
記住我



Out of 10,826 unique records, eight studies were eligible for at least one outcome analysis, accounting for 2610 patients. The duration of follow-up varied between 16 and 256 weeks. Figure 2 shows the flow diagram of the study selection process. Table 1 summarizes the key characteristics of the included trials.
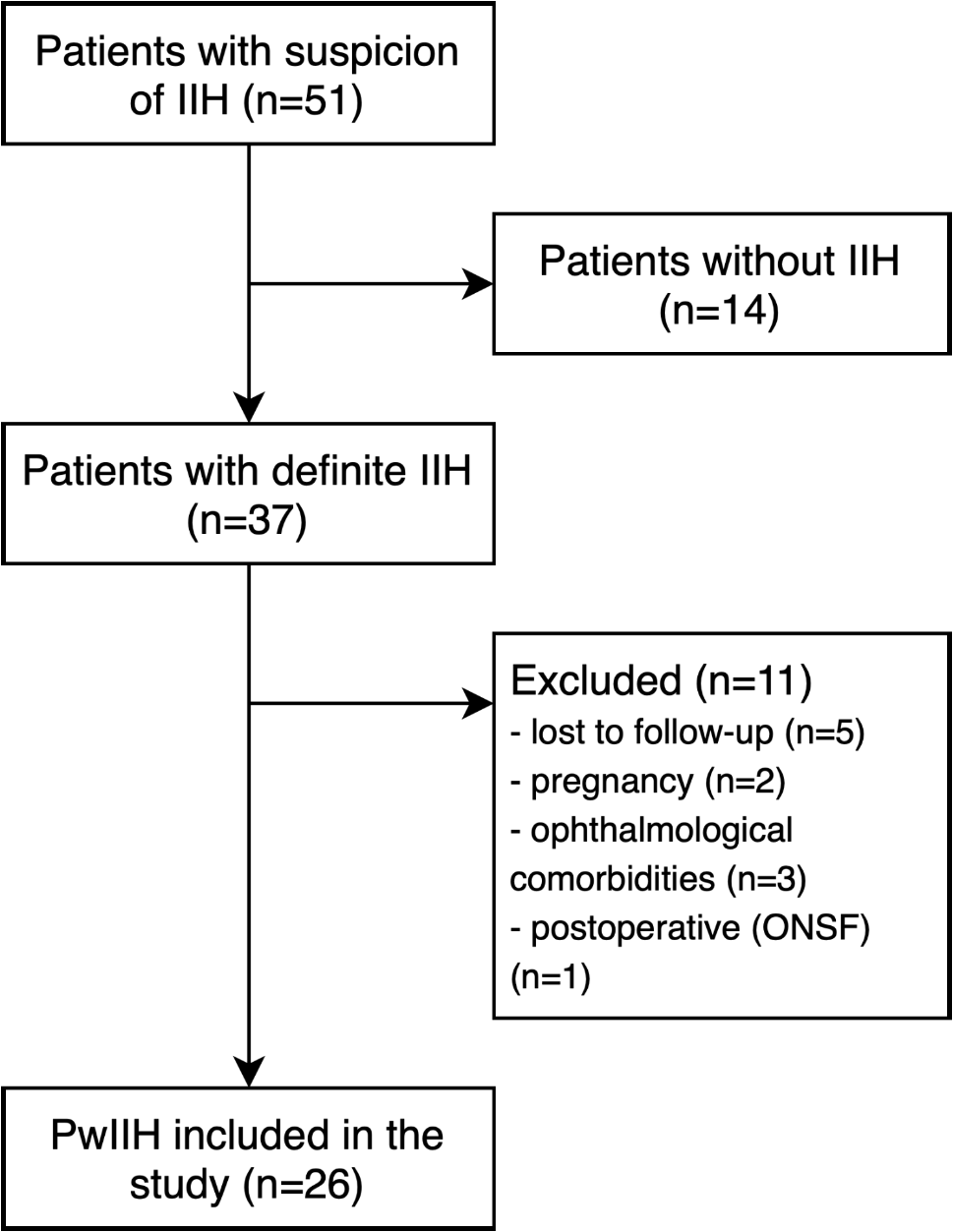
Fig. 2
Flow diagram of screened, included, excluded and analyzed studies for the European Headache Federation (EHF) critical re-appraisals and meta-analyses of oral drugs in migraine prevention
Table 1 Key characteristics of the included trialsNarrative description of topiramate in placebo-controlled trialsEpisodic migraineIn 2004, three MIGR studies (MIGR-001 [30], MIGR-002 [6], and MIGR-003 [31]) were published comparing different doses of topiramate with placebo in patients aged 12–65 years with 3 to 12 migraine attacks per month but no more than 15 monthly headache days. Participants with a maximum of two prior preventive treatments were allowed in the trial, but no concomitant use of another preventive drug was permitted. Primary endpoint was the reduction in mean monthly migraine frequency during the whole 26-week trial period, defined as the number of migraine attacks per month. Monthly migraine days (MMD) and the 50% responder rates were secondary endpoints.
The US-American MIGR-001 study compared three doses of topiramate (50 mg/day, 100 mg/day, 200 mg/day) to placebo [30]. All topiramate doses were associated with higher 50% responder rates compared to placebo (36% for 50 mg, 54% for 100 mg, and 52% for 200 mg vs. 23% for placebo). The two higher topiramate doses led to a significant reduction of MMD (from 6.4 to 3.7 for 100 mg; from 6.1 to 4.0 for 200 mg vs. from 6.1 to 5.2 for placebo), while the 50 mg group did not reach a significant difference. A total of 94 participants discontinued the trial due to adverse events (23% of patients in the topiramate groups vs. 9% of patients in the placebo group). The adverse events that most frequently led to withdrawal comprised of paresthesia, fatigue, nausea, anorexia, and memory and language problems.
The North American MIGR-002 study investigated the same topiramate doses as in the MIGR-001 trial [6]. The 100-mg and 200-mg groups met the primary endpoint, i.e., reduction in the number of monthly migraine attacks vs. placebo. All topiramate groups reached a higher 50% responder rate than placebo (39% for 50 mg, 49% for 100 mg, 47% for 200 mg vs. 23% for placebo). The reduction of MMD also favored topiramate 100 mg (-2.6) and topiramate 200 mg (-2.9) to placebo (-1.3). Withdrawal rates due to adverse events were 17% in the 50-mg group, 27% in the 100-mg group, and 21% in the 200-mg group vs. 12% in the placebo group. The most frequent adverse events leading to withdrawal were paresthesia, fatigue, diarrhea, and cognitive problems.
The multinational MIGR-003 study compared topiramate 100 mg/day or 200 mg/day with placebo and with propranolol 160 mg/day as an active control [31]. The comparison with propranolol is not included in the pooled quantitative analysis of this manuscript. The reduction in the mean number of monthly migraine attacks was significantly different to placebo in the 100-mg group but not in the 200-mg group. Moreover, the 100-mg group was superior to placebo in the reduction of MMD (-1.8 vs. -1.1 for placebo), while both topiramate groups had higher 50% responder rates than placebo (37% for 100 mg, 35% for 200 mg vs. 22% for placebo). Efficacy in the topiramate groups was comparable to propranolol. Adverse events led to treatment discontinuation in 37 patients with topiramate 100 mg (26%), 63 (44%) patients with topiramate 200 mg vs. 15 (10%) patients with placebo, most commonly paresthesia, fatigue, nausea, and cognitive problems.
Mei et al. randomly assigned patients with 2 to 6 migraine attacks per month to receive topiramate or placebo in a 1:1 ratio for 16 weeks [32]. The topiramate start dose was 25 mg/day, which was gradually titrated up to 100 mg/day by the end of the first trial month. The primary endpoint was the reduction of monthly migraine attacks from baseline to weeks 12 to 16. Topiramate was statistically superior to placebo in reaching the primary endpoint (topiramate: from 5.26 to 2.60; placebo: from 5.76 to 4.57). The number of MMD was not reported. In addition, the 50% responder rate was higher in the topiramate group compared to the placebo group (63% vs. 21%). In the topiramate group, 17 patients (29%) discontinued the trial due to adverse events vs. two (4%) in the placebo group. The most common adverse events leading to discontinuation included cognitive problems, paresthesia, weight loss, and somnolence.
Silberstein et al. evaluated the preventive efficacy and tolerability of topiramate 200 mg/day compared to placebo in patients with 3 to 8 migraine attacks per month [33]. Primary endpoint was the change in the mean number of monthly migraine attacks during the entire double-blind study phase. The study did not meet its primary endpoint. Indeed, the reduction in monthly migraine attacks between topiramate 200 mg (-1.42) and placebo (-1.04) was not statistically different. Also, the 50% responder rate was only numerically but not significantly different in the topiramate group compared to placebo (40% vs. 34%). Twenty-one (15%) patients in the topiramate group and four (5%) patients in the placebo group discontinued the trial due to adverse events, including fatigue, nausea, and paresthesia.
The most recent placebo-controlled trial for topiramate is the INTREPID study [37]. The study included high-frequency episodic migraine, defined as 9 to 14 MMD. The aim of the study was to investigate whether topiramate (100 mg/day) can prevent the progression to chronic migraine. Accordingly, the primary endpoint of this trial was the percentage of participants with chronic migraine at month 6. The study revealed similar transformation rates in the topiramate and placebo group and did not meet the primary endpoint. However, topiramate treatment resulted in a significant reduction of MMD compared with placebo (-6.6 vs. -5.3). The 50% responder rates were higher in the topiramate group, but the exact proportions were not reported. Twenty-one (11%) patients in the topiramate group and 18 (9%) patients in the placebo group discontinued the trial due to limiting adverse events. The most common adverse events were paresthesia, fatigue, and dizziness.
Chronic migraineTwo studies assessed the preventive properties of topiramate in patients with chronic migraine [34, 35].
The TOPMAT-MIG-201 trial enrolled 59 patients with chronic migraine defined as ≥ 15 MMD for at least three months before trial entry and ≥ 12 MMD during the 4-week baseline phase [34]. Participants were randomized 1:1 to receive either placebo or topiramate in a dose between 50 and 200 mg/day, according to the investigator’s judgement. The study was completed by 38 patients. Primary endpoint was the change in MMD from baseline to the last trial month (-3.5 in the topiramate group vs. + 0.2 in the placebo group). Participants receiving topiramate had significantly higher 50% responder rates compared to placebo (22 vs. 0%). Six (19%) patients in the topiramate group discontinued the study due to insufficient tolerability compared to three (11%) in the placebo group. Overall, the three most common adverse events were paresthesia, nausea, and dizziness.
The second study on chronic migraine by Silberstein et al. randomized 328 participants in a 1:1 ratio to placebo or topiramate with a target dose of 100 mg/day [35]. Overall, 182 subjects continued the study until the end. In this study, the definition of chronic migraine was ≥ 15 monthly headache days, at least 50% of which fulfilled the migraine criteria. The change of monthly migraine/migrainous days from baseline to the entire 16-week double-blind treatment phase was the primary endpoint. A migrainous day was defined as a day with moderate or severe headache with at least one feature among unilaterality, pulsatile character, photophobia and/or photophobia, nausea and/or vomiting, or worsening through physical activity. Treatment with topiramate led to a reduction of -6.4 migraine/migrainous days per month, while placebo reduced them by 4.7 days. The 50% responder rates, published in a subsequent publication, were 37.3% vs. 28.8% for topiramate vs. placebo and differences did not reach statistical significance [36]. In the topiramate group, 18 participants (11%) discontinued the trial due to adverse events, while this was the case for 10 subjects (6%) on placebo. The most frequent adverse events with topiramate were paresthesia, upper respiratory tract infections, and fatigue.
Quantitative analysisAll trials described above were included in the quantitative analysis of at least one outcome of interest. Table 2 summarizes key findings of the different meta-analyses.
Table 2 Topiramate compared to placebo for migraine prophylaxisMonthly migraine daysOur quantitative analysis for MMD included 2,361 participants from all eight studies (Fig. 3). Six studies provided direct information about MMD [6, 30, 31, 34, 35, 37]. For the remaining two [32, 33], we used the number of monthly migraine attacks as a surrogate parameter.
Fig. 3
Forest plot showing meta-analysis comparing topiramate with placebo for the reduction of monthly migraine days
Overall, the meta-analysis revealed a high certainty evidence that treatment with topiramate reduces migraine frequency over time with a mean difference of 0.99 days compared to placebo. Five studies were deemed at low risk of bias [6, 30, 31, 33, 35], and three studies at high risk of bias [30, 34, 37] (Fig. 4). Reasons for the low rating were mostly missing outcome data.
Fig. 4
Risk of bias ratings for the randomized controlled trials of topiramate vs. placebo included in this meta-analysis
Pairwise meta-regressions did not show different results for trials at high risk of bias compared with trials at a low risk of bias (Supplementary Material 2). Similarly, a subgroup analysis based on mean MMD at baseline and prior use of migraine preventive treatments revealed similar results as the primary analysis (Supplementary Material 2).
50% responder rateSix trials including 1,959 participants reported the 50% responder rates as an outcome [6, 30, 31, 33, 34, 36]. We found high certainty of evidence that topiramate increased the 50% responder rates (Fig. 5). Across these trials, the relative effect of topiramate compared to placebo was 1.61 (95% CI 1.29–2.01). One trial [34] was rated as high risk of bias and the remaining five as low risk of bias.
Fig. 5
Forest plot showing meta-analysis comparing topiramate with placebo for 50% responder rates
Separate subgroup analyses based on baseline migraine frequency, prior use of preventive medication, and risk of bias showed results consistent with the primary analysis (Supplementary Material 3).
Adverse events leading to discontinuationOverall, 322 out of 1,561 participants receiving topiramate within eight trials ended the study prematurely due to adverse events [6, 30,31,32,33,34,35, 37]. Topiramate led to higher discontinuation rates than placebo with a risk difference of 0.08 (95% CI 0.02–0.14) (Fig. 6). The certainty of evidence was deemed as high.
Fig. 6
Forest plot showing meta-analysis comparing topiramate with placebo for adverse events leading to discontinuation
Subgroup analyses based on risk of bias, migraine frequency, and previous preventive medication yielded similar results as the primary analysis (Supplementary Material 4).
留言 (0)