
Remember me







Peripheral nerve injury (PNI) is a substantial clinical pain event with devastating consequences. Complications including the loss or partial recovery of motor/sensory function, chronic pain, and end target muscle atrophy exist in approximately 33% of patients with PNI.1,2 In the United States, more than 50,000 peripheral nerve repair surgeries are performed annually, with a spend of approximately $150 billion annually, and 87% of these costs provide no significant benefit.3,4 The most significant PNIs are those that result in a gap in nerve continuity. Segmental loss of nerve may permanently affect motor and sensory functions.5 Evidence indicates that stretching nerve ends to repair a nerve gap will decrease blood flow to jeopardize the health of the nerve.6 To overcome lengthy nerve gaps, the clinical criterion standard is sensory nerve autograft transplantation.7
As the most efficacious microsurgical approach, autografts are capable of bridging the nerve gap to restore nerve function by harvesting the sural and lateral antebrachial cutaneous nerves, etc.8 However, this technique is accompanied by adverse effects, such as donor nerve functional loss and painful neuromas occurring at the donor site. Moreover, the number of autologous expendable nerve grafts is limited.9
To overcome the disadvantages of donor adverse effects, the single-fascicle nerve graft concept has attracted attention. In 2011, Tzou et al10 reported that by using the Sprague-Dawley rat to set up a model of sciatic nerve defect, a single-fascicle nerve graft, compared with triple-fascicle, has the potential to achieve good functional regeneration. Siemionow et al11 claimed that this method results in more axons and myelin thickness than conventional grafts, and better functional recovery. These shreds of evidence indicate that a nerve graft, which is not proportional to the cross-section of the dissected nerve stump, might be available in clinical surgery. This possibility suggests that effective nerve gap repair might require certain peripheral nerve tissue rather than intact nerve fascicle or even cross-section–matched fascicles.
Nevertheless, the mentioned technique has a disadvantage of donor site injury, including wound healing complications, numbness, pain, and scar. In addition, a donor site might provide enough autograft for cross-section–matched fascicles. So, the indications of using a single-fascicle nerve are restricted. To overcome these drawbacks, we modified the Tzou's technique. Our study began with an emergency surgery, the diagnosis of which was left-sided frontal branch facial nerve dissection. The legal guardians agreed with surgery exploration but refused extra incision for harvesting autograft. Because the approximately 0.5-cm distance between nerve stumps caused tension postanastomosis, we adjusted measures to local conditions to longitudinally cut the nerve stump and harvest a partial nerve graft, as long as the nerve gap, to bridge nerve defects. The denervated frontal muscle recovered function and symmetry appearance compared with the normal side 13 months post–initial surgery. To test the feasibility of this modification, we referred to Tzou's work to set up a similar animal model to compare the effectiveness of the criterion standard cross-sectional–matched autograft and the semifascicle graft. In consideration of neuroma and scar formation, nerve conduits (NCs) serve to direct nerve grafts and protect the nerve from the surrounding tissue.
MATERIALS AND METHODS Section 1: Case ReportThe patient was 2.7 years old when he presented to the emergency room. The primary diagnosis was a laceration lateral to the left eyebrow. Because of the specific position of the wound, the surgeon (H.X.) performed a physical examination and found no obvious asymmetry of the eyebrows when the eyes were closed, but the affected side was obviously lower than the healthy side when the eyebrows were lifted. The frontalis on the affected side exhibited no contraction (Figs. 1A, B).
 FIGURE 1:
FIGURE 1: Case report: A 2.7-year-old patient was diagnosed with laceration at first. Because of the specific position of the wound, the surgeon (H.X.) performed a physical examination; no obvious asymmetry of the eyebrows was found when the kid closed the eyes (A), but the affected side was obviously lower than the healthy side when the kid lifted the eyebrows. In addition, the frontalis of the affected side was noticed to have no contraction (B).
Because the patient was relatively young, an electromyography test failed to be performed initially and also during follow-up. Therefore, transection of the left frontal branch of the facial nerve was suspected. The legal guardian agreed to an exploratory operation but required that there would be no extra wound caused by harvesting autograft for nerve bridging when necessary.
Surgical ProceduresAfter thorough debridement and rinsing, we failed to identify an intact nerve branch around the wound. We then explored the proximal stump of the frontal branch of the facial nerve, which was approximately 1.5 cm on the lateral side of the sentinel vein (Fig. 2A; white arrow: proximal nerve stump; black arrow: sentinel vein). The distal side was located at the corresponding position (Fig. 2B; white arrow: distal nerve stump). The distance between the nerve stumps was approximately 0.5 cm. We longitudinally and equally dissected the distal stump into 2 semifascicles for approximately 1.0 cm (Fig. 2C), then harvested 1 semifascicle as a nerve graft to bridge the nerve gap by using 11-0 prolene (Fig. 2D). The wound was closed and well dressed.
 FIGURE 2:
FIGURE 2: A, During operation, we explored the proximal stump of the frontal branch of facial nerve, which was approximately 1.5 cm on the lateral side of the sentinel vein (white arrow: proximal nerve stump; black arrow: sentinel vein). B, The distal side was located on the corresponding position (white arrow: distal nerve stump). C and D, The diagram of the surgery.
Postoperative CareThe patient received anti-infective and anti-inflammatory drugs, and dressing changes were made postoperatively. He was asked to have a subsequent visit every 2 months and perform rehabilitation at home.
Section 2: Animal Study Animal and AnesthesiaAll animal care procedures complied with the ethics committee regulations of Shanghai Jiao Tong University, Shanghai, China. Thirty-six male Sprague-Dawley rats weighing 250–300 g were used in this study. Chloral hydrate (4%, 8 mL/kg intraperitoneal) was used for anesthesia. All surgeries were performed under sterile conditions.
GroupsAll rats were randomly divided into 3 groups (12 rats per group).
Group A was the intact sciatic nerve graft group (intact fascicle). First, we dissected and exposed the right sciatic nerve. Second, a 1.0-cm sciatic nerve segment was harvested. Third, the nerve segment was sutured back to this location using 10-0 sutures. Fourth, the skin wound was closed with 4-0 sutures. Fifth, on the left side, a skin incision was created that corresponded to the one on the right side and then closed with 4-0 sutures as a sham surgery control.
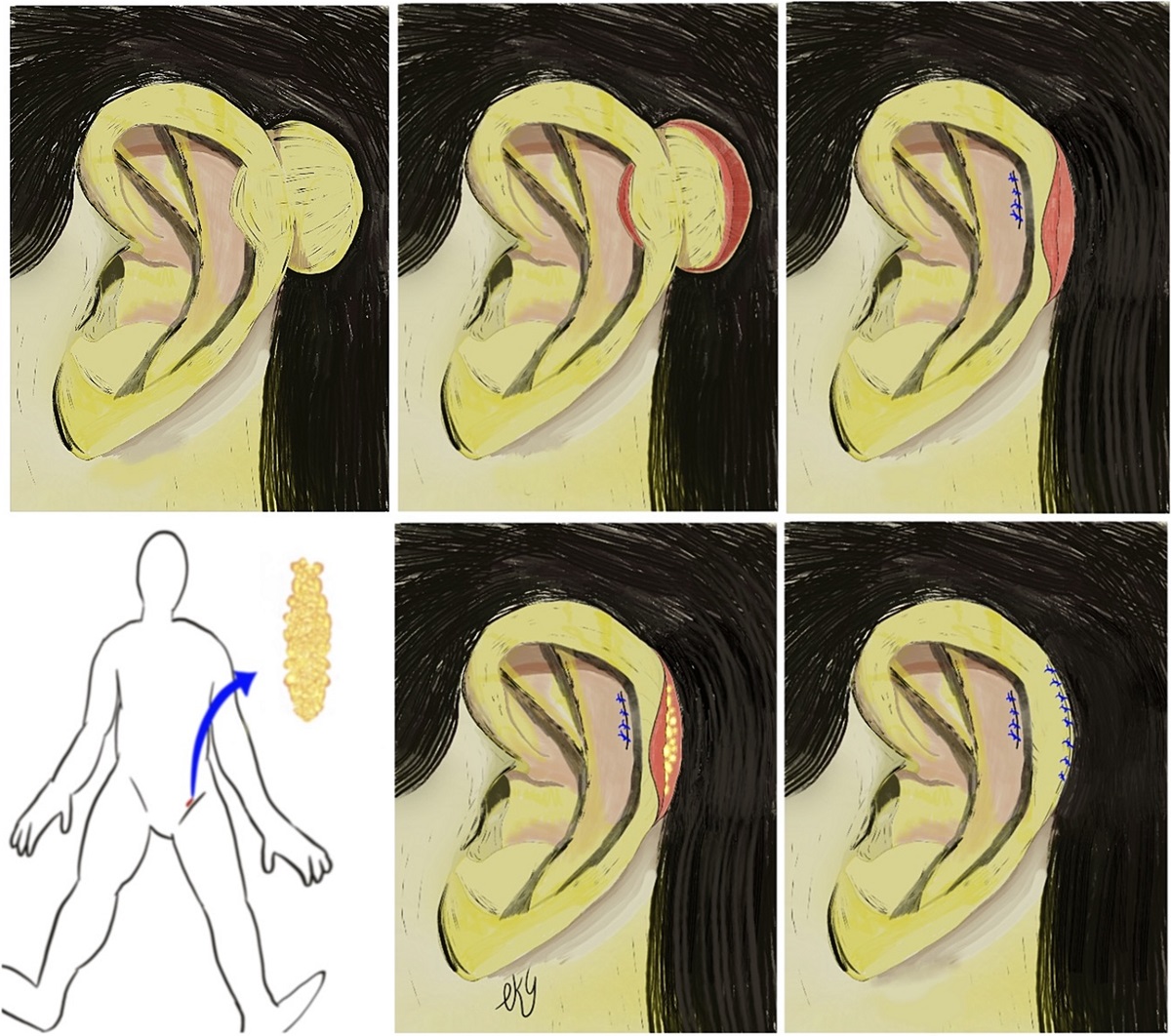
Group B was the semifascicle sciatic nerve graft group (semifascicle), which was similar to that in group A. A different procedure was performed after harvesting the 1.0-cm sciatic nerve segment. The distal stump was longitudinally and equally dissected into 2 semifascicles for approximately 1.0 cm; one part was harvested to bridge nerve defect (Fig. 3A).
 FIGURE 3:
FIGURE 3: A, Setting up the semifascicle nerve graft animal model. B, Setting up the semifascicle + NC animal model. C, The NC used in the current study. D, Harvest the bridged nerve 8 weeks postsurgery.
Group C comprised the semifascicle sciatic nerve graft plus NC group (semifascicle + conduit); the procedures were similar to those performed for group B. The nerve graft was placed inside the NC (Fig. 3B). We used a poly-l-lactic acid microtube array sheet conduit (Fig. 3C). The preparation method was previously described.12
Each group was further randomly divided into 2 subgroups (6 per group) to create 4- and 8-week groups, which were euthanized after 4 and 8 weeks, respectively, to facilitate histological examination.
Wet Weight MeasurementThe 8-week subgroups included in groups A–C were tested. To assess denervation atrophy of the gastrocnemius muscle, the gastrocnemius muscles were harvested after transcardial perfusion with paraformaldehyde (4%), with the animals under deep anesthesia; the wet muscle weight was then measured immediately. The data are presented as the ratio of wet weight of experimental side/control side, ie, the right side/left side ratio.
HistologyThe specimens were fixed in neutral buffered formalin (10%), decalcified in Formical-2000 (Decal Chemical Corp, Suffern, NY), and embedded in paraffin. Immunostaining was performed on longitudinal 5-μm-thick sections of the nerve. After blocking with albumin, mouse polyclonal antibodies against the S100 protein (1:1000, Dakopatts AB) and mouse monoclonal antibodies against beta-tubulin III (1:1000, Sigma-Aldrich) were applied for 12 hours at 4°C. After rinsing in 0.01 M phosphate-buffered solution, secondary goat anti–mouse antibodies Alexa Fluor 568 and Alexa Fluor 488 (1:300; Molecular Probes, Europe BV, Leiden, Netherlands) were applied for 1 hour at room temperature in the dark. The slides were coverslipped with Vectashield mounting medium after counterstaining of the nuclei with 4′,6-diamidino-2-phenylindole (Vector Laboratories, Burlingame, CA). Staining specificity was tested by omission of primary antibodies and examined under a fluorescence microscope (10× magnification, IX81; Olympus, Center Valley, PA).13
Neural tissue areas were calculated using the Image-Pro Plus software (version 4.5; Media Cybernetics, Silver Spring, MD). Only the areas positively stained with tubulin were counted. For counting and analysis of nerve fibers, images were acquired at 400× magnification. The nerve fibers were manually counted.12
Behavior TestsEight-week subgroups included in groups A–C were tested weekly for mechanical pain and temperature.
Mechanical Pain Sensory TestThe reaction time of the mechanical foot contraction reflex was measured to test the pain sensory recovery. Reaction time was recorded using an electronic von Frey pain meter. Rats were placed on a metal screen and covered with a Plexiglas box. After 30 minutes of adaptation, the hindlimb paws of the rats were stimulated with 10.0 g. The time from the beginning of stimulation to the appearance of the hind-paw lifting was recorded. Each animal was stimulated 3 times at intervals of 10 minutes, and the average of the results was obtained.
Sensory Temperature TestMeasurements were performed weekly using a plantar thermal stimulation meter. In a quiet environment, the indoor temperature was maintained at 25°C. Rats were placed in a Plexiglas box with a 6-mm thick glass plate underneath. After 30 minutes of adaptation, the rats were stimulated with an infrared beam in the middle of the plantar. The latency period was recorded from the beginning to the appearance of the hindlimb lifting. The automatic cutoff time was 20 seconds to prevent skin burns. Each animal was measured 3 times at intervals of 10 minutes, and the average value was calculated.13
Statistical AnalysisData were analyzed using GraphPad Prism software (Prism 6; GraphPad Software, Inc). All values are expressed as mean ± standard deviation. One-way analysis of variance was used to evaluate the survival percentages and vessel densities among the groups. The Kruskal-Wallis H test was used for data that were not normally distributed, after which Dunn test was performed. The probability (P) value of less than 0.05 was considered statistically significant.
RESULTS Section 1: Case ReportThe patient recovered without any complications and was discharged from the hospital 1 day later. The frontalis of the affected side exhibited contraction at approximately 2 months postsurgery (Video 1, Supplemental Digital Content, https://links.lww.com/SAP/A885). An obvious frontalis contraction was observed at 6 months. Thirteen months after the initial surgery, no obvious asymmetry of the bilateral frontalis contraction and eyebrows was observed. However, soft tissue depression along the left-side orbit was noticed, which might require further plastic surgery (Figs. 4A, B, Video 2, Supplemental Digital Content, https://links.lww.com/SAP/A886).
 FIGURE 4:
FIGURE 4: A and B, Thirteen months post–initial nerve repair surgery. No obvious asymmetry of bilateral frontalis contraction and eyebrows were found. However, the soft tissue depression along the left-side orbit was noticed, which might require further plastic surgery.
Section 2: Animal Study Effect of Semifascicle Bridging Method on Axon RegenerationGross observation indicated that 8 weeks postsurgery, the semifascicle graft (with or without NC) recovered its diameter, which was close to the normal proximal part (Fig. 3D). Myelinated axons were observed by immunostaining of the distal nerve stump.
The 4-week postsurgery intact fascicle group (1.53 ± 0.25 mm2) exhibited a larger neurotissue area than those of the semifascicle (1.23 ± 0.10 mm2, P = 0.02) and semifascicle + conduit groups (0.85 ± 0.17 mm2, P < 0.0001). The size of the semifascicle group was larger than that of the semifascicle + conduit group (P = 0.004, Figs. 5A, B). Neurofilament quantity analysis indicated that the intact fascicle group (4592 ± 397.0) had a larger neurotissue area than the semifascicle (3759 ± 369.9, P = 0.003) and semifascicle + conduit groups (3137 ± 272.2, P < 0.0001). The size of the semifascicle group was larger than that of the semifascicle + conduit group (P = 0.02, Figs. 5A, C). The S100-stained Schwann cells presented higher numbers than those of the intact fascicle and semifascicle + conduit groups (Fig. 5A).
 FIGURE 5:
FIGURE 5: A–C, The 4-week postsurgery intact fascicle group (1.53 ± 0.25 mm2) had a larger neurotissue area than the semifascicle group (1.23 ± 0.10 mm2, P = 0.02) and semifascicle + conduit group (0.85 ± 0.17 mm2, P < 0.0001). The semifascicle group was larger than the semifascicle + conduit group (P = 0.004). Neurofilament quantity analysis indicated that the intact fascicle group (4592 ± 397.0) has a larger neurotissue area than those of the semifascicle group (3759 ± 369.9, P = 0.003) and semifascicle + conduit group (3137 ± 272.2, P < 0.0001). The semifascicle group was larger than that semifascicle + conduit group (P = 0.02). The S100-stained Schwann cells presented a higher amount than those of the intact fascicle and semifascicle + conduit groups. ns indicates no significant difference. ****P < 0.0001; **P < 0.01; *P < 0.05.
The 8-week postsurgery intact fascicle group (1.15 ± 0.09 mm2) possessed a larger neurotissue area than those of the semifascicle (0.82 ± 0.08 mm2, P < 0.0001) and semifascicle + conduit groups (0.93 ± 0.08 mm2, P = 0.002). The semifascicle and semifascicle + conduit groups were not significantly different (P = 0.10, Figs. 6A, B). Neurofilament quantity analysis indicated that the intact fascicles (2323 ± 280.8), semifascicles (2194 ± 223.3), and semifascicle + conduit groups (2131 ± 159.0) were not significantly different (P > 0.05, Figs. 6A, C). The semifascicle +conduit group had higher Schwann cell numbers than those of the intact fascicle and semifascicle groups (Fig. 6A).
 FIGURE 6:
FIGURE 6: A–C, The 8-week postsurgery intact fascicle group (1.15 ± 0.09 mm2) has a larger neurotissue area than those of the semifascicle group (0.82 ± 0.08 mm2, P < 0.0001) and semifascicle + conduit group (0.93 ± 0.08 mm2, P = 0.002). The semifascicle and semifascicle + conduit groups had no significant difference (P = 0.10). Neurofilament quantity analysis indicated that intact fascicle (2323 ± 280.8), semifascicle (2194 ± 223.3), and semifascicle + conduit groups (2131 ± 159.0) had no significant difference (P > 0.05). The semifascicle + conduit group had a higher Schwan cell amount than that of the intact fascicle and semifascicle group. ns indicates no significant difference. ****P < 0.0001; **P < 0.01.
Effect of Semifascicle Bridging Method on Muscle RecoveryThe wet weight measurement of the gastrocnemius muscle revealed that the 8-week post-PNI and graft bridging, intact fascicle group (44.67% ± 3.56%) exhibited no significant differences from the semifascicle group (49.33% ± 3.50%, P = 0.07), but was higher than that of the semifascicle + conduit (28.67% ± 3.08%, P < 0.0001). The gastrocnemius muscle of the semifascicle group was heavier than that of the semifascicle + conduit group (P < 0.0001, Fig. 7A).
 FIGURE 7:
FIGURE 7: A, Muscle wet measurement shows that 8 weeks after setting up the animal model, the intact fascicle group (44.67% ± 3.56%) had no significant difference with the semifascicle group (49.33% ± 3.50%, P = 0.07), but had higher significance than the semifascicle + conduit group (28.67% ± 3.08%, P < 0.0001). The semifascicle group was heavier than the semifascicle + conduit group (P < 0.0001). B, Von-fray and (C) thermal test results, which present no significant difference among the 3 groups at 8 week. ns indicates no significant difference. ****P < 0.0001.
The Behavior Tests Among 3 GroupsThe von Fray tests showed no significant differences between 2 of the 3 groups (P > 0.05, Fig. 7B). The data indicated that no difference was observed between weeks 1 and 3. The intact fascicle group displayed shorter retraction time from weeks 4 to 8, but no trend was observed in the other 2 groups.
The thermal test also showed no significant differences between 2 of the 3 groups (P > 0.05, Fig. 7C). The data indicated that no difference was observed between weeks 1 and 2. The intact fascicle group exhibited shorter retraction time from weeks 4 to 8 compared with those of the other 2 groups. The semifascicle + conduit group tended to have shorter retraction times compared with those of the semifascicle group.
DISCUSSIONA major principle in peripheral nerve reconstruction is the absence of tension.14 When there is a segmental nerve gap, primary nerve repair should be precluded.15 Instead, most reports suggest that the criterion standard of nerve reconstruction is nerve autografts.16 These autografts, such as sural nerve and the superficial branch of the radial nerve, are capable of providing Schwann cells, providing intact endoneurial tubes, and guiding the regeneration of the nerve axons. However, the risks of neuroma formation, sensory loss, and skin scar formation at the donor sites limit nerve autograft use.17,18
The single-fascicle graft study conducted by Siemionow et al11 provides a direction for minimizing the complications of harvesting a nerve autograft. The graft covers 25%–50% of the cross-sectional area of the nerve stump and results in adequate functional recovery. Our emergency case report unveiled the feasibility of a semifascicle nerve graft, which could not only recover function but also treat the injury site as both donor and recipient sites to avoid donor site damage. The patient recovered nerve function from 3 months postsurgery and exhibited satisfactory function at 13 months postsurgery. Although the inferior part of the frontalis muscle had atrophy, this technique still presented the advantage of avoiding donor site and related complications. According to the literature, the relatively pure function of the frontal branch of the facial nerve and the short distance to the target tissue are more likely to permit reconnection.19 Nevertheless, this case report demonstrated the clinical translational value of this technique as a preliminary, clinical approach study. The Wallerian degeneration of the peripheral nerve axon indicates that all axons of the distal stump would degenerate then the axons inside the proximal stump would regenerate through the distal stump to innervate the targeted organ.20 Thus, the harvested part of the tissue of the distal nerve stump would not interfere with the axon regeneration from the proximal to distal stump. Meanwhile, the semifascicle graft modification does not require a donor site; in contrast, the recipient site is also the donor site.
In the validated animal study, histological analysis revealed that the semifascicle group had a similar axon number as that of the intact fascicle group at week 8 postsurgery. Muscle wet weight measurement and behavior analysis also indicated no significant difference between the semifascicle and intact fascicle groups. These results were similar to those of previous studies.10,11 Cross-sectional unmatched nerve grafts were associated with acceptable axonal regeneration and functional recovery.
In comparison with trunk grafts, which have limited prognosis because of central fibrosis, the interfascicle graft provides a better outcome.18,21 Because of faster diffusion and revascularization, thinner grafts survive more easily posttransplantation.22 This mechanism supports the feasibility of relatively smaller and thinner formation of semifascicle grafts. In addition to this mechanism, Schwann cells work as neurotropic and neurotrophic factors to guide axon growth.23 Similar to previous research, the epineurium of the nerve graft was removed in this study. Certain tissue structures are believed to be more accessible for Schwann cells to reach the sprouting axons.10,11 The mentioned mechanisms might explain the feasibility of semifascicle nerve grafts.
The unsatisfactory results in the semifascicle + conduit group reflected that the NC functions as a “double-edge sword.” On the one hand, the NC provided sufficient supportive and protective effects, which preserved the neurotissue area from being crushed to contraction by the surrounding tissue. On the other hand, poor regeneration status at week 4 postsurgery and lightest muscle wet weight indicated that the NC used in this study had a negative effect in promoting nerve regeneration, which might be due to the inhibition of nutrient exchange. However, a limitation of the study is that it fails to preclude the possibility of using an NC, because different kinds of NCs present both positive and negative functions in different animal and clinical studies.24–27 The conduit properties, including permeability, flexibility, physical inertness, and rate of degradation, are all important factors that can potentially impact the nerve regeneration result.28 Therefore, the effect of NC used in improving the outcome of semifascicle nerve grafts requires further investigation.
In addition, we acknowledge other limitations. First, the nerve gap was approximately 1 cm, which is relatively short. A longer gap length should be studied to investigate the regenerative ability of semifascicle nerve grafts. Second, the loss of semifascicle is correlated with the decreased number of nerve fiber and is proposed to have restricted clinical indications. Third, simply by the nature of the semifascicle graft, half of the target nerve might be unavailable for reinnervation. Furthermore, intrafascicular dissection of the distal nerve could have additional fibrosis as a possibility. Thus, further studies involving different nerve injury sites and complex nerve fibers of both injured nerves and nerve grafts, as well as fibrosis analysis, are required to verify the efficacy of the semifascicle graft.
CONCLUSIONSThis study demonstrates the feasibility and clinical value of a semifascicle nerve graft. This method could not only achieve acceptable muscle wet weight, behavioral recovery, and axonal regeneration but also treat the injured site as both donor and recipient sites to avoid donor site damage and associated complications.
However, clearer indications and contraindications are expected in clinical practice, such as the length of the nerve gap, the type of nerve injury, and the types of nerve fibers involved in the injured nerves. Therefore, further animal and clinical studies are required to elucidate these current concerns.
REFERENCES 1. Noble J, Munro CA, Prasad VS, et al. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma. 1998;45:116–122. 2. Atkins S, Smith KG, Loescher AR, et al. Scarring impedes regeneration at sites of peripheral nerve repair. Neuroreport. 2006;17:1245–1249. 3. Millesi H. Bridging defects: autologous nerve grafts. Acta Neurochir Suppl. 2007;100:37–38. 4. Taylor CA, Braza D, Rice JB, et al. The incidence of peripheral nerve injury in extremity trauma. Am J Phys Med Rehabil. 2008;87:381–385. 5. Gregory H, Phillips JB. Materials for peripheral nerve repair constructs: natural proteins or synthetic polymers? Neurochem Int. 2021;143:104953. 6. Trumble TE, McCallister WV. Repair of peripheral nerve defects in the upper extremity. Hand Clin. 2000;16:37–52. 7. Gravvanis AI, Lavdas A, Papalois AE, et al. Effect of genetically modified Schwann cells with increased motility in end-to-side nerve grafting. Microsurgery. 2005;25:423–432. 8. Ruijs ACJ, Jaquet JB, Kalmijn S, et al. Median and ulnar nerve injuries: a meta-analysis of predictors of motor and sensory recovery after modern microsurgical nerve repair. Plast Reconstr Surg. 2005;116:484–494 discussion 495–486. 9. McCallister WV, Cober SR, Norman A, et al. Using intact nerve to bridge peripheral nerve defects: an alternative to the use of nerve grafts. J Hand Surg Am. 2001;26:315–325. 10. Tzou CJ, Aszmann OC, Frey M. Bridging peripheral nerve defects using a single-fascicle nerve graft. Plast Reconstr Surg. 2011;128:861–869. 11. Siemionow M, Zielinski M, Meirer R. The single-fascicle method of nerve grafting. Ann Plast Surg. 2004;52:72–79. 12. Wang Y, Wang W, Wo Y, et al. Orientated guidance of peripheral nerve regeneration using conduits with a microtube array sheet (MTAS). ACS Appl Mater Interfaces. 2015;7:8437–8450. 13. Xu H, Chen J, Feng Z, et al. Shortwave infrared fluorescence in vivo imaging of nerves for minimizing the risk of intraoperative nerve injury. Nanoscale. 2019;11:19736–19741. 14. Millesi H, Meissl G, Berger A. The interfascicular nerve-grafting of the median and ulnar nerves. J Bone Joint Surg Am. 1972;54:727–750. 15. Boyd KU, Nimigan AS, Mackinnon SE. Nerve reconstruction in the hand and upper extremity. Clin Plast Surg. 2011;38:643–660. 16. Fox IK, Mackinnon SE. Adult peripheral nerve disorders: nerve entrapment, repair, transfer, and brachial plexus disorders. Plast Reconstr Surg. 2011;127:105e–118e. 17. Ray WZ, Mackinnon SE. Management of nerve gaps: autografts, allografts, nerve transfers, and end-to-side neurorrhaphy. Exp Neurol. 2010;223:77–85. 18. Beris A, Gkiatas I, Gelalis I, et al. Current concepts in peripheral nerve surgery. Eur J Orthop Surg Traumatol. 2019;29:263–269. 19. Scheib J, Hoke A. Advances in peripheral nerve regeneration. Nat Rev Neurol. 2013;9:668–676. 20. Conforti L, Gilley J, Coleman MP. Wallerian degeneration: an emerging axon death pathway linking injury and disease. Nat Rev Neurosci. 2014;15:394–409. 21. Millesi H. Techniques for nerve grafting. Hand Clin. 2000;16:73–91 viii. 22. Almgren KG. Revascularization of free pheripheral nerve grafts. An experimental study in the rabbit. Acta Orthop Scand Suppl. 1975;154:1–104. 23. Madison R, da Silva CF, Dikkes P, et al. Increased rate of peripheral nerve regeneration using bioresorbable nerve guides and a laminin-containing gel. Exp Neurol. 1985;88:767–772. 24. Nakamura Y, Takanari K, Ebisawa K, et al. Repair of temporal branch of the facial nerve with novel polyglycolic acid-collagen tube: a case report of two cases. Nagoya J Med Sci. 2020;82:123–128. 25. Binnetoglu A, Demir B, Akakin D, et al. Bacterial cellulose tubes as a nerve conduit for repairing complete facial nerve transection in a rat model. Eur Arch Otorhinolaryngol. 2020;277:277–283. 26. Niimi Y, Matsumine H, Takeuchi Y, et al. A collagen-coated PGA conduit for interpositional-jump graft with end-to-side neurorrhaphy for treating facial nerve paralysis in rat. Microsurgery. 2019;39:70–80. 27. Sand JP, Park AM, Bhatt N, et al. Comparison of conventional, revascularized, and bioengineered methods of recurrent laryngeal nerve reconstruction. JAMA Otolaryngol Head Neck Surg. 2016;142:526–532. 28. Muheremu A, Ao Q: Past, present, and future of nerve conduits in the treatment of peripheral nerve injury. Biomed Res Int. 2015, 2015:237507, 1, 6.
Comments (0)