
Remember me




Lung cancer (LC) is one of the leading causes of death in the world with more than 1.8 million deaths.1 Recently, there were improvements in LC management and minimally invasive surgical approaches with a reduction of mortality.2–4 Unfortunately, the postoperative pulmonary complication (PPC) rate is between 29.9% and 36.6% in the elderly population depending on the type of operation (segmentectomy, lobectomy, or pneumonectomy).5,6 The decrease in physical function in survivor patients with LC (PWLC) was also reported up to 2 years after surgery.7 Investigating the potential effect of inspiratory muscle training (IMT) on physical capacity is important due to the inversed correlation between physical capacity and the risk of death in PWLC.8,9 One focal point of PWLC surgery was respiratory muscle weakness.10,11 Indeed, the inspiratory muscle weakness induces impairment of cough, chest compliance, and physical capacity, and was associated with PPCs.12–16 To address these postoperative issues, IMT has emerged.17
Several systematic reviews with metanalysis showed the effectiveness of preoperative IMT in PWLC, but evidence of postoperative IMT (P-IMT) was scattered.18,19 Moreover, guidelines for dosing of P-IMT such as intensity, frequency, and time are not yet understood.
This systematic review was conducted, first, to summarize the effects of P-IMT on PPCs, physical capacity, maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), quality of life (QoL), physical activity (PA) level, hospital length of stay, and lung function after LC surgery. Second, the settings of the programs of P-IMT were also summarized in PWLC after surgery.
METHODSThe Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines were used to conduct this review.20
Literature SearchFour electronic databases were used for searching: PubMed, EMBASE, Cochrane library, and CINAHL. The equation of searching strategy in PubMed was based on PICO criteria and as follows: (“inspiratory muscle training”[Title/Abstract]) OR (IMT[Title/Abstract]) OR (“respiratory muscle training”[Title/Abstract]) AND (lung* AND (carcinogen* OR sarcom* OR tumor* OR tumour* OR carcinoma* OR cancer* OR neoplasm*)) AND (“postoperative” OR “post-surgery”). The equation was adapted to the other databases. The searching and screening were conducted independently by 2 reviewers (N-M. N. and G. R.). There was no publish date limitation for the search.
Study SelectionStudies were selected based on the following inclusion criteria: (1) the main purpose of studies was to investigate the effect of IMT in the postoperative LC population; (2) randomized controlled trial (RCT) including sham/control groups; (3) outcomes including at least one of following measures: PPCs, 6-minute walk test (6MWT), MIP, MEP, QoL questionnaires, PA level, hospital length of stay, and lung function.
Exclusion criteria were: (1) non-English language, (2) studies including preoperative IMT intervention, and (3) inclusion of diseases other than LC.
After removing duplicated studies with Endnote,21 2 independent reviewers (N-M.N. and G.R.) screened all potential studies by title and abstract. Then a full test reading was performed with selected studies. The final list of included studies was discussed and confirmed by consensus.
Quality AssessmentThe quality of studies was checked by the online Physiotherapy Evidence Database (PEDro) website and then assessed again by 1 reviewer (N-M.N.). The PEDro scale includes 11 items with a score of 0 or 1.22 Item 1 (eligible criteria) is not included in the cumulative score; thus, the maximal score was 10. The higher the score, the better the internal validity. These items satisfied the core set of items for RCT quality assessment.23 The levels of quality were divided into 3 groups: good (>6), fair (4-5), and poor (≤3).24
Data ExtractionThe extracted data from all included studies were: (1) characteristics of demographic data (sample size, age, body mass index (BMI), smoking, and MIP); 2) type of surgery; 3) intervention program of study and control groups (method, duration, and starting point); and (4) outcomes (PPCs, 6MWT, Vo2peak, MIP, MEP, QoL, hospital length of stay, and spirometry). Data extraction was conducted independently by 2 reviewers. The final table of data was cross-checked.
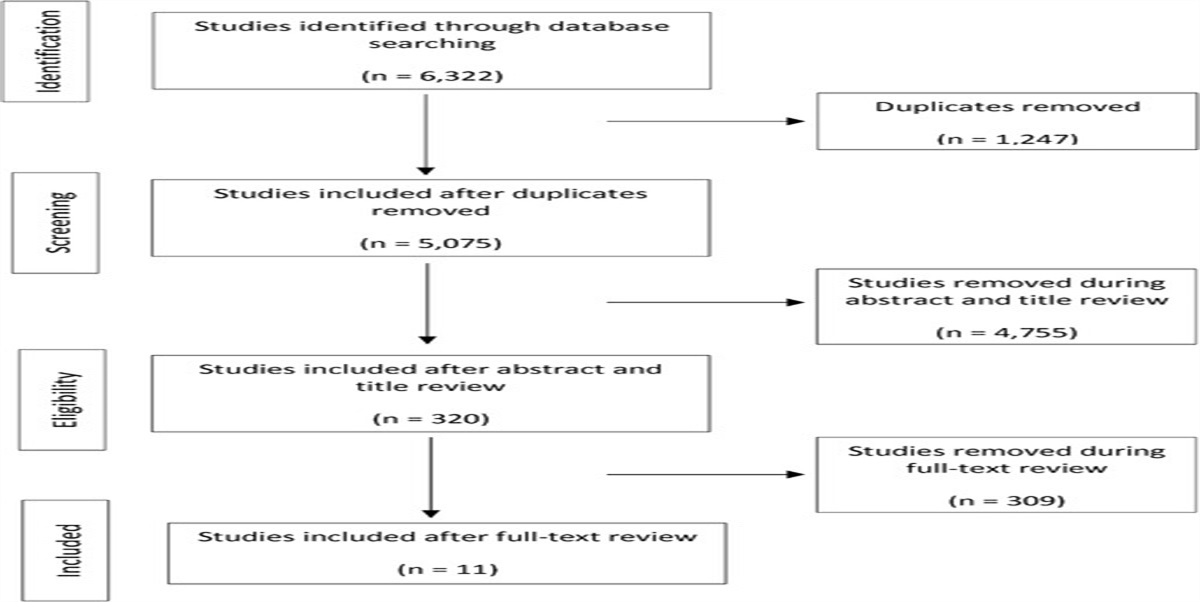
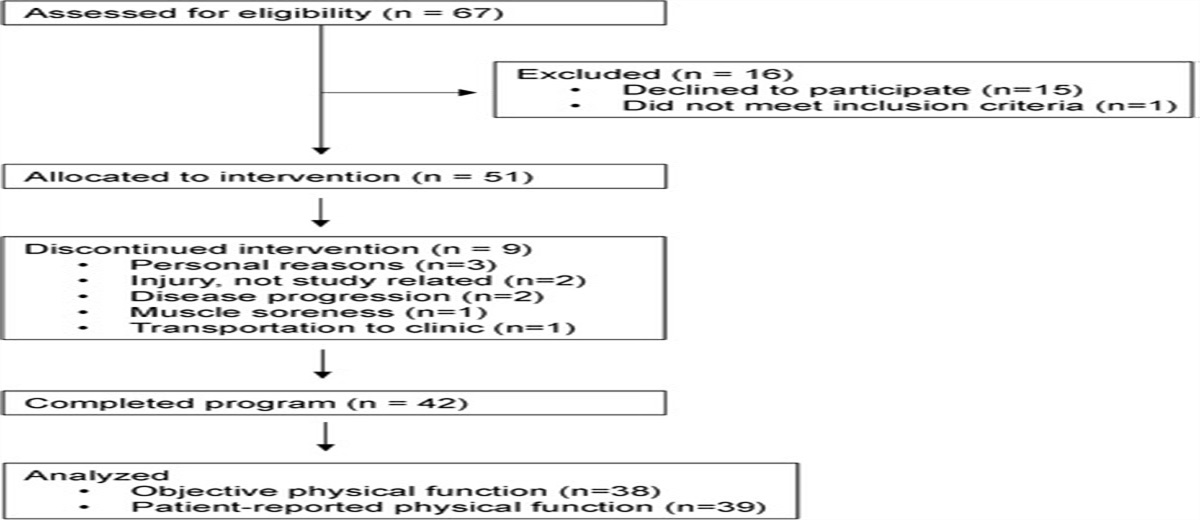
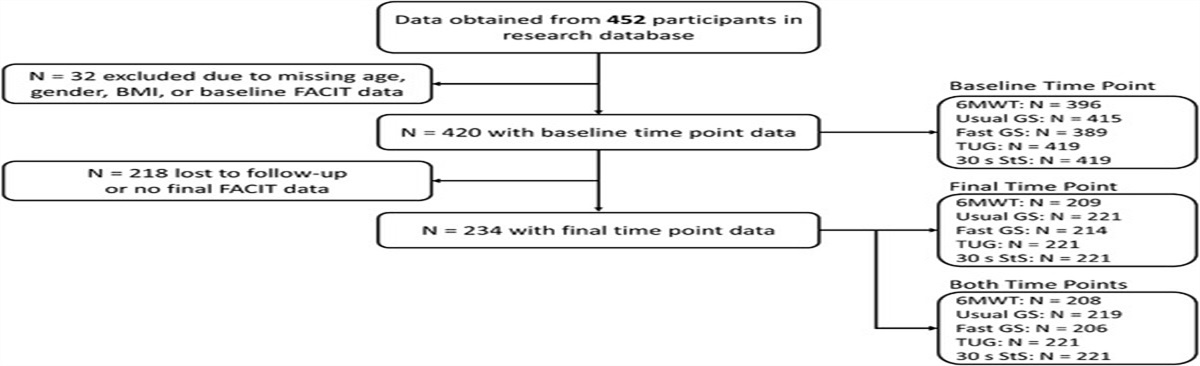
RESULTS Study SelectionAfter a comprehensive literature search, ta total of 201 studies met the inclusion criteria (Figure). After title/abstract screening, 27 studies were assessed by full-text reading. Five articles were included in the final systematic review (Figure).
 Fig.:
Fig.: A flowchart of search strategy.
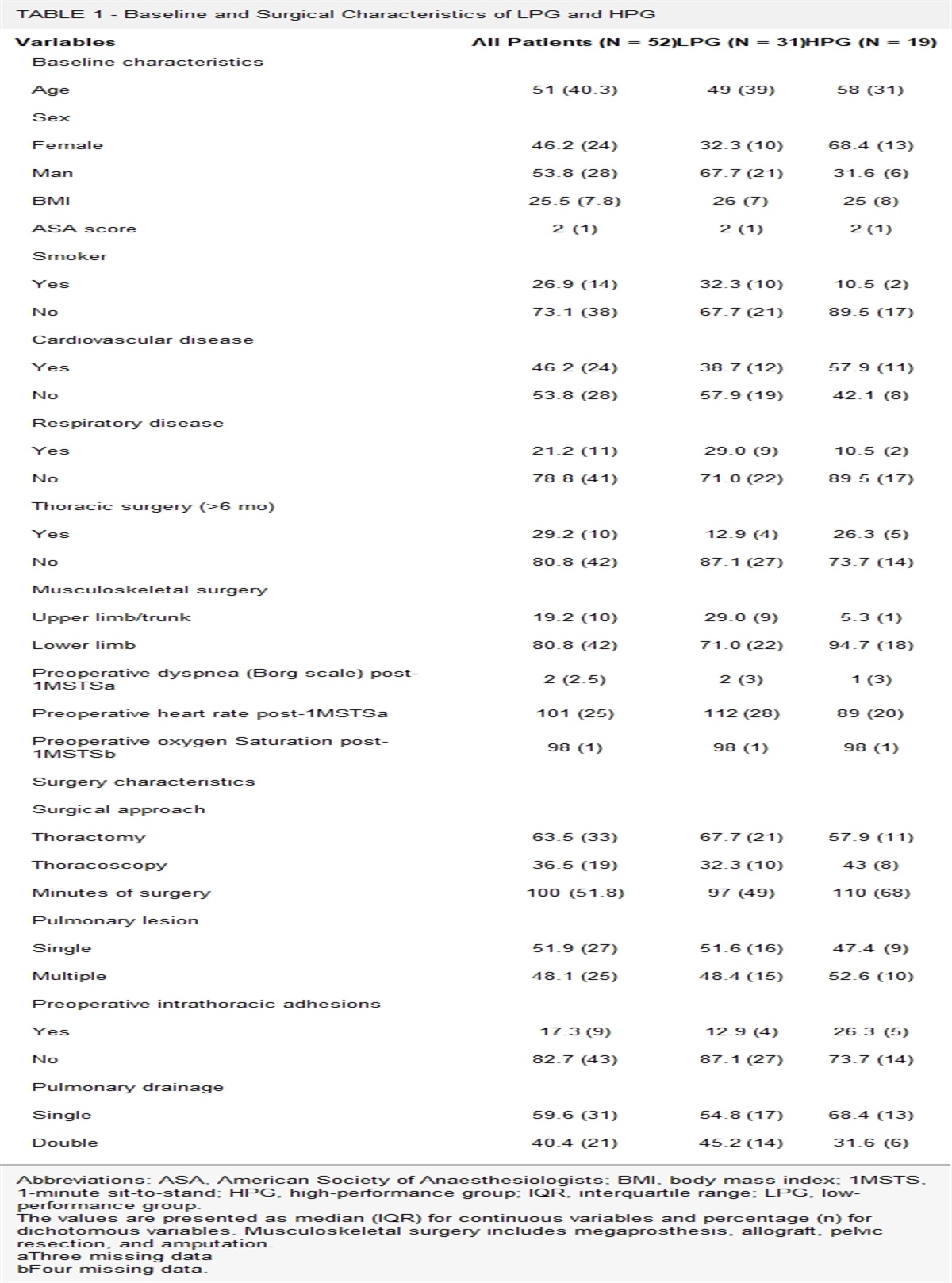
Study Description and QualityThe 5 RCTs included 276 patients with a confirmed diagnosis of LC. All patients underwent surgery. The types of surgery included open surgery (134 participants) and video-assisted thoracic surgery (VATS) (142 participants). There was a dropout of 27 participants in 3 studies; thus, 249 participants were analyzed after training. One study included only PWLC with VATS,25 and others combined both types of surgery with no significant difference in the open-VATS surgery ratio between the control (CG) and intervention groups (IG).26–29 The median age of participants was 64.2 (70.5; 53.3) years. BMI was in the normal or overweight range.30 The smoking rate was above 60% in 4 studies reporting this rate.27 There was no significant difference in demographic characteristics between the IG and the CG in all studies (P > .05) (Table 1).
TABLE 1 - Characteristics of Studies Author Design Sample Size Mean Age, y Gender (Female/Male) BMI Smoking Rate Pre-op MIP, cmH2O Surgery PEDro Score VATS Thoracotomy Brocki et al26 IG: IMT + rehab 34 69.7 ± 7.9 14/20 25.4 ± 4.3 33/34 82.8 ± 26.8 59% 41% 8 CG: rehab 34 70.5 ± 7.5 15/19 28.0 ± 5.7 30/34 78.5 ± 29.5 44% 56% Brocki et al27 IG: IMT + rehab 34 70 ± 8 14/20 26 ± 4 ... 83 ± 27 59% 41% 7 CG: rehab 32 70 ± 8 13/19 28 ± 6 ... 78 ± 29 44% 56% Messaggi-Sartor et al28 IG: IEMT + aerobic 16 64.2 ± 8.1 8/8 28.1 ± 4.6 13/16 69.4 ± 25.0 12.5% 87.5% 6 CG: health advice 21 64.6 ± 8.9 3/18 26.8 ± 3.1 20/21 75.4 ± 30.4 4.8% 95.2% Taşkin et al29 IG: IMT + CT + early mobilization 20 53.3 ± 10.4 5/15 26.5 ± 4.0 17/20 65.1 ± 15.5 15% 85% 7 CG: CT + early mobilization 20 57.1 ± 8.7 7/13 28.4 ± 6.1 13/20 59.2 ± 13.7 15% 85% Liu et al25 IG: IMT + aerobic + rehab 28 66.3 ± 7.9 18/10 73% > 23 18/28 53.5 ± 15.6 100% 7 CG: rehab 26 64.2 ± 5.9 14/12 57% > 23 23/26 49.4 ± 15.1 100%Abbreviations: BMI, body mass index; CG, control group; CT, chest therapy; IEMT, inspiratory-expiratory muscle training; IG, intervention group; IMT, inspiratory muscle training; pre-op MIP, preoperative maximal inspiratory pressure; rehab, rehabilitation program; VATS, video-assisted thoracoscopic surgery.
The median PEDro score was 7. All the scores were between 8 and 6.
Intervention DescriptionAll the patients from the IG received P-IMT combined with a rehabilitation program. Rehabilitation programs were composed of aerobic training, breathing exercise, positive expiratory pressure (PEP), early mobilization, airway clearance techniques, strength limb exercise, PA advice, and respiratory muscle training. The duration of training was from 2 to 8 weeks.26–28 In 1 study, the training program was finished when patients were discharged without a fixed duration.29 One study started the training 4 days after surgery, and it continued until 6 weeks after discharge.25 Three studies started the training 1 to 2 days after surgery without mentioning the tube removal,26,27,29 and 1 study started at 4 to 6 weeks post-surgery.28
The CGs received the same rehabilitation program in 3 studies.25–27,29 One CG received only PA advice. Two studies used Powerbreath, 2 others used Threshold, and 1 study combined inspiratory and expiratory muscle training with Oxygen Dual Valve. The intensity of P-IMT varied from 15% to 50% of the MIP and the training frequency ranged from 100 to 120 repetitions a day and 3 to 5 days a week (Table 2).
TABLE 2 - Characteristics of Interventions and Results Author Sample Size Intervention Program Time (Beginning and Duration) IMT Program Outcome Findings Intensity Frequency Device Brocki et al26 IG: 34 IMT + rehab: mobilization, deep breathing, PEP, cough After surgery, 2 wk 15% MIP, increase 2 cmH2O/d 30 × 2Hypoxemia: IG (5/34) vs CG (12/34), P = .049
Pneumonia: same presentation than for hypoxemia, P = .14
Atelectasis: idem, P = .11
CG: 34 Rehab: mobilization, deep breathing, PEP, cough After surgery, 2 wk ... ... ... 6MWT:IG: D = −48.1 ± 71.9 m, P < .001
CG: D = − 31.7 ± 79.1 m, P > .05
D = −16.4 m, 95% CI, −52.4 to 21.3, P = .21
MIP:IG: MD = 0.21 ± 17.9 cmH2O, P > .05
CG: MD = −4.92 ± 15.1 cmH2O, P > .05
D = 4.5 cmH2O (95% CI, −3.85 to 12.85), P = .22
MEP:IG: MD = −4.7 ± 16.3 cmH2O, P > .05
CG: MD = −0.5 ± 16.2 cmH2O, P > .05
D = −4.12 cmH2O (95% CI, −12.27 to 4.04), P = .26
Spirometry:FVC (% pred): no difference, P = .57
FEV1 (% pred): idem, P = .14
Brocki et al27 IG: 34 IMT + rehab: mobilization, positive expiration pressure, cough. After surgery, 2 wk 15% MIP, increase 2 cmH2O/d 30 × 2, Twice a day, continued for 2 wk Powerbreath QoL: IG vs CG: P = .8Sedentary: IG (6%) vs CG (22%), P = .006
Low activity: IG (56%) vs CG (66%), P = .006
Moderate activity: IG (38%) vs CG (12%), P = .006
CG: 32/34 Rehab: mobilization, positive expiration pressure, cough After surgery, 2 wk ... ... ... Messaggi-Sartor et al28 IG: 11/16 IEMT + aerobic 4-6 wk post-surgery, 8 wk 50% MIP/MEP, increase 10 cmH2O/wk 10 × 5IG (% pred): Pre (68.5 ± 27.5) – post (83 ± 21.2)
CG (% pred): pre (71.6 ± 32.9) – post (70 ± 29.1)
MD between 2 groups = 13.42 cmH2O (95% CI, 2.7 to 24.1), P = .015
MEP:IG (% pred): pre (64.5 ± 19.5) – post (78.4 ± 17.8)
CG (% pred): pre (62.2 ± 21.6) – post (68.8 ± 20.1)
MD between 2 groups = 18.58 cmH2O (95% CI, 4.0 to 33.1), P = .023
QoL: improve EORTC QoL-C30 score after intervention, but no significant difference between IG and CG (P > .05) Taşkin et al29 IG: 20 CT + early mobilization + IMT 1-2 d after surgery, around 2 wk 15% MIP, increase 2 cmH2O/d up to 45% 10 × 6IG: MD = −29.5 ± 122.3 m, P > .05
CG: MD = − 115.2 ± 128.9 m, P < .01
D = 85.72 m (95% CI, 166.15 to 5.28), P = .037
CG: 20 CT + early mobilization 1-2 d after surgery, around 2 wk ... ... ... MIP:IG: MD = 3.1 ± 17.3 cmH2O, P > .05
CG: MD = − 8 ± 16.4 cmH2O, P > .05
D = 11.05 (95% CI, 21.84 to 0.25), P = .045
MEP:IG: MD = 1.1 ± 17.7 cmH2O, P > .05
CG: MD = −24.1 ± 34.6 cmH2O, P < .01
D = 25.23 (95% CI, 42.83 to 7.62), P = .006
Hospital stays: IG (9.1 ± 3) vs CG (12.9 ± 4.2), P = .002 Liu et al25 IG: 26/32 Aerobic + IMT + rehab (breathing control, limbs exercises, airway clearance technique, incentive spirometry, lung expansion) 4 d after surgery, 6 wk 30% MIP, increase to 45%MIP 10-15Pneumonia: idem, P = .165
Atelectasis: idem, P = .295
ARDS: idem, P = .519
CG: 28/31 Rehab (breathing control, limbs exercises, airway clearance technique, incentive spirometry, lung expansion) 4 d after surgery, 6 wk ... ... ...Respiratory failure: idem, P = .519
Subcutaneous emphysema: idem, P = .893
Air leak: idem, P = .177
6MWT at wk 2:6MWT at wk 6:6MWT at wk 12:MIP at wk 2:MIP at wk 6:MIP at wk 12:MEP at wk 2:MEP at wk 6:MEP at wk 12:Abbreviations: ARDS, acute respiratory distress syndrome; CG, control group; CT, chest therapy; FEV1, first second of forced expiration; FVC, forced vital capacity; IEMT, inspiratory-expiratory muscle training; IG, intervention group; IMT, inspiratory muscle training; MD, mean difference; MEP, maximal expiratory pressure; MIP, maximal inspiratory pressure; PA, physical activity; PEP, positive expiratory pressure; PPC, postoperative pulmonary complication; QoL, quality of life; rehab, rehabilitation program; 6MWT, 6-minute walking test; WHO, World Health Organization.
PPCs were assessed in 2 studies. Only one study reported a significantly lower rate of hypoxemia in the IG than in the CG (15% vs 35%, P = .049), but no difference in pneumonia (P = .14) or atelectasis (P = .11) between the 2 groups without associating with the type of surgery.26 Another study reported the same result of PPCs in the 2 groups with VATS.25
Physical CapacityThree studies assessed the 6MWT.25,26,29 Only 2 of them demonstrated a significant difference in the walked distance between the 2 groups. One of them showed a significant difference after 2, 6, and 12 weeks.25 The other reported a significant decrease in the 6MWT in the CG while there was no significant change in the IG, and the difference between the 2 groups was significant.29
One study assessed Vo2peak and the authors reported a significant improvement in the IG than in the CG.28
Maximal Inspiratory Pressure and Maximal Expiratory PressureMIP was assessed in 4 studies as the outcome measure. Three studies showed a significant difference in MIP between the 2 groups. One reported a significant difference at 6 months after surgery,29 and 1 after 10 to 12 weeks since the end of the intervention.28 One of them reported a significant difference at week 6, but not at weeks 2 and 12.25 Another study demonstrated no significant difference between the IG and the CG (P = .22).26
Three of the 4 studies that investigated MEP demonstrated a significant difference in MEP between the 2 groups,28,29 but one of them only reported a significant difference at weeks 2 and 12, but without difference at week 6.25
Quality of LifeTwo studies that assess QoL reported no significant difference between IGs and CGs. One study used the EQ-5D-5L (P = .8).27 The other assessed the European Organization for Research and Treatment of Cancer Quality of Life (EORTC QL-30) (P > .05).28
Physical Activity LevelOne study assessed PA by using the Physical Activity Scale 2.1 reported less sedentary and more moderate activity levels in the IG than in the CG (P = .006).27 Another study assessed the Physical Functioning Scale with the EORTC QL-30 finding no significant difference between the 2 groups (P > .05).28
Hospital Length of StayOnly one study assessed the hospital length of stay as an outcome. It was shorter in the IG (9.1 ± 3 days) than in the CG (12.9 ± 4.2 days) (P = .002).29
SpirometryOnly one study assessed the effect of P-IMT on lung function without a significant difference between the IG and the CG.26
DISCUSSIONThis systematic review focused on the effect of P-IMT after surgery in PWLC. There was insufficient evidence to promote the use of P-IMT. Included studies were heterogeneous in terms of intervention programs, which made it challenging to analyze the results. Due to the few studies, the findings should be cautiously interpreted.
The effect of P-IMT on PPCs was difficult to analyze because of the methodology of the studies. According to the result, the earlier starting point with a higher %MIP did not show more benefit in PPCs compared with the 4-day delayed lower-intensity P-IMT. The longer duration of the 6-week P-IMT did not show any benefit on PPCs compared with the 2-week program. However, due to the natural recovery process of the operative lung being 6 weeks, the assessment conducted earlier than 6 weeks after surgery may not be good for evaluating the effect of P-IMT in PPCs.31 In addition, the high rate of smoking and high BMI in these studies, which also increases the risk of PPCs,32 should be considered while interpreting the result. The benefit of P-IMT on PPCs with different surgery types was not found. However, with the same percentage of subcutaneous emphysema and air leak in both groups, P-IMT did not increase these risks, contributing to the feasibility of P-IMT in postoperative PWLC. Therefore, P-IMT can be used to improve diaphragm function after surgery.33–36 More studies are needed to clarify this point as well as the ideal characteristics of the program.
Studies in this systematic review showed that the short-term effect of P-IMT on the 6MWT was unclear. Noticeably, 2 studies, which showed a benefit in the 6MWT,25,28 added aerobic exercise in the IG but not in the CG; therefore, aerobic exercise can be the reason for the improvement of the 6MWT.37–39 In addition, it was impossible to recommend when to start P-IMT due to different starting points in included studies. The result of this review did not suggest any ideal setting of P-IMT for the improvement of the 6MWT. Despite the similar duration, intensity, and frequency of P-IMT in 2 studies, only 1 of them reported a significant difference in the 6MWT between the 2 groups.26,29 Due to this discrepancy, concluding the short-term effect of P-IMT on the 6MWT was challenging. The ideal intensity and frequency of P-IMT for the short-term 6MWT could not be determined. With only 1 study, it was difficult to assess the effect of P-IMT on Vo2peak. Like the 6MWT, the improvement of Vo2peak may be induced by aerobic exercise applied in the IG but not in the CG.37–39 The same caution should be applied while interpreting the effect of mid-to-long-term P-IMT on physical capacity. More studies with longer follow-ups are needed to understand the specific role as well as the ideal characteristics of P-IMT on physical capacity.
As noted earlier, understanding the effect of P-IMT on inspiratory muscles is important because of the negative correlation previously observed between MIP and PPCs.40 With similar intensity and frequency, the short-term effect of P-IMT on MIP was contradictory. Two studies reported a significant short-term reduction in postoperative MIP prior to recovering to the preoperative state without significant difference between the 2 groups.26,29 Thus, the decline may be due to inspiratory muscle dysfunction caused by postoperative pain in the early days.41 And the recovery of MIP can be a natural process after 2 weeks of surgery.42 There was insufficient evidence to suggest that P-IMT had different efficacy in patients with different surgical procedures. More studies are needed to understand the effect of P-IMT on MIP.
According to our results, mid-to-long-term effects of P-IMT on MIP were weak. Two studies showed a significant difference in MIP between the IG and the CG with 6- to 8-week training.25,28 However, both studies included aerobic exercise in the IG but not in the CG; thus, the improvement of aerobic-induced general health can be the reason for the enhancement of MIP.43 Noticeably, the significant difference in MIP between the 2 groups disappeared after 12 weeks post-surgery.25 Thus, retaining training may be a good recommendation to maintain MIP, especially in elderly people.44
For MEP, the evidence was conflicted. Two out of the 3 studies showed short-term benefits of MEP.25,29 As no changes were observed in the IG contrarily to the CG, it has been suggested that P-IMT can maintain or promote the recovery of MEP.29 However, this study applied PEP for CGs and IGs. Although PEP cannot be exactly defined as expiratory muscle training, it has to be considered while interpreting the results.45 Another study reported a significant reduction in MEP after surgery but recovered to presurgery status after 2 weeks in both groups without a significant difference between the 2 groups.26 Thus, recovery may be the natural process after surgery.42 Although there was some supportive evidence, it was challenging to define the effect of P-IMT on short-term MEP.
The improvement of the long-term MEP was observed.25,28 However, the effect should be cautiously interpreted since aerobic exercises, which were applied in IGs but not in CGs, may be the reason for the improvement.37 Besides, the MEP reevaluation time of these studies was less than 12 weeks, which was believed to be not long enough to reverse the strength induced by resistance training.46–49
Due to the importance of the change in QoL, PA level, hospital length of stay, and spirometry in the LC population, investigating the effects of P-IMT in these aspects was worthy.50–53 However, with only 1 study assessing each of the outcomes stated above, it was challenging to reach a conclusion. In addition, the time of the QoL assessment in included studies was too early to catch the true score. Indeed, QoL was usually assessed 6 months after surgery.7,54 Our result reported a higher PA level with P-IMT.27 The reason can be the improvement of the whole-body exercise capacity contributed by inspiratory muscle strengthening, which facilitates PA levels.55 One study reported a shorter hospital length of stay with early IMT.29 The earlier discharge was only observed in the IG despite early mobilization, which was believed to reduce the hospital length of stay, was applied in both groups.56,57 Therefore, P-IMT can promote the earlier discharge after LC surgery. No effect of P-IMT on spirometry tests was found in this systematic review, with only 1 study assessed spirometry. In addition, the test was conducted at week 2 postoperatively, when pain can still impair breathing maneuvers, leading to uncountable results.58
The main limitation of this review was the small number of studies. With only 5 studies included, data extraction and analysis were challenging. Included studies had a heterogeneous population with differences in intensity and training programs. Thus, it made the comparison difficult. The wide range of duration and starting point of intervention was also another limitation. In addition, the inconsistent outcome measurement in the studies also challenged the result interpretation.
ConclusionOverall, this systematic review reported conflicting results of P-IMT in PWLC with surgery. No effect of P-IMT in PPCs was reported. The effect of P-IMT on physical capacity and respiratory muscle strength was not observed. P-IMT can be used as an additional therapy to improve hospital length of stay and postoperative PA levels with a low level of evidence. In addition, we could not find the optimal setting of P-IMT for PWLC with surgery. Further studies with clear settings of the intervention program and specific outcomes should be conducted to confirm the role of P-IMT on PWLC with surgery.
REFERENCES 1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. 2. Jones GS, Baldwin DR. Recent advances in the management of lung cancer. Clin. Med. 2018;18(suppl 2):s41–s46. 3. American Lung Association. State of Lung Cancer: 2020 Report. https://www.lung.org/getmedia/381ca407-a4e9-4069-b24b-195811f29a00/solc2020-report-final.pdf. Published 2021. Accessed January 19, 2022. 4. Howlader N, Forjaz G, Mooradian MJ, et al. The effect of advances in lung-cancer treatment on population mortality. N Engl J Med. 2020;383(7):640–649. 5. Rueth NM, Parsons HM, Habermann EB, et al. The long-term impact of surgical complications after resection of stage I nonsmall cell lung cancer: a population-based survival analysis. Ann Surg. 2011;254(2):368–374. 6. Detillon DD, Veen EJ. Postoperative outcome after pulmonary surgery for non-small cell lung cancer in elderly patients. Ann Thorac Surg. 2018;105(1):287–293. 7. Poghosyan H, Sheldon LK, Leveille SG, Cooley ME. Health-related quality of life after surgical treatment in patients with non-small cell lung cancer: a systematic review. Lung Cancer. 2013;81(1):11–26. 8. Jones LW, Hornsby WE, Goetzinger A, et al. Prognostic significance of functional capacity and exercise behavior in patients with metastatic non-small cell lung cancer. Lung Cancer. 2012;76(2):248–252. 9. Jones LW, Watson D, Herndon JE, et al. Peak oxygen consumption and long-term all-cause mortality in nonsmall cell lung cancer. Cancer. 2010;116(20):4825–4832. 10. Varela G, Novoa NM, Agostini P, Ballesteros E. Chest physiotherapy in lung resection patients: state of the art. Semin Thorac Cardiovasc Surg. 2011;23(4):297–306. 11. Varela G, Jiménez MF, Novoa N, Aranda JL. Estimating hospital costs attributable to prolonged air leak in pulmonary lobectomy. Eur J Cardiothorac Surg. 2005;27(2):329–333. 12. Mans CM, Reeve JC, Elkins MR. Postoperative outcomes following preoperative inspiratory muscle training in patients undergoing cardiothoracic or upper abdominal surgery: a systematic review and meta-analysis. Clin Rehabil. 2015;29(5):426–438. 13. Greising SM, Ottenheijm CA, O'Halloran KD, Barreiro E. Diaphragm plasticity in aging and disease: therapies for muscle weakness go from strength to strength. J Appl Physiol. 2018;125(2):243–253. 14. Ohara DG, Pegorari M, Oliveira Dos Santos N, et al. Respiratory muscle strength as a discriminator of sarcopenia in community-dwelling elderly: a cross-sectional study. J Nutr Health Aging. 2018;22(8):952–958. 15. Buchman A, Boyle P, Wilson R, Leurgans S, Shah R, Bennett D. Respiratory muscle strength predicts decline in mobility in older persons. Neuroepidemiology. 2008;31(3):174–180. 16. Wijdicks EF. The neurology of acutely failing respiratory mechanics. Ann Neurol. 2017;81(4):485–494. 17. Wang YQ, Liu X, Jia Y, Xie J. Impact of breathing exercises in subjects with lung cancer undergoing surgical resection: a systematic review and meta-analysis. J Clin Nurs. 2019;28(5-6):717–732. 18. Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disabil Rehabil. 2018;40(8):864–882. 19. Rosero ID, Ramírez-Vélez R, Lucia A, et al. Systematic review and meta-analysis of randomized, controlled trials on preoperative physical exercise interventions in patients with non-small-cell lung cancer. Cancers (Basel). 2019;11(7):944.
Comments (0)