According to the American Society for Aesthetic Plastic Surgery (ASAPS), the placement of dermal fillers is the second most commonly performed minimally invasive cosmetic procedure in the USA. ASAPS data show that there is an increase in buttock augmentation procedures from 2015 to 2019 by 90.3% [1].
Gluteal cosmetic procedures can be surgical silicone implants, autologous fat grafting or local injection of injectable fillers. The most commonly used injectable for buttock augmentation includes: Hyaluronic acid, fluid silicone, Polyalkylimide Gel, Polyacrylamide Gel (PAAG) and Polymethylmethacrylate (PMMA) [2].
Injectable silicone is not approved by the US Food and Drug Administration for any esthetic procedure including facial and body contouring or enhancement [3].
Complications of gluteal cosmetic procedures include gluteal abscess, skin ulceration, granuloma, foreign body migration, acute and late onset pneumonitis and pulmonary embolism. Though rare, embolization of soft dermal fillers resulting in pulmonary embolism and death has been reported [4].
According to the ASERF task force, despite the growing popularity of gluteal fat grafting, significantly higher mortality rates appear to be associated with gluteal fat grafting than with any other esthetic surgical procedure. The Multi-Society Task Force for Safety in Gluteal Fat Grafting (ASAPS, ASPS, ISAPS, IFATS, ISPRES) recently released an urgent practice advisory in response to the alarming number of deaths still occurring from this procedure. The unusually high mortality rate from this cosmetic procedure is estimated to be as high as 1:3000, greater than any other cosmetic surgery [5].
Rapkiewicz et al. [6] presented a series of 10 deaths complicating gluteal procedures with the majority occurring in the setting of liposuction and gluteal fat transfer. They reported post-mortem autopsy findings of macroscopic pulmonary fat embolism.
Bejarano et al. [7] reported pulmonary complications related to the illegal use of injected silicone for cosmetic procedures. Silicone injection can cause complications similar to that seen in fat embolism inducing inflammation and immune response activation with consequent alveolar hemorrhage, diffuse alveolar damage and acute respiratory distress syndrome (ARDS).
Carolyn et al. [8] reported a case of acute pneumonitis after silicone injection for gluteal augmentation. The patient presented with hemoptysis, shortness of breath, and acute respiratory failure two days after the silicone injections. Her chest computed tomography (CT) showed predominantly basilar and peripheral Ground Glass Opacity (GGO) and bilateral pulmonary nodules. Her condition required ECMO and she improved with intravenous methylprednisolone 125 mg every 6 h.
Inayat et al. [9] reported that filler-induced non-thrombotic pulmonary embolism (NTPE) can be either mechanical obstruction of the pulmonary circulation or chemical inflammatory reaction with pneumonitis and alveolar hemorrhage. The precipitating factors include high-pressure injection, large filler volume injection, massage or trauma at the injection site and direct injection into a vein [10, 11].
Ng et al. [12] reported that, for decades, liquid injectable silicone has been used for correction of contour defect or soft-tissue augmentation. Medical-grade liquid silicone (polydimethylsiloxane) became the preferred inert material for cosmetic purpose due to its durability, lack of immunogenicity and thermal stability. However, it was found later that silicone can induce pulmonary embolism (silicone embolism syndrome: SES). It has been reported by several studies as a cause of acute pneumonitis with alveolar hemorrhage and ARDS [13].
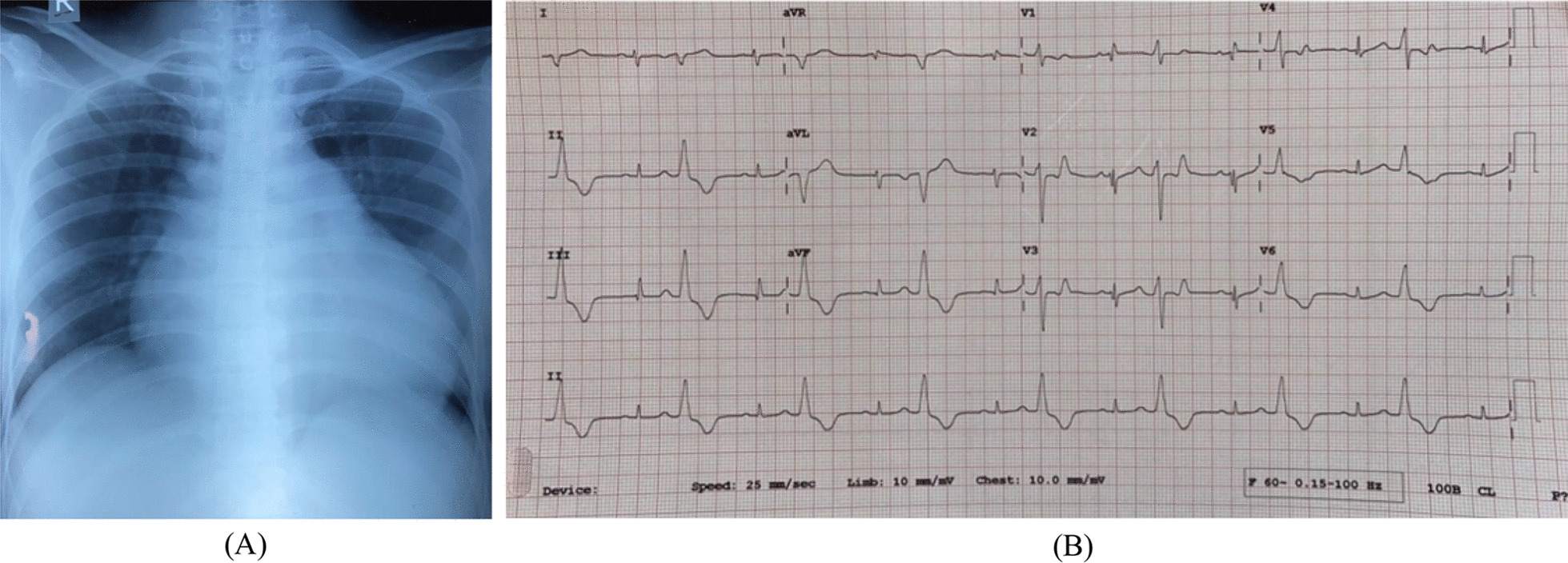
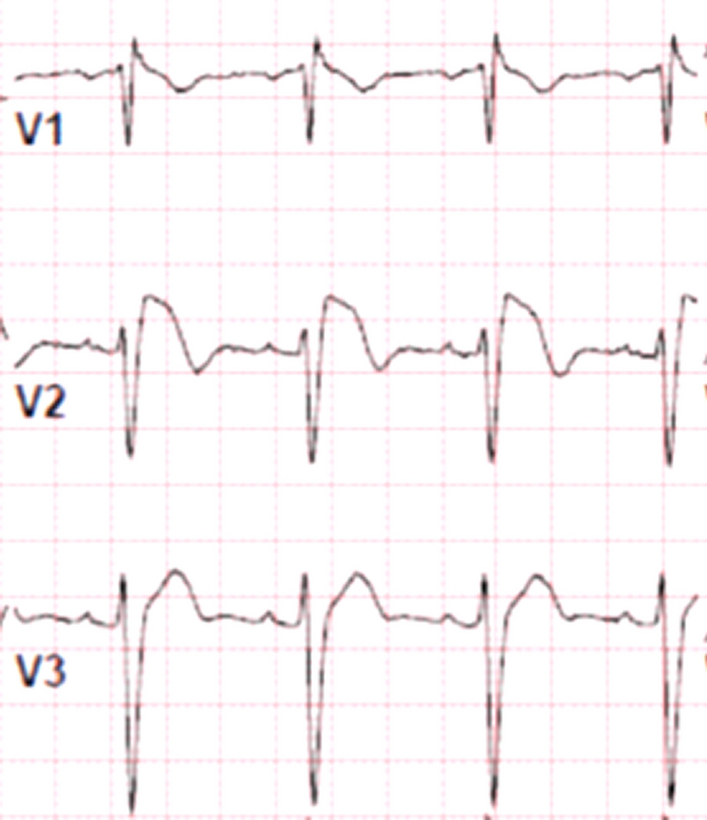
Cases of NTPE occurs typically in young females with recent history of gluteal cosmetic procedures. Presentation is mostly within few hours after the procedure, but may be late, with no evidence of DVT. Symptoms will range from mild dyspnea, cough and expectoration up to extreme difficulty in breathing with hemoptysis and signs of acute respiratory failure. Hemodynamics can be stable or the patient might be shocked with tachypnea and tachycardia. Chest auscultation might reveal crepitations of inflammatory secretions. Blood gases will indicate hypoxia and mild hypercapnia. Chest X-ray will show extensive pneumonic infiltrates. A 2-D echocardiogram might reveal severe pulmonary hypertension and RV dysfunction. Lung computed tomography (CT) can show diffuse alveolar infiltrates, bilateral GGO and pleural effusion. CT pulmonary angiography might not show evidence of acute venous thromboembolism. Bronchoscopy will show diffuse alveolar hemorrhages with no overt source of bleeding. Bronchoalveolar lavage fluid cytology may show macrophages and mixed inflammatory cells and negative cultures. Trans-bronchial lung biopsy shows lung parenchyma with intra-alveolar hemorrhage, macrophages and non-refractile vacuole like structures [14].
Fat embolism syndrome (FES) that might occur with liposuction and autologous fat grafting is classically characterized by the combination of a triad: acute respiratory failure, neurologic abnormalities, and a petechial rash. Patients presenting to the ER with sudden alteration in mental status should be questioned for recent surgical or invasive cosmetic procedures. FES should be considered even if the patient has no petechial rash. Brain magnetic resonance images (MRI) and lung CT should be ordered for these patients. Patient might have multiple cerebral white lesions on brain MRI [15].
Compared to the amount of filler used in facial procedures [2–5 cc], commonly used fillers or autologous fat transfers in the gluteal region usually involve up to 600 cc in each buttock. This large amount of filler in the gluteus muscles increases the likelihood of embolization. Moreover, application of these fillers in vascular regions of the gluteus muscles make embolization more likely [16].
According to the Multi-Society Task Force for Safety in Gluteal Fat Grafting, pulmonary fat embolism is the most common cause of mortality. The mechanism is fat entering the venous circulation after penetration of the gluteal veins. Autopsy findings in all mortality cases universally showed fat within the gluteal muscle. The Task Force has therefore concluded that fat should never be placed in the muscle. Fat should only be placed in the subcutaneous tissue. Operators should avoid deep injection, should use wide-bore syringe and blunt cannula, aspirate prior to each injection and use ultrasound-guided injection. Patients interested in gluteal augmentation through fat grafting or filler procedures should be informed of the risk of pulmonary fat or filler embolism which might end in death. They should be informed about the alternatives of these procedures that include silicone implant-based gluteal augmentation [5].
Treatment of a complicated case of filler pulmonary embolization and pneumonitis is based on limited experience as there is no published consensus. Patients with severe respiratory symptoms might be admitted to ICU and treated with massive IV steroids and antibiotics. The role of anticoagulants or thrombolytic therapy is controversial. Sedation and prone position, non-invasive or even invasive mechanical ventilation might be needed. ECMO might be considered in patients complicated by hemodynamic shock or severe ARDS and acute respiratory failure.



Comments (0)