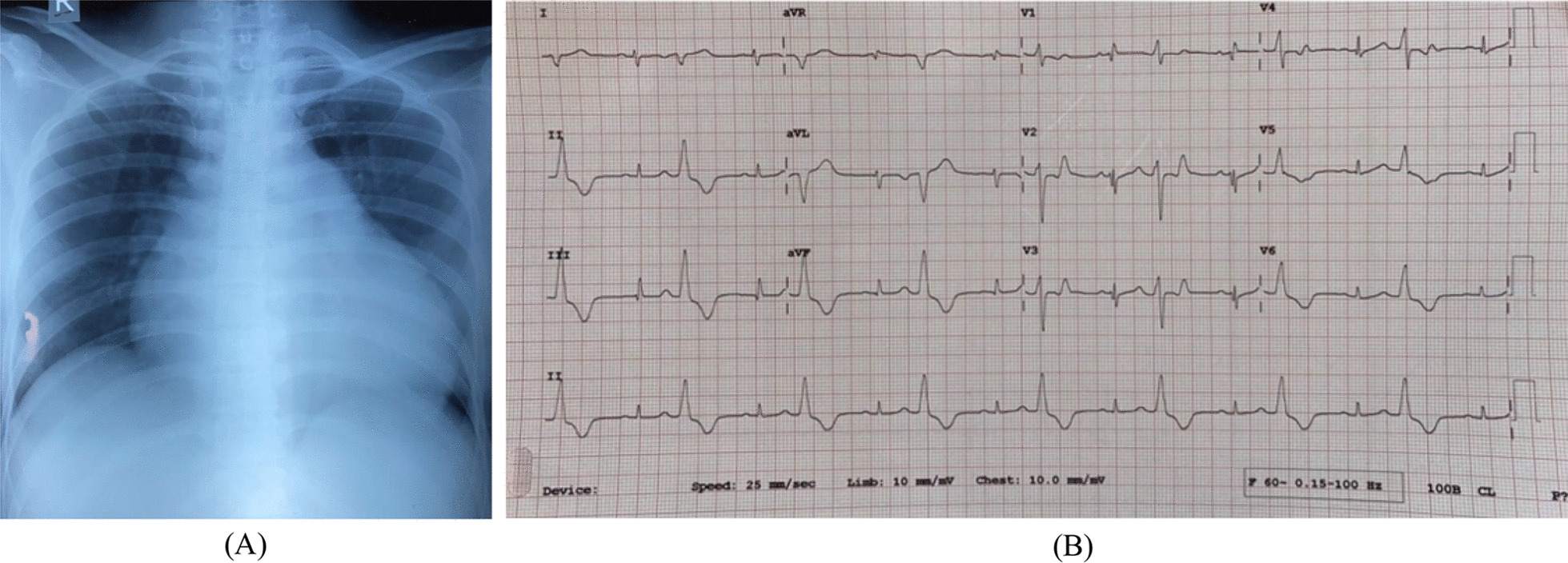
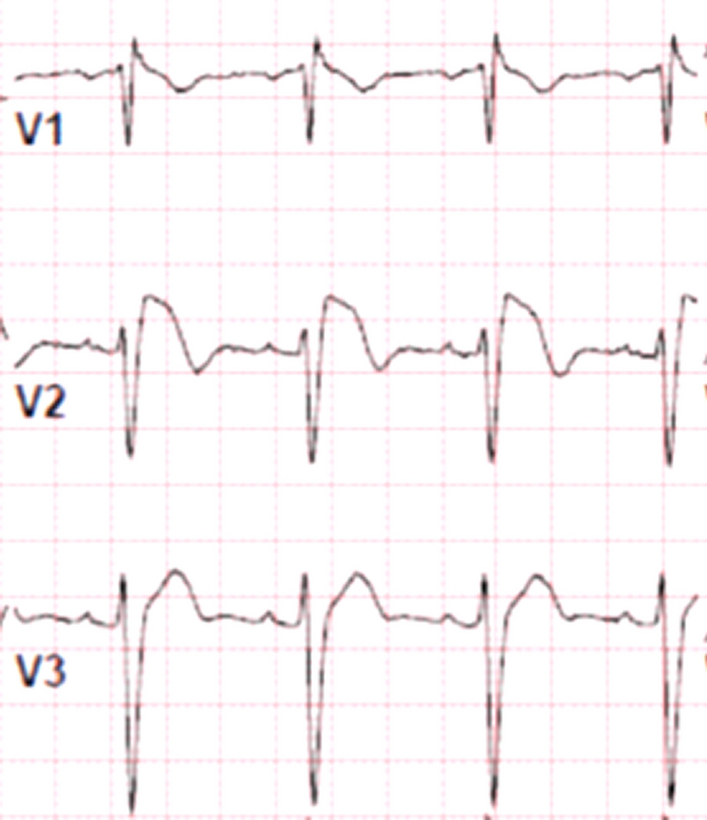
The pericardium is a double-layered fibro-serous sac that surrounds and stabilises the heart within the thorax, preventing it from overfilling, minimising friction, and protecting it from infection by neighbouring organs. When pleuro-pericardial membranes merge in the fifth week of embryonic development, the pericardium forms. Failures of this process, which may be caused by early Cuvier duct atrophy, result in congenital abnormalities such as complete or incomplete pericardial agenesis [7]. Inadequate blood supply to the pleuro-pericardium as a result of left common cardiac vein atrophy results in abnormal development of the pleuro-pericardial membranes and pericardial abnormalities early in life [4]. The most common ailment (70%) is the absence of the left pericardium, common in men. Complete pericardial aplasia (9%) is less common than right pericardial aplasia (17%) and left pericardial aplasia (7%). While the majority of individuals with congenital pericardial absence have isolated issues, around 1/3 of these children have other congenital cardiovascular and pulmonary disorders. Furthermore, these patients may have one or more of the following syndromes such as VATER (vertebral deformities, anal atresia, tracheoesophageal fistula, and radial and renal abnormalities), Marfan's syndrome, or Pallister–Killian syndrome (tetrasomy 12p). It is clinically recognised by a range of symptoms, including non-exercise-induced lancinating chest discomfort, disorientation, dyspnoea, and palpitations [4]. Chest radiography reveals a significant left lateral displacement of the heart profile without tracheal deviation, as well as a flattened and extended left ventricular border. Between the diaphragm and the heart, or the aorta and the pulmonary artery, intervening lung tissue forms a lucent region [8]. Frequently, the electrocardiogram displays bradycardia with right bundle branch block (as in our patient). Additionally, poor R wave progression as well as large P waves may be observed. Echocardiography is a type of cardiac imaging that can first provide information on the prevalence of complete pericardial agenesis [9]. During systole, the ventricular septum might shift paradoxically or flatly while maintaining normal systolic thickness, cardiac hypermobility, and an expanded RV. Additionally, echocardiography may be used to emphasise the LV's teardrop shape, bulbous ventricle, and extended atria in the apical four-chamber view [10]. Additionally, as observed in the two-chamber picture, the atrioventricular groove is significantly angulated, and the inferior wall of the left ventricle bulges outward [11]. Exercise–stress echocardiography may indicate an amplification of the heart's "pendulum-like" motion. Doppler methods may detect a drop in systolic flow and a decrease in the systolic-to-diastolic flow ratio in the pulmonary veins, most likely as a result of the lack of negative intrapericardial pressure [5]. Echocardiography, like chest X-rays, is frequently uninvolved in patients with incomplete/partial pericardial agenesis. Ventricle enlargement, herniation of atrial appendages, irregular ventricular wall motion, and ventricular abnormalities linked with coronary compression can all be recognised in some circumstances [9]. Imaging such as CT and MRI can be used to assess the extent of the defect (complete or partial), the presence of herniated structures, and the presence of further flaws. MRI is an excellent tool for detecting both partial and total pericardial agenesis. The normal pericardium is a small linear band surrounded by dense epicardial adipose tissue, moderately intense heart tissue, and surrounding adipose tissue. However, in 10% of people, a small amount of adipose tissue obscures the pericardium. The pericardium is more apparent above the right ventricle in systole.
During diastole, the normal pericardium is between 1.7 + 0.5 mm and 1.2 + 0.5 mm thick. Although not all pericardial recesses are visible on MRI, several are including the transverse pericardial sinus, which is dorsal to the ascending aorta, and the oblique pericardial sinus, which lies behind the left atrium. Additionally, an aberrant posture of the heart, bulging of the major pulmonary artery, and lung tissue interposition between the left hemidiaphragm and the inferior side of the heart, as well as between the great arteries, are all symptoms of a total left defect. Additionally, a herniated heart can be caused by a pericardial defect, evident in a partial defect [3]. CT helps in detecting interposed lung tissue between the major pulmonary artery and aorta window, which is considered pathognomonic for this condition, as well as a prominent main pulmonary artery [12]. On decubitus CT, complete defects display a rightward axis shift, which aids in the identification of entire and partial flaws [13]. By contrast, thoracoscopy is the recommended confirmatory procedure [3].
Patients with a full pericardial defect frequently have a favourable prognosis and are not treated until significant symptoms develop. However, in patients with partial pericardial agenesis, herniation of the heart due to tension on the chordal tissues can result in tricuspid regurgitation, catastrophic myocardial strangling, ischaemia, and sudden cardiac death. Unless complications arise, minor or full anomalies do not generally require repair. When herniation develops or is imminent in partial defects, the defect can be widened surgically by pericardiectomy or pericardioplasty [14]. Additionally, if the apical appendage is acutely strangled, a left atrial appendectomy may be considered [15]. Reconstruction is not suggested for a large defect such as the one in our instance, as the heart adapts to deformed architecture in general, and rectification attempts may result in unstable flow patterns [16]. The majority of patients with a complete defect have a reasonable chance of healing and only require surgery if complications or uncontrollable symptoms emerge [4]. Recommendations given to patients with pericardial agenesis depend on the individual’s specific symptoms, associated conditions, and overall health. However, here are some recommendations that may be considered. (1) Regular cardiac monitoring, they may need regular check-ups, electrocardiograms (ECG/EKG), echocardiograms, and cardiac imaging tests to evaluate the function and detect any potential complications. (2) Lifestyle modifications include adopting a healthy lifestyle with mild regular physical activity, weight management, avoidance of smoking and consumption of alcohol, and managing other health conditions such as high blood pressure or cholesterol levels. (3) Symptom management for some individuals with pericardial agenesis may experience symptoms like chest pain and breathlessness, which are managed symptomatically at times with the help of a healthcare professional. (4) Monitoring the complications for individuals with pericardial agenesis may be at risk of certain complications like arrhythmias or cardiac herniation. Monitoring for these complications and managing them appropriately is essential.



Comments (0)