
Remember me


We often encounter infection in an ascending aortic graft, which is difficult to treat. The reason is that an infection of the ascending aorta requires reoperation for artificial vessel replacement, aortic mesh filling, and long-term antibiotic therapy, which can be fatal if not effective. This report describes a case of mediastinitis one year after ascending aorta graft surgery. Postoperatively, the patient developed mediastinal hematoma on multiple occasions that was difficult to diagnose and entailed multiple median sternotomies. In this report, we summarize this rare case and the relevant literature.
The patient was a 40-year-old otherwise healthy man who was found to have a heart murmur on physical examination. Before the first surgery, he had NYHA2 heart failure symptoms due to aortic regurgitation. The diameter of the ascending aorta was 50mm. Echocardiography confirmed a bicuspid aortic valve with severe aortic regurgitation and dilatation of the ascending aorta, both of which were considered indications for surgery. He underwent aortic valve replacement with a 23-mm SJM Regent mechanical valve and repair of the ascending aorta using a 26-mm Gelweave graft at another hospital (operation 1). The patient was discharged from hospital without any problems and followed up as an outpatient.
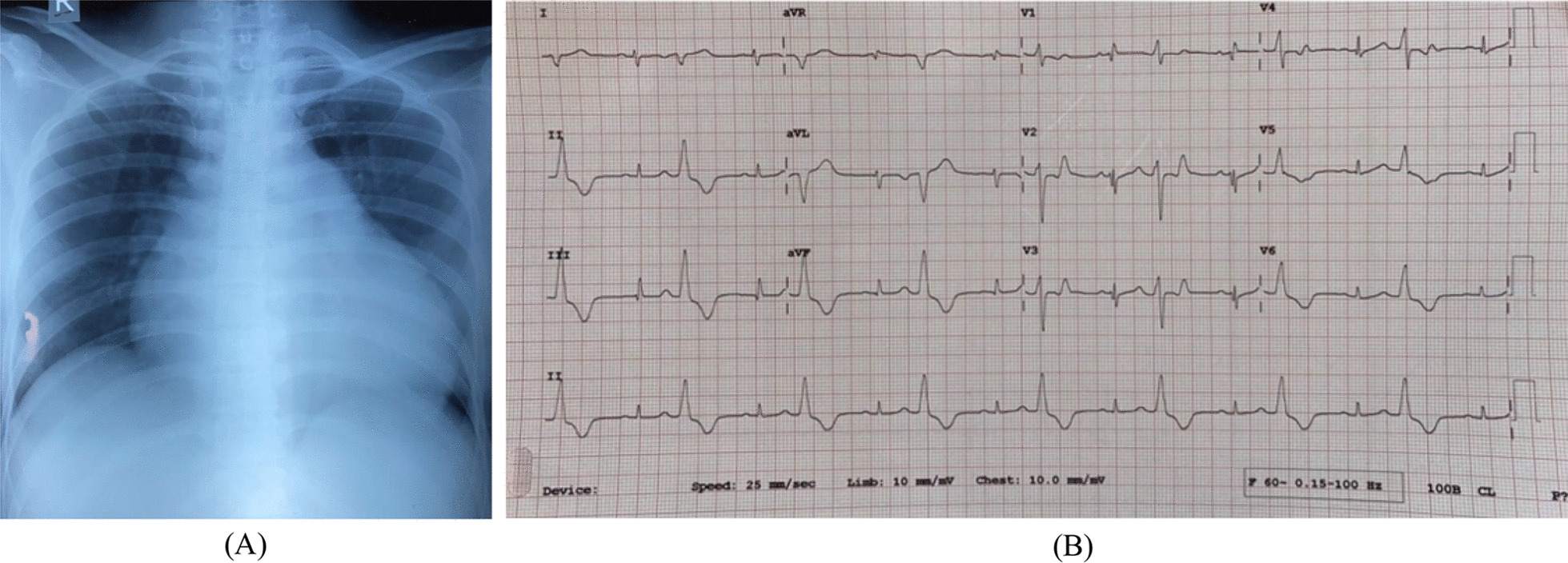
One year later, he presented with a fever of 38°C, a white blood cell count of 10,300/μL, and a C-reactive protein level of 18.3 mg/dL. CT showed mediastinitis (Fig. 1A). A blood culture revealed methicillin-resistant Staphylococcus aureus (MRSA). We performed a redo ascending aortic replacement and aortic valve replacement (operation 2). Prior to re-sternal median incision, the femoral arteriovenous vein was exposed. The next day, we confirmed hemostasis and performed omentopexy around the ascending graft (operation 3) (Fig. 1B). The patient was discharged from hospital without any problems. In POY 3, a computed tomography (CT) scan showed that the mediastinum was not filled (Fig. 1C). The mediastinum was found to be filled with greater omentum, but there was still space for fluid to accumulate there. A further CT scan obtained in POY 4 showed fluid retention around the ascending aortic graft (Fig. 1D), which was considered to be a seroma. The surrounding tissue was removed (operation 4).
Fig. 1
Findings on CT scans during the first 5 years after the initial surgery. a POY 1. Residual fluid was detected around the ascending aortic graft. An infected graft was diagnosed based on a positive blood culture and laboratory test results. b POY 1. A CT scan obtained after omentoplasty. c POY 3. A CT scan showing that the mediastinum was not filled. d POY 4 Residual fluid was seen in the anterior mediastinum around the ascending aortic graft (green arrow). CT, computed tomography; POY, postoperative year
The patient was ambulatory and did well thereafter. A CT scan obtained in POY 6 (Fig. 2A) showed fluid in the tissue around the graft but no signs of infection, and follow-up was continued. In POY 7, more fluid was found in the tissue around the graft (Fig. 2B), and fluid around the ascending aorta was compressing the heart. The left atrium was compressed, resulting in poor pulmonary venous return and decreased oxygenation. Airway compression was expected during induction of general anesthesia. After induction of general anesthesia, ECMO was immediately administered, and then, the chest was opened to remove the hematoma around the ascending aorta, which stabilized general oxygenation and hemodynamic status. Oozing was noted in the operation, indicating that the graft had failed; the graft was replaced with a 26-mm Triplex, and the patient was stable thereafter (Fig. 2C) (operation 5). The oozing ran the entire length of the artificial graft from the black line. Since the oozing was from the entire length of the artificial vessel, it was impossible to repair and had to be replaced. Two months later, fluid retention was again observed around the ascending aorta (Fig. 2D), and a diagnosis of expanding hematoma was made. After a further week, the hematoma capsule was removed (operation 7), and hemostasis was confirmed. On the following day, the left vastus lateralis muscle was filled into the anterior mediastinum (operation 8) (Fig. 2E) in collaboration with the plastic surgeons, after which the patient was discharged. However, 6 months later, he was found to have another hematoma in the mediastinum (Fig. 2F), which was removed (operation 9).
Fig. 2
Findings on CT scans from years 6 to 9 after the initial surgery. a POY 6. A mass was detected around the ascending aorta. b POY 7. A 100-mm mass was detected around the ascending aorta and the ascending aortic graft was replaced. c A CT scan obtained immediately thereafter showed slight effusion around the ascending aorta. d Two months later, fluid retention was again observed around the ascending aorta. e The hematoma capsule was removed, and after confirming hemostasis, the left vastus lateralis muscle was filled into the anterior mediastinum. f Six months later, further hematoma was found in the mediastinum. CT, computed tomography; POY, postoperative year
One year later, he was admitted to hospital with sepsis caused by MRSA. He had a fever of 38 degrees Celsius three days prior to admission. The seating of the aortic valve was observed to be unstable (operation 10). Therefore, the aortic valve was urgently replaced with a 23-mm Inspiris valve and a diagnosis of infective endocarditis was made (operation 11). The infection could not be controlled, and the patient died on postoperative day 20. The family did not wish to have a postmortem study. The patient’s disease course and details of the operations performed are shown in Fig. 3.
Fig. 3
Disease course, findings on computed tomography, diagnoses, and operations performed during years 1–9 after the initial surgery
Comments (0)