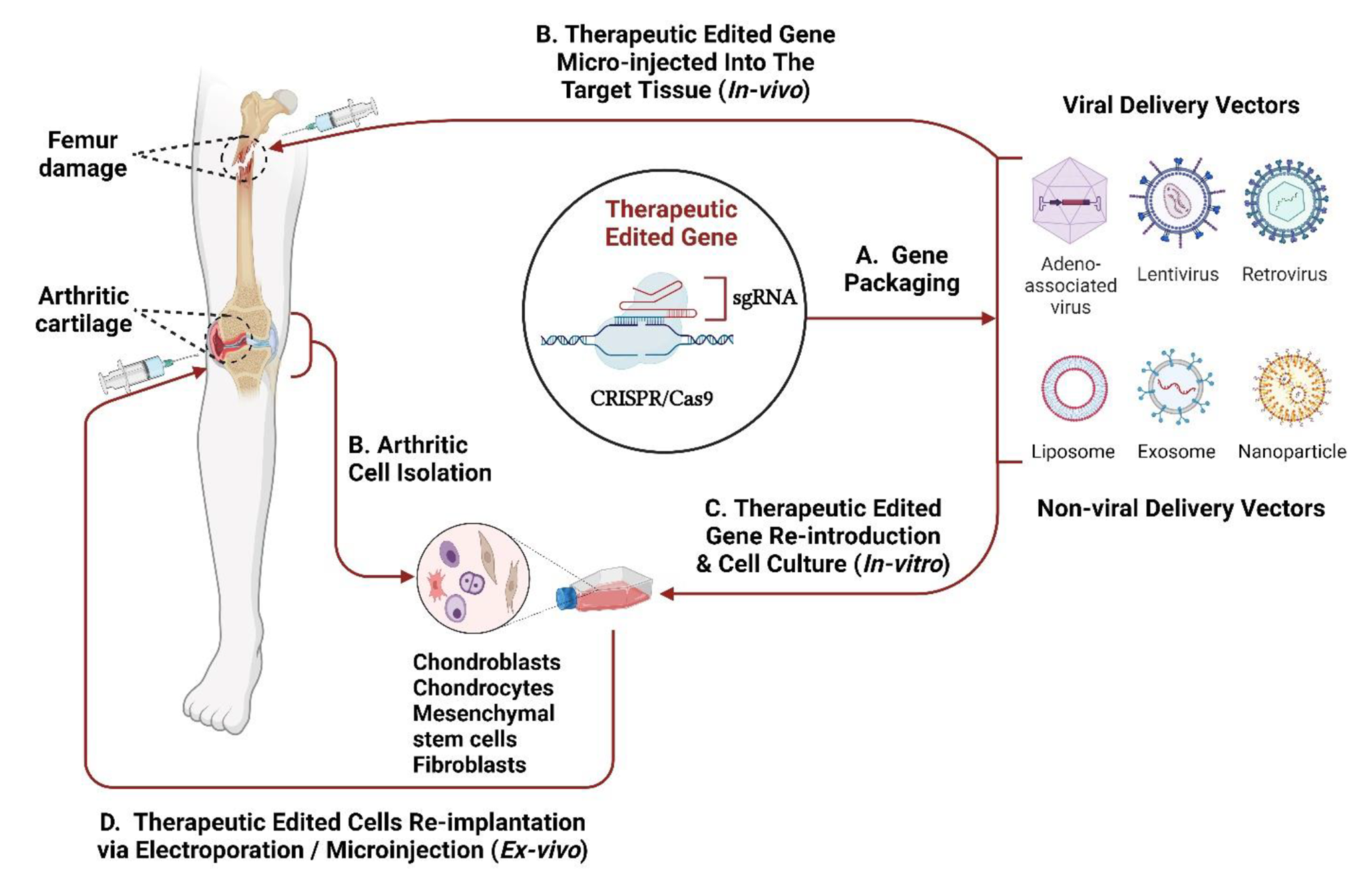

Owing to the several links between the gut, with microbial set its, and thyroid homeostasis, the term “gut-thyroid axis” has been recently proposed [50] and the principal elements involved are depicted in Fig. 2.
Fig. 2
Main elements involved in the “gut-thyroid axis”
Thyroid hormones exert a key role in the development and differentiation of intestinal epithelium, thus actively participating in the intestinal barrier integrity. Among the intestinal effects of thyroid hormones, the more relevant are the regulation of intestinal epithelium turnover [51] and the induction of intestinal alkaline phosphatase. This latter is a brush-border enzyme that dephosphorylates the proinflammatory bacterial endotoxin lipopolysaccharide (LPS), thereby preventing its translocation into the systemic circulation [52, 53]. This process has been correlated to the induction of autoimmunity in genetically- predisposed subjects, since the intestine hosts the 70% of the immune system (Gut Associated Lymphoid Tissue – GALT) [54]. Indeed, the entry into the systemic circulation of bacterial antigens and their epitopes, even through the molecular mimicry, may trigger auto-aggressive processes [55] by a local or by-stander activation. Furthermore, it represents a potential site for the activation of autoreactive cells and initiation/propagation of autoimmune diseases, also involving organs far from the intestine [56]. To note, a condition of gut leakiness has been also related to the growth and progression of cancers involving organs other than thyroid [54].
On the side of thyroid function variations, they have also been related to a different gut microbiota composition: in hypothyroid patients an increased prevalence of small intestine bacterial overgrowth has been described [57] as well as a dysbiotic state in patients with thyroid hyperfunction [58]. Conversely, it was demonstrated that germ free (GF) mice, devoid of microorganisms colonization, have lower radioactive iodine uptake and 25% higher values of TSH than conventionally reared ones [59]. To note, a direct binding of thyroid hormones to gut bacterial strains has been firstly demonstrated in the 60’s, suggesting the intestine to be a reservoir for thyroid hormones [60]. It has been also hypothesized a role for the intestine and the associated microbiota in thyroid hormones metabolism since:—some bacterial strains possess glucuronidase and sulfatase activities, enabling thyroid hormone enterohepatic recycling;—in mice, intestinal wall possesses deiodinases isoforms and ornithine decarboxylase allowing the synthesis of thyroid hormones’ derivatives;—deiodinases activities, that have been detected in the intestinal content of rats, are inhibited by resident microbiota [17];—in animal models, LPS injection is able to modulate hepatic and pituitary deiodinases activity [13]. Thyrocytes themselves are able to respond to circulating LPS because of their expression of functional Toll-like receptor 4 (TLR4), which is able to induce both Na+/I symporter (NIS) and thyroglobulin (Tg) gene expression [61]. LPS is also able to decrease thyroid hormone receptor expression in hepatic extracts [13]. Interestingly, SCFAs (Short Chain Fatty Acids) (butyrate, propionate and acetate) produced by resident microbiota are able to inhibit histone deacetylase and to activate Mitogen-activated protein kinase (MAPK) pathway that may induce hyperphosphorylation and thus increased transcription of thyroid hormone receptor [13]. Some papers reported a variation in SCFA concentration in patients with different thyroid disorders [31]. Another key element of the thyroid-gut axis is represented by bile acids homeostasis. Indeed, secondary biliary acids, formed in the colon through deconjugation and dehydroxylation by colic microbiota, are able to interact with Takeda G-protein coupled receptor 5 (TGR5), a receptor that stimulates type-2 deiodinases in brown adipose tissue, increasing local triiodothyronine (T3) production. On the other hand, thyroid hormones regulate biliary acids’ metabolism increasing the liver expression of cholesterol 7α-hydroxylase (CYP7A1). Interestingly, one of the secondary bile acids, deoxycholic acid, possesses a selective antimicrobial effect due to its ability to induce bacterial membrane damage. Noticeably, the composition of primary and secondary biliary acids is significantly different in patients with hyper- or hypothyroidism [21, 31].
In the next paragraphs, we will stress the relationship between the microbiota, its byproducts and the more common thyroid disorders.
4.1 Hashimoto’s thyroiditis and hypothyroidismAlready in the 80’s, it has been shown that GM conferred a greater susceptibility to the development of thyroiditis in rodents grown in conventional conditions compared to GF ones [62]. To note, sequences homologies have been found between thyroid-specific antigens [thyroid peroxidase (TPO) and Tg] and surface antigens of several bacteria, both pathogens or commensals, normally belonging to gut microbiota [63]. Later, it has been proven that TLR4 activation by LPS is able to trigger thyroiditis in NOD H2h4 mice [64]. Other clues of a role for GM in Hashimoto’s thyroiditis (HT) pathogenesis are related to the detection of the leakiness of the gut barrier detected in a morphologic and functional study in euthyroid patients with this disorder [65]. This evidence has been strengthened by the evidence that serum zonulin, an indirect index of increased gut permeability, is increased in HT patients [66].
Recently, a meta-analysis described the significant differences of GM composition in HT patients compared to healthy subjects. Sawicka-Gutaj et al. [44] reported that ACE and Chao1, indices describing microbial richness, and the Shannon index, reflecting the communities’ diversity, were increased in HT patients as compared to healthy controls. However, the Simpson index, which reflects the community diversity too, was lower in HT patients [44]. Overall, these results are in keeping with the longer gastrointestinal transit time that is a key sign in hypothyroid patients and that has been related to increased prevalence of small intestine bacterial overgrowth [57].
At phylum level, Bacteroidetes showed an increased relative abundance and Firmicutes a slightly reduced one compared to control subjects. To note, the Firmicutes/Bacteroidetes (F/B) ratio is known to be an indicator of normal intestinal homeostasis; this ratio’s increase or decrease has been suggested as flag of dysbiosis. [42]. A decrease in this ratio has been described in GD but in HT patients inconsistent results were reported [44].
At family level, some studies demonstrate that Lachnospiraceae, Bacteroidaceae, Enterobacteriaceae, Alcaligenaceae, Coriobacteriaceae, Erysipelotrichiaceae and Bacillobacteriaceae were increased in the gut microbiota of the HT patients; differently, Ruminococcaceae, Prevotellaceae, and Veillonellaceae were reduced [42]. Interestingly, these last two families are involved in the induction of regulatory T lymphocytes (Tregs) in the gut [42, 43].
At genus level, it was observed that Bacteroides, Faecalibacterium, Prevotella and Lachnoclostridium genera were lower, while Blautia, Ruminococcus, Roseburia, Fusicatenibacter, Romboutsia, Dorea and Eubacterium genera were higher in HT patient fecal samples than in healthy controls [44].
At species level, the most important result of the above meta-analysis was the increased relative abundance of Bacteroides fragilis, a bacterium able to activate the expression of NLR family pyrin domain containing 3 (NLRP3), an inflammasome component overexpressed in thyroid tissue of patients with HT [33]. When analyzed by Spearman’s correlation, some phylum, family and genus such as Bacteroides, Ruminococcaceae, Enterobacteriaceae, Veillonella, Streptococcus and Lactobacillus positively correlated with antithyroperoxidase antibodies (TPO) and negatively with TSH levels; moreover, the genus Streptococcus positively correlated with antithyroglobulin antibodies levels [42, 44, 47].
One study examined the gut microbiota composition in untreated patients with non-autoimmune hypothyroidism as compared to healthy subjects [67]. The authors described greater richness but lower diversity in the hypothyroid group, with increased F/B ratio and LPS serum concentration; also the SCFA producing ability was significantly reduced [67]. In the last years, it has been also evaluated the relationship between functional thyroid disorders and the composition of microbiota belonging to body niches different from the gut one [48]. A significant alpha and beta diversity on salivary samples has been described by Dong et al. [68] by comparing the microbiota of 20 healthy control (HC) and 20 subjects affected by subclinical hypothyroidism (SH). It was observed that salivary microbial composition of SH group was characterized by a major richness without the identification of a dominant species. At the phylum level, there was a similar composition between the two groups but a different distribution of 45 taxa [68].
4.1.1 Microbiota composition and levothyroxine treatmentIn patients with hypothyroidism, oral levothyroxine sodium is the treatment of choice. This treatment must be personalized based on the weight and age of patients, but its efficacy depends on the absorbed hormonal fraction [26]. It has been hypothesized that levothyroxine treatment efficacy might be influenced by the composition of the gut microbiota [69]. Indeed, once absorbed at the small intestine level, thyroxine is metabolized by deiodinases but a significant fraction may be glucurono-conjugated and sulfated at liver level, rendering it more soluble in water and allowing its elimination in the intestine along with the bile [70]. It has been demonstrated that bacterial glucuronidase and sulfatase activities are able to give back thyroxine the possibility to be reabsorbed through the enterohepatic recycling [71, 72]. A recent study compared gut microbiota composition in subclinical hypothyroid patients with stable or increasing levothyroxine requirement, describing a different relative abundance at genus level in Alistipes and Ruminococcus (some strains belonging to these genera possess beta-glucuronidase activity) and in Anaerotruncus genus (involved in intestinal barrier stability through butyrate production) [73].
4.2 Graves’ disease, with or without orbital involvement, and antithyroid treatmentUsing animal models established by immunization with human TSHR, Masetti et al. [74] and Moshkelgosha et al. [75] analyzed how differences in gut microbiota influence the clinical manifestation of GD and Graves’ ophthalmopathy (GO) with two experiments: the first one comparing the same mouse model (BALB/c mice) placed in two different locations (Germany, UK); the second one comparing two different mice strains (C57BL/6 and BALB/c mice). Gut microbiota compositions resulted significantly different in both the experiments and correlated with clinical manifestation of GD/GO. In another experiment, Moshkelgosha et al. [76], before the TSHR immunization, administrated antibiotic vancomycin that lowered the richness and diversity of gut microbiota, also reducing F/B ratio. A significant reduction of Tregs in orbital lymph nodes and GD/GO-like clinical features has been observed. These studies suggested a crucial role of gut microbiota in the clinical manifestation of GD and GO.
In the last years a growing number of papers has faced the study of gut microbiota in patients with GD and GO. A condition of increased intestinal permeability, proved by the increase of circulating markers of leaky gut (LPS, zonulin, and D-lactate) has been described in these patients by Zheng et al. [77]. Moreover, higher LPS levels were associated with more severe hyperthyroidism, higher TSH Receptor Antibodies (TRAb) concentrations, and a worse course of both hyperthyroidism and orbitopathy [78]. A recent meta-analysis [44] examined 12 papers, mostly from China, analyzing a total of 563 patients with GD/GO who underwent fecal microbial analysis. The meta-analysis showed a clear trend toward decreasing values of all indices of richness and diversity in GD patients as compared to healthy controls. In most of the studies, the F/B ratio was lower in GD patients than in healthy individuals, suggesting the presence of dysbiosis in GD patients. Similar modifications were observed in GO patients. However, quite opposite results have been reported by Masetti et al. [23] that anticipated the results of the INDIGO study, a large-scale analysis in GD and GO patients in four European countries. In this study, fecal samples were obtained from untreated patients or within 6 weeks from treatment initiation. No significant differences emerged in alpha and beta diversity indices. Bacteroidetes were significantly decreased, while the F/B ratio was significantly higher in GD/GO than in healthy controls. These conflicting results may be explained by the different geographical origin of the patients with different environmental exposures, namely dietary habit [78]. Back to the results in GD patients from Sawicka-Gutaj et al. [44], a trend toward an increased abundance of Bacteroidetes and Actinobacteria at the phylum level, reflected in a higher abundance of Prevotella and Bifidobacterium at the genus level, has been observed. Similarly, a higher abundance of Prevotella was reported in GO patients.
Among clinical parameters, TRAb levels positively correlated with Prevotella, Bifidobacterium and Lactobacillus, while CAS (clinical activity score) was associated with Bacteroides abundance [79]. Noticeably, some species belonging to Prevotella genus, through the activation of TLR 2, are able to induce the secretion of proinflammatory cytokines and to promote neutrophil recruitment. An increased concentration of Prevotella genus has been described in HIV infection, obesity, hypertension and Nonalcoholic Fatty Liver Disease (NAFLD), as well [80]. Similarly, some Bifidobacterium and Lactobacillus strains could exert a pathogenic activity in autoimmune thyroid disorders (ATD) through molecular mimicry, due to their structural homology with the amino acid sequences of human TPO and Tg [81]. This evidence could explain the findings of Jiang et al. [82] and Chen et al. [83], which, analyzing the fecal microbiota in GD patients, revealed that the abundance of Lactobacillus was significantly higher in TPO autoantibodies (TPOAb) positive GD patients than that in TPOAb negative ones. Moreover, it could potentially justify the conflicting findings of Ishaq et al. [84] who, antithetically, described a reduction in Bifidobacterium and Lactobacillus in GD patients.
Fewer evidence is available about the effect of GD/GO therapy on microbiota and vice versa. Maier et al. [85] assessed the effect of methimazole (MMI) and of propylthiouracil (PTU) on 40 selected bacterial strains in vitro, finding minimal influence. On the contrary, Chen et al. [83] analyzed GM in MMI treated GD patients reporting a significantly improved diversity after 3–5 months treatment and a significant reduction of Lactobacillus. Sun et al. [86] compared microbiota modifications in GD patients treated with MMI or PTU. The MMI group showed more Firmicutes at the phylum level, while the PTU group was characterized by higher abundance of Bacteroidetes. The microbial dysbiosis index (MDI) and the F/B ratio suggested that dysbiosis occurred in both drug-treated groups. Interestingly, GD treatment reduced some SCFA-producing bacteria. It has been reported that, upon PTU treatment, a higher percentage of patients had subtherapeutic drug levels than under MMI medication [87]. A possible explanation could stem from intrinsic microbial enzymatic activity. Noticeably, some bacterial strains possess trimethylamine monooxygenase, which can metabolize PTU the same way as liver flavin-dependent monooxygenase (FMO3) [18]. Yan et al. [88] reported that Prevotella might also affect the therapeutic efficacy of drugs for GD. Glucocorticoids and immunosuppressive drugs (azathioprine and mycophenolate) also used in the treatment of GO are known to affect microbiota composition, however data regarding specifically GO patients are lacking [34].
4.3 Thyroid cancerIt is accepted that dysbiosis has a carcinogenic effect on gastrointestinal cells, but its role on extraintestinal ones still needs to be ascertained. However, carcinogenesis relies mainly on two mechanisms: DNA damage and cellular apoptosis, on one side, inflammatory reactions and immune surveillance on tumor growth, on the other [25, 40]
In patients with TC or thyroid nodules, one study [89] showed an increase in gut microbial richness and diversity compared to healthy controls. Specifically, at phyla level, Firmicutes were increased in stool sample of TC patients, with an increase in Streptococcus and reduction in Butyricimonas and Lactobacillus [89]. Reduction of Butyricimonas and Lactobacillus can affect some products of bacterial metabolism, such as SCFAs and especially butyrate, important for its immunoregulatory effect. Therefore, their reduction could lead to increased cellular proliferation, and ultimately to a higher risk of cancer [89]. Another study [90] instead, showed a reduction in microbial richness, especially of the butyrate-producing gut microbiota, both in TC and in thyroid nodules with a high Thyroid Imaging Reporting and Data System (TI-RADS) score, meaning a higher ultrasound risk of being malignant. To note, in one of these cohorts [91], 2/3 of patients had lymph node metastases at diagnosis.
A further interesting finding is the existence of an intratumoral microbiota, mainly represented by intracellular bacteria found in cancer cells and peritumoral tissues. It has been shown that, in patients with thyroid cancer, tumoral and intestinal microbiota are different [92]. In detail, a prevalence of Proteobacteria was seen in thyroid samples, while Firmicutes were more represented in stools. Other studies [93, 94], instead, investigated the difference between tumoral and peritumoral microbiota composition. Results displayed a general lower microbic abundance in tumor tissue, associated with reduced richness and diversity indexes, while an increase in Sphingomonas was observed [94]. Noticeably, Sphingomonas abundance was higher in N1 stage compared to N0 stages [94]. Owing to these findings, Sphingomonas genus has been proposed as a marker to distinguish tumoral from peritumoral tissue and to suspect the presence of lymph node metastases [29, 37]. From a clinical point of view, thyroid micr
留言 (0)