
Remember me




Lung metastasis occurs in 30% to 44% of patients with bone tumors, making the lungs the most common site of metastasis for this type of tumor.1-3 These patients have typically already undergone surgical resection and reconstruction of the musculoskeletal system with significant functional limitations. Limb salvage surgery with mega-prostheses or allograft reconstructions of the femur, tibia, and humerus are common operations in this field. The elective treatment of lung metastases is ablative surgery, and the wedge resection technique is also used in the event of repeated recurrences over time.1,3 Lung wedge resection surgery does not follow the anatomical limits of the lung but is customized according to the metastatic area to be removed in combination with a reasonable amount of healthy tissue (margin). The aim of this technique is to limit the sacrifice of lung tissue, with a lower impact on function and preserving residual lung volume postoperatively.4 In the postoperative phase, physiotherapy treatment can play an important role in preventing postsurgical respiratory complications, managing painful symptoms, and, above all, facilitating the recovery of physical performance.5-7 Breathing exercises (the active cycle of breathing techniques), early mobilization exercises, and the use of volume incentives are recommended from the first postoperative day, with very uniform recovery assessment methods.6,8-11 The 1-minute sit-to-stand (1MSTS) is a test used precisely for assessing the physical performance of different types of patients, such as patients with lung, heart, or kidney diseases, or those receiving palliative care.12-15 Data on early recovery of patients after wedge resection treatment are limited in the literature, particularly for the population with bone tumor metastases.
Therefore, the aim of this study is to describe the course of recovery of physical ability for patients undergoing lung wedge resection surgery for bone tumor metastases using the 1MSTS test and highlighting:
The physical performance that can be recovered during hospitalization and the course of that recovery. The feasibility and safety of performing the 1MSTS test during the first 6 days of postoperative hospitalization. The clinical characteristics of patients who are able to achieve a high level of recovery early on compared to patients with a low level of recovery. MATERIALS AND METHODS DesignProspective prognostic observational cohort study.
Setting and PopulationThe study was conducted in a general and thoracic surgery department within an orthopedic department, which is a national and international hub for the treatment of musculoskeletal tumors. All patients undergoing planned ablative thoracic surgery by wedge resection for localized lung metastases from January 2022 to July 2023 were recruited consecutively. The study was approved by the Local Ethics Committee under protocol no. 0018550 and registered at https://clinicaltrials.gov/ with no. NCT05310539. Patients eligible for the study were identified according to the following criteria:
Inclusion criteria: All patients over 12 years of age undergoing planned ablative thoracic surgery of localized lung metastases for primary bone tumor and able to perform the 1MSTS test in the preoperative physiotherapy assessment phases. Exclusion criteria: All patients who had undergone ablative thoracic surgery in the 6 months prior to the time of enrollment or for a nononcological diagnosis. In the case of severe postoperative complications that did not allow the implementation of the physiotherapeutic recovery course, data on such patients were excluded. Treatment PathPatients were admitted for preoperative assessments and examinations the day before surgery. The surgical procedure routinely involved one or more metastasectomies performed by means of lateral thoracotomy access with muscle sparing, or, for selected cases, one or more metastasectomies performed by videothoracoscopy with 3 chest accesses (triportal). Then, 1 or 2 chest drains were inserted, depending on the need to monitor for air and/or blood loss that occurred during surgery. Physiotherapy began on the first postoperative day, with twice daily sessions for 5 days and then once on the sixth day. On the seventh day, they were encouraged to walk independently and perform the respiratory exercises learned during the week at least once during the day. The individual physiotherapy sessions lasted approximately 30 minutes and included breathing exercises such as the active cycle of breathing techniques, exercises to stimulate inspiratory volume, upper limb mobilization exercises on the same thoracic side involved in the surgery, and exercises aimed at recovering autonomy in daily living. Patients were encouraged to gradually recover sitting, standing, and walking from the first day. The physiotherapist recorded the treatment performed, improvements observed, and relevant notes, such as the onset of early fatigue or worsening symptoms of pain, in the physiotherapy journal.
Outcomes MeasuredThe recovery of physical performance was assessed by conducting the 1MSTS test. The test was conducted by asking the patient to stand up from a chair, fully extending the knees, as many times as possible in 1 minute without resting the upper limbs on the chair.16 The test was conducted by the departmental physiotherapist, noting whether the patient was able to perform the test correctly or needed any modifications to the test to make it safe and feasible, such as performing the test with upper limb support. To be able to verify feasibility for the patient, pain levels were recorded before and after performing the 1MSTS test, using the Numeric Rating Scale,17 dyspnea was perceived through the Borg scale,18 and oxygen saturation (SpO2 as a percentage) and heart rate parameters were determined through the use of a pulse oximeter.19 The test was conducted on the preoperative day as a baseline assessment of the patient and once daily from the first postoperative day until the sixth postoperative day, which was identified as the primary outcome of the study. The test was not performed on Sundays, which fell on the fifth postoperative day. To verify the patient’s level of recovery during hospitalization, a comparison was made between the number of repetitions performed in the preoperative test vs the performance on the sixth postoperative day (Diff1MSTS = Reps. D6 − Reps. preop.). This way, patients who were able to reach or improve on the preoperative test results (Diff1MSTS ≥ 0) formed the group of patients with a high level of recovery of physical performance (high-performance group [HPG]), which was compared to the group defined as having a low level of recovery with lower physical performance than preoperatively (Diff1MSTS < 0; low-performance group [LPG]).
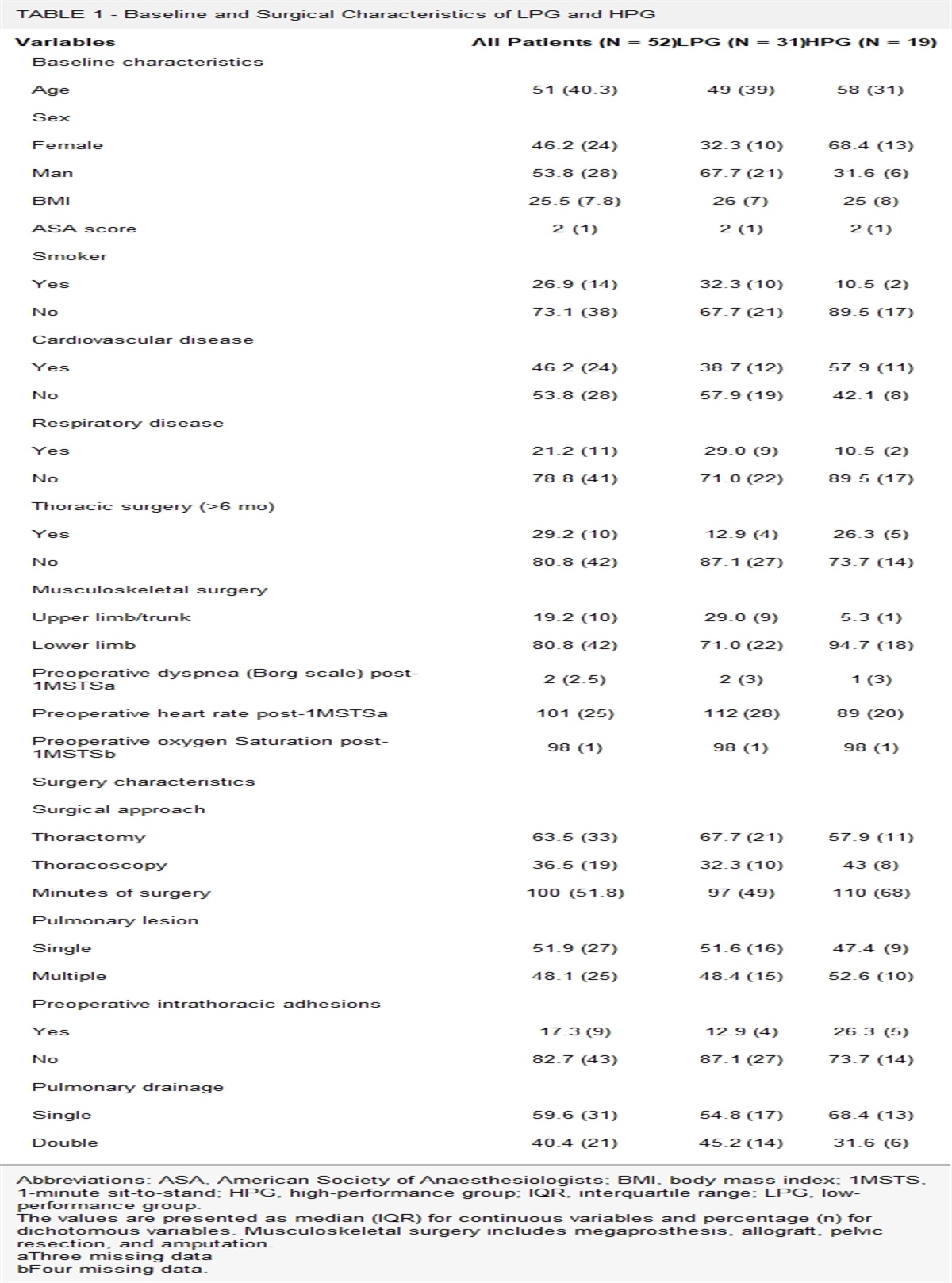
VariablesThrough a literature search20-23 and discussion with professionals (nurses, physiotherapists, oncologists, thoracic surgeons from the various disciplines, etc) involved in managing patients undergoing lung resection, a panel of variables identified as possible risk factors for recovering physical ability in the postoperative period was established. The variables were divided into 2 categories: variables related to patient characteristics and variables related to the surgical procedure, and they are summarized in Table 1. These data were collected by interviewing the patient and consulting the medical records.
TABLE 1 - Baseline and Surgical Characteristics of LPG and HPG Variables All Patients (N = 52) LPG (N = 31) HPG (N = 19) Baseline characteristics Age 51 (40.3) 49 (39) 58 (31) Sex Female 46.2 (24) 32.3 (10) 68.4 (13) Man 53.8 (28) 67.7 (21) 31.6 (6) BMI 25.5 (7.8) 26 (7) 25 (8) ASA score 2 (1) 2 (1) 2 (1) Smoker Yes 26.9 (14) 32.3 (10) 10.5 (2) No 73.1 (38) 67.7 (21) 89.5 (17) Cardiovascular disease Yes 46.2 (24) 38.7 (12) 57.9 (11) No 53.8 (28) 57.9 (19) 42.1 (8) Respiratory disease Yes 21.2 (11) 29.0 (9) 10.5 (2) No 78.8 (41) 71.0 (22) 89.5 (17) Thoracic surgery (>6 mo) Yes 29.2 (10) 12.9 (4) 26.3 (5) No 80.8 (42) 87.1 (27) 73.7 (14) Musculoskeletal surgery Upper limb/trunk 19.2 (10) 29.0 (9) 5.3 (1) Lower limb 80.8 (42) 71.0 (22) 94.7 (18) Preoperative dyspnea (Borg scale) post-1MSTSa 2 (2.5) 2 (3) 1 (3) Preoperative heart rate post-1MSTSa 101 (25) 112 (28) 89 (20) Preoperative oxygen Saturation post-1MSTSb 98 (1) 98 (1) 98 (1) Surgery characteristics Surgical approach Thoractomy 63.5 (33) 67.7 (21) 57.9 (11) Thoracoscopy 36.5 (19) 32.3 (10) 43 (8) Minutes of surgery 100 (51.8) 97 (49) 110 (68) Pulmonary lesion Single 51.9 (27) 51.6 (16) 47.4 (9) Multiple 48.1 (25) 48.4 (15) 52.6 (10) Preoperative intrathoracic adhesions Yes 17.3 (9) 12.9 (4) 26.3 (5) No 82.7 (43) 87.1 (27) 73.7 (14) Pulmonary drainage Single 59.6 (31) 54.8 (17) 68.4 (13) Double 40.4 (21) 45.2 (14) 31.6 (6)Abbreviations: ASA, American Society of Anaesthesiologists; BMI, body mass index; 1MSTS, 1-minute sit-to-stand; HPG, high-performance group; IQR, interquartile range; LPG, low-performance group.
The values are presented as median (IQR) for continuous variables and percentage (n) for dichotomous variables. Musculoskeletal surgery includes megaprosthesis, allograft, pelvic resection, and amputation.
aThree missing data
bFour missing data.
Numerical variables were described using median values and interquartile range, while dichotomous variables were described as frequency and percentage. The collected variables were returned in summary form by comparing the HPG to the LPG. The relationship between these groups and the variables under consideration was analyzed using a logistic regression model, and the independent factors were selected by applying a backward procedure, first limiting any confounding variables in the model and then adjusting the effects for all the factors analyzed.
Sample SizeGiven the rarity of the oncological pathology of the musculoskeletal system, incidence of less than 1%,24 and the related cases of pulmonary metastases, a convenience sample of at least 50 patients was recruited. Data were collected from all patients treated consecutively during the study period, according to the defined inclusion criteria.
RESULTSA total of 65 patients underwent thoracic surgery during the study period. Of these, 3 patients were excluded: in 2 cases, because a major operation had been performed in conjunction with wedge surgery—in one case, vertebrectomy, and, in the other, removal of a knee spacer due to infection—and, in 1 case, due to wedge surgery with a nononcological diagnosis. For 7 patients, multiple interventions were involved, so only data from their first admission were considered in this analysis. Of the 55 eligible patients, it was possible to enroll 52. The median age was 51 years (interquartile range [IQR] 40.3), and women made up 44.2% of the sample. The basic characteristics of the sample are summarized in Table 1.
The 1MSTS test on the sixth day was conducted in all patients with a median number of repetitions of 17.5, with a value comparable to the preoperative median. During hospitalization, there was evidence of progressive improvement in physical performance with an increase in the median number of repetitions and the number of patients able to perform the test (Table 2). To make it safe to perform the test for 7 patients (13.5%), the test was allowed to be performed with upper limb support and, in one case, with the use of forearm support. The Borg scale, measured after the test, showed a median of 3 (IQR 1.8) for moderate dyspnea, and only 6 patients (11.5%) showed Borg scale values above 4. The median heart rate was 105 (IQR 32.5). Assessing the maximum heart rate of individual patients using Cooper’s formula, all patients had a heart rate after exertion in the range of 50% to 85% of the maximum rate. The median of the percentage of oxygen saturation dropped by 1 point after the test was performed, and the median of pre- and posttest symptoms of pain was almost equivalent from as early as the third postoperative day.
TABLE 2 - Evolution of 1MSTS Performance from Pre- to Postsurgery Presurgery Postsurgery 1st day 2nd day 3rd day 4th day 6th day 1MSTS test No. of repetitions 177 7 (8.5) 128 14 (7.8) 15.58 17.56 Percentage of patients evaluated 96.2 (50) 28.815 63.5 (33) 76.9 (40) 76.9 (40) 100 (52) Pain (NRS) Pretest 0 (0) 2 (2.3) 21 22 2 (1.3) 1.51 Posttest 0 (0) 41 32 21 2 (1.5) 22 Dyspnea (Borg Scale) Pretest 0 (0) 2 (2.1) 2 (2.5) 1 (1.8) 12 0.51 Posttest 0 (0) 21 3 (1.8) 3 (2.3) 32 3 (1.8) Heart rate Pretest 84 (30) 84.5 (22.8) 80 (18.8) 8521 8320 8624 Posttest 106 (32) 95 (19.8) 100 (20.5) 99.5 (28.5) 102 (27.3) 105 (32.5) Oxygen saturation Pretest 981 96.5 (4.5) 963 963 972 982 Posttest 981 963 954 96.5 (4.3) 973 97 (3.8)Abbreviation: 1MSTS, 1-minute sit-to-stand; NRS, Numeric Rating Scale.
The values are presented as median (IQR) for continuous variables.
Table 1 summarizes the comparison of baseline characteristics and surgical variables between the LPG with 31 patients (62%) and the HPG with 19 patients (38%). In this analysis, 2 patients were excluded because they had not performed the 1MSTS test preoperatively due to organizational reasons. The logistic regression (Table 3) conducted for early recovered physical performance showed female gender as a protective factor. Previous respiratory comorbidities and previous surgery to the upper limbs/trunk were risk factors. After the 1MSTS test was performed preoperatively, a higher heart rate and lower oxygen saturation rate were themselves predictors of a worse postoperative outcome.
TABLE 3 - Multivariate Analysis for the High Performance at 6 Days After Surgery Variables OR 95% CI for OR P Value Lower Limit Upper Limit Female 22.719 1.679 307.422 0.019 No respiratory disease 26.159 1.061 645.186 0.046 Lower limb musculoskeletal surgery 0.033 0.002 0.722 0.03 1MSTS presurgery assessment Heart rate posttest 0.859 0.771 0.957 0.006 Oxygen saturation posttest 3.709 0.998 13.787 0.05Abbreviation: 1MSTS, 1-minute sit-to-stand.
Patients undergoing wedge resection surgery for ablation of metastases secondary to bone tumor are able to achieve significant recovery of physical performance from the first few postoperative days, with a significant increase as early as the sixth day. The performance of the 1MSTS test showed that the median number of repetitions recorded on the first day could be doubled by as early as the third postoperative day and similarly, on the second postoperative day, more than 60% of patients were already able to perform the test. To make it easier to perform the test safely, it was also deemed acceptable to perform the test with the arms resting on the chair. This situation occurred in a very small number of patients (13.5%), and it was deemed that this measure would not affect the validity of the data and the test. It should be borne in mind that all patients enrolled had already received surgery with massive reconstruction of the musculoskeletal system as for megaprosthesis and bone allograft, and this condition was the reason for the need for this measure. A total of 38% of patients were able to recover their preoperative level within the first 6 days, and the reported data can help to build a reference standard for this type of patient. Leeden et al10 reported a lower number of repetitions in the 1MSTS of 9.4 (SD = 3.7) for oncological lung surgery patients at the time of discharge on the eighth day, with an average reduction of 3.4 repetitions compared to baseline values.
For patients with bone tumor, the 1MSTS proved to be safe and feasible. The exertion required in terms of saturation, heart rate, symptoms of pain, and dyspnea was attributable to a well-tolerated profile of exertion for the patient. In one case only, the test on the sixth day had to be interrupted before the minute mark due to patient fatigue.
The number of possible repetitions of the 1MSTS preoperatively was equal to 17 (IQR = 7) and was lower than the reference values for a healthy population aged 50 to 54 years reported by Strassman et al29 with a median of 42 repetitions (IQR 35-53), as well as the values reported by Boujibar et al23 for a population awaiting major lung resection surgery due to tumor with a median of 23 repetitions (IQR 18-27). It is worth noting that the data presented by Boujibar et al23 also showed that, after performing the 1MSTS, respiratory parameters were more impaired than those in this study, with mean dyspnea of 4.9 on the Borg scale and an average of oxygen saturation rate of 96. It can be hypothesized that pulmonary lesions related to metastases secondary to bone tumor have less impact on respiratory parameters like dyspnea and oxygen saturation, while at the same time, these patients suffer more from the musculoskeletal surgery they have already undergone, which results in lower physical performance.
The evaluation of the recovery of physical abilities in relation to preoperative abilities made it possible to distinguish between the HPG and LPG. The search for relevant independent prognostic factors made it possible to discover certain basic characteristics of patients that must be taken into account from the preoperative phase when planning the course of care and physiotherapeutic treatment. Among the patients’ nonmodifiable characteristics, female gender was found to be a protective factor, while the presence of respiratory comorbidities and having previous upper limb or trunk surgery due to an oncological pathology were risk factors. The latter may be explained by considering the important role of pushing and balancing that the arms play during the movement of getting up from a chair, thus having a greater impact on the performance of the 1MSTS test.
Preoperatively, the recording of parameters after the 1MSTS test showed that an increased heart rate and lower oxygen saturation may be risk factors for a postoperative LP. Aerobic training aimed at improving physical abilities in the preoperative phase could be a useful tool to enable the patient to be in an optimal condition at the time of wedge resection surgery and thus facilitate the recovery of physical abilities.25-28
To the authors’ knowledge, there are no studies in the literature investigating the recovery of physical abilities of patients undergoing wedge resection. The results of this study may form the basis for further studies in this field with a special focus on bone tumor patients who are shown to have particular needs in order to understand the beneficial effects of a preoperative aerobic exercise program.
LimitationThe study has some limitations. The rarity of the disease does not allow for large sample sizes, so the results of the regression analysis must be evaluated with caution. Second, longer follow-up is necessary to better understand the recovery of physical abilities over time and verify whether a low level of performance recorded early on may be associated with a worse recovery in the medium and long term.
CONCLUSIONRecovery of physical ability after wedge resection surgery for patients with metastases secondary to bone tumor should be encouraged from the early postoperative phases and can be monitored through the use of the 1MSTS test during hospitalization. Aerobic training exercises in the preoperative phase may be useful to improve preoperative performance and early recovery.
STUDY DETAILS Author Contributions Role Author Conceptualization MC, VP, CG, AA, AR, AC Data curation MC, VP, CG, AA, AR Formal analysis MM Methodology MM, VP, AC, DMD, FD, GC Project administration GC Supervision AC, DMD, FD, GC Writing – original draft MM Writing – review & editing MC, DMD, FD, GCThe study was approved by the Local Ethics Committee under protocol no. 0018550 - CE-AVEC 950/2021 /Oss/IOR and registered at https://clinicaltrials.gov/ with no. NCT05310539.
Funding sourcesNo funding was received for this work.
Data Sharing StatementThe data that support the findings of this study are available on request from the corresponding author.
REFERENCES 1. Vijayamurugan N, Bakhshi S. Review of management issues in relapsed osteosarcoma. Expert Rev Anticancer Ther. 2014;14:151–161. doi:10.1586/14737140.2014.863453. 2. Mialou V, Philip T, Kalifa C, Perol D, Gentet J-C, Marec-Berard P, et al. Metastatic osteosarcoma at diagnosis: prognostic factors and long-term outcome—the French pediatric experience. Cancer. 2005;104:1100–1109. doi:10.1002/cncr.21263. 3. Bacci G, Longhi A, Versari M, Mercuri M, Briccoli A, Picci P. Prognostic factors for osteosarcoma of the extremity treated with neoadjuvant chemotherapy: 15-year experience in 789 patients treated at a single institution. Cancer. 2006;106:1154–1161. doi:10.1002/cncr.21724. 4. Alam NZ. Lung resection in patients with marginal pulmonary function. Thorac Surg Clin. 2014;24:361–369. doi:10.1016/j.thorsurg.2014.07.004. 5. Odor PM, Bampoe S, Gilhooly D, Creagh-Brown B, Moonesinghe SR. Perioperative interventions for prevention of postoperative pulmonary complications: systematic review and meta-analysis. BMJ. 2020;368:m540. doi:10.1136/bmj.m540. 6. Reeve J, Denehy L, Stiller K. The physiotherapy management of patients undergoing thoracic surgery: a survey of current practice in Australia and New Zealand. Physiother Res Int. 2007;12:59–71. doi:10.1002/pri.354. 7. Himbert C, Klossner N, Coletta AM, Barnes CA, Wiskemann J, LaStayo PC, et al. Exercise and lung cancer surgery: a systematic review of randomized-controlled trials. Crit Rev Oncol Hematol. 2020;156:103086. doi:10.1016/j.critrevonc.2020.103086. 8. Malik PRA, Fahim C, Vernon J, Thomas P, Schieman C, Finley CJ, et al. Incentive spirometry after lung resection: a randomized controlled trial. Ann Thorac Surg. 2018;106:340–345. doi:10.1016/j.athoracsur.2018.03.051. 9. Wwl L, Lee TW, Yim APC. Shoulder function after thoracic surgery. Thorac Surg Clin. 2004;14:331–343. doi:10.1016/S1547-4127(04)00021-0. 10. van der Leeden M, Balland C, Geleijn E, Huijsmans RJ, Dekker J, Paul MA, et al. In-hospital mobilization, physical fitness, and physical functioning after lung cancer surgery. Ann Thorac Surg. 2019;107:1639–1646. doi:10.1016/j.athoracsur.2018.12.045. 11. Yang M-X, Wang J, Zhang X, Luo Z-R, P-m Y. Perioperative respiratory muscle training improves respiratory muscle strength and physical activity of patients receiving lung surgery: a meta-analysis. World J Clin Cases. 2022;10:4119–4130. doi:10.12998/wjcc.v10.i13.4119. 12. Bohannon RW, Crouch R. 1-Minute sit-to-stand test: systematic review of procedures, performance, and clinimetric properties. J Cardiopulm Rehabil Prev. 2019;39:2–8. doi:10.1097/HCR.0000000000000336. 13. Vaidya T, de Bisschop C, Beaumont M, Ouksel H, Jean V, Dessables F, et al. Is the 1-minute sit-to-stand test a good tool for the evaluation of the impact of pulmonary rehabilitation? Determination of the minimal important difference in COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2609–2616. doi:10.2147/COPD.S115439. 14. Tanriverdi A, Kahraman BO, Ozpelit E, Savci S. Test-retest reliability and validity of 1-minute sit-to-stand test in patients with chronic heart failure. Heart Lung Circ. 2023;32:518–524. doi:10.1016/j.hlc.2023.01.008. 15. Spence JG, Brincks J, Løkke A, Neustrup L, Østergaard EB. One-minute sit-to-stand test as a quick functional test for people with COPD in general practice. NPJ Prim Care Respir Med. 2023;33:11. doi:10.1038/s41533-023-00335-w. 16. Crook S, Büsching G, Schultz K, Lehbert N, Jelusic D, Keusch S, et al. A multicentre validation of the 1-min sit-to-stand test in patients with COPD. Eur Respir J. 2017;49:1601871. doi:10.1183/13993003.01871-2016. 17. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36:707–714. doi:10.1016/j.ajem.2018.01.008. 18. Wilson RC, Jones PW. A comparison of the visual analogue scale and modified Borg scale for the measurement of dyspnoea during exercise. Clin Sci (Lond). 1989;76:277–282. doi:10.1042/cs0760277. 19. Schnapp LM, Cohen NH. Pulse oximetry. Uses and abuses. Chest. 1990;98:1244–1250. doi:10.1378/chest.98.5.1244. 20. Pagès PB, Serayssol C, Brioude G, Falcoz PE, Brouchet L, Le Pimpec-Barthes F, Thomas PA, Bernard A. Risk factors for survival and recurrence after lung metastasectomy. J Surg Res. 2016;203(2):293–300. doi:10.1016/j.jss.2016.01.028. 21. Stéphan F, Boucheseiche S, Hollande J, Flahault A, Cheffi A, Bazelly B, Bonnet F. Pulmonary complications following lung resection: a comprehensive analysis of incidence and possible risk factors. Chest. 2000;118(5):1263–1270. PMID: 11083673. 10.1378/chest.118.5.1263 22. Moon Y, Choi SY, Moon MH. Prognosis of wide wedge resection in patients with stage IA1 and IA2 lung adenocarcinoma with total tumor size including the lepidic component greater than 2 cm: a single center retrospective study. J Thorac Dis. 2020;12(9):4731–4741. doi:10.21037/jtd-20-1507. 23. Boujibar F, Gillibert A, Bonnevie T, Rinieri P, Montagne F, Selim J, et al. The 6-minute stepper test and the sit-to-stand test predict complications after major pulmonary resection via minimally invasive surgery: a prospective inception cohort study. J Physiother. 2022;68:130–135. doi:10.1016/j.jphys.2022.03.001. 24. Picci P, Manfrini M, Fabbri N, Gambarotti M, Vanel D. Atlas of Musculoskeletal Tumors and Tumorlike Lesions: The Rizzoli Case Archive. Springer Nature; 2014. doi:10.1007/978-3-319-01748-8. 25. Kökez H, Keskin H, Ergin M, Erdoğan A. Is preoperative pulmonary rehabilitation effective in the postoperative period after lung resection? Afr Health Sci. 2023;23(1):646–655. doi:10.4314/ahs.v23i1.69. 26. Granger C, Cavalheri V. Preoperative exercise training for people with non-small cell lung cancer. Cochrane Database Syst Rev. 2022;9(9):CD012020. doi:10.1002/14651858.CD012020.pub3. 27. Finley DJ, Stevens CJ, Emond JA, Batsis JA, Fay KA, Darabos C, Sacks OA, Cook SB, Lyons KD. Potential effectiveness of a surgeon-delivered exercise prescription and an activity tracker on pre-operative exercise adherence and aerobic capacity of lung cancer patients. Surg Oncol. 2021;37:101525. doi:10.1016/j.suronc.2021.101525. 28. Sebio García R, Yáñez-Brage MI, Giménez Moolhuyzen E, Salorio Riobo M, Lista Paz A, Borro Mate JM. Preoperative exercise training prevents functional decline after lung resection surgery: a randomized, single-blind controlled trial. Clin Rehabil. 2017;31:1057–1067. doi:10.1177/0269215516684179. 29. Strassmann A, Steurer-Stey C, Lana KD, Zoller M, Turk AJ, Suter P, et al. Population-based reference values for the 1-min sit-to-stand test. Int J Public Health. 2013;58:949–953. doi:10.1007/s00038-013-0504-z.
Comments (0)