
Remember me





The insertion of dental implants into the maxillary sinus is the most common complication that occurs in the maxilla, and various studies have been conducted on the shape of the maxillary sinus associated with implant placement. In addition, various studies have been conducted on the factors affecting the size and shape of the maxillary sinus and their influence on panoramic features [6, 17, 18].
The penetration of dental implants into the nasal cavity is another complication. Despite the fact that it can be asymptomatic and may remain in the nose for many years [16, 19, 20], when complications do occur, unilateral mucopurulent and nasal discharge are the most prevalent symptoms in such cases [11]. It can also alter airflow accompanied by pain and discomfort [16, 21]. Hence, it is important to evaluate the nasal cavity by radiological examination to avoid perforation and secure an appropriate bony volume. Also, if the alveolar bone is narrow, implant placement requires increased attention, and a more meticulous assessment is necessary even after the placement.
This study showed three cases of implant penetration in the nasal cavity with varying severities. The common feature of the (CB)CT images of the presented patients was that the size of the maxillary sinus on the affected side was relatively small and the nasal cavity was relatively widened horizontally. In a study by Park et al., the three-dimensional CBCT image was analyzed using the concept of inferior meatus pneumatization as a characteristic of the presence of implant fixtures invading the enlarged nasal cavity [16]. This was similar to the presented three cases; CBCT showed relatively small maxillary sinus and enlarged inferior meatus. We focused on how these changes appear in the panoramic radiographs and found the following common features: (1) the horizontal radiopaque line of the hard palate was observed to be inferior to or similar to that of the antral floor; (2) the bone between the lateral wall of the nasal cavity and the medial wall of the maxillary sinus was emphasized and observed in a triangular shape, as if the bony volume was larger than the actual three-dimensional volume.
Understanding the image of the nasal cavity in a panoramic radiograph cannot be explained simply. The overall changes in the volume and shape of the nasal cavity, adjacent maxillary sinus, and their three-dimensional relationship with the focal layer on panoramic radiography have a complex effect on the obtained image features of the nasal cavity.
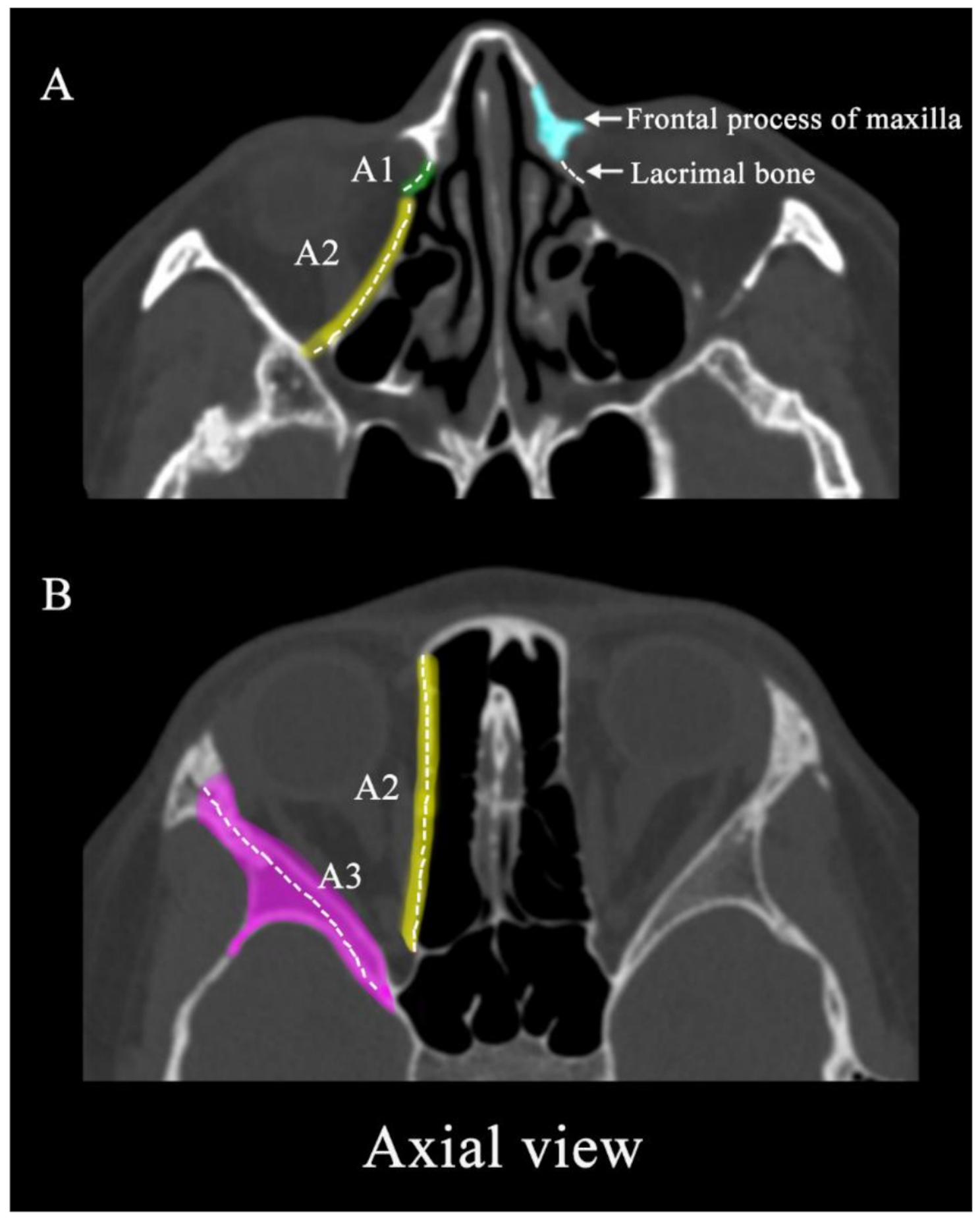
The lateral demarcation line of the nasal cavity in the panoramic image is the nasal pyriform aperture rather than the actual lateral wall of the nasal cavity in the actual three-dimensional anatomy (Fig. 6, line 2).
Fig. 6
The movement and process of the central ray of the panoramic radiograph around nasal cavity is matched and marked by same number. The vertical lines of the panoramic radiography (a) and the yellow arrows of the three-dimensional image (b) shows the path through which the central ray of the X-ray beam passes at the moment. When a central ray passes through the nasal septa, it passes vertically (number 1). As the central ray moves, it passes the corner of the abduction side, the nasal pyriform aperture of the maxilla (number 2), rather than the actual lateral wall (red line)
In addition, the three-dimensional nasal floor not only forms the radiopaque line below the demarcated nasal cavity mentioned above but it also extends posteriorly as a radiopaque line, often known as the hard palate line, which is anatomically the palatal process of the maxilla (Fig. 7a) [22]. This phenomenon is similar to the posterior extension of the inferior nasal concha observed on panoramic radiography. The nasal cavity and maxillary sinus are three-dimensionally separated adjacent structures; however, in obtaining panoramic radiographs, both the nasal cavity and maxillary sinus exist in the same path through which X-rays pass. Even though the actual nasal cavity is present with a long posterior overlap along the nasal floor line (Fig. 7b), it can be mistakenly assumed that only the maxillary sinus, with its boundaries respectively visible, provides information in that region in the panoramic image. For example, in the case 1, when clinical dentists first encounter the panoramic radiograph, there is a high probability of erroneously assuming that implants have been placed in the maxillary sinus, as implant fixtures can be seen on the outer side of the corticated nasal cavity boundary, leading to misinterpretation. Therefore, when interpreting such radiographs, it is crucial not to overlook the fact that information from both the maxillary sinus and the nasal cavity is presented together. Especially when the maxillary sinus appears small, considering that the nasal cavity occupies a broader area in that region can aid in the accurate interpretation.
Fig. 7
a In order to confirm the panoramic features of the nasal floor, the gauze soaked in contrast media is placed on the nasal floor of the plastic skull and a panoramic radiograph is obtained. The three-dimensional nasal floor not only forms a radiopaque line below the demarcated nasal cavity (blue arrow) but it also extends posteriorly as a radiopaque line, often known as the hard palate line, which is anatomically the palatal process of the maxilla (red arrow). b The actual nasal cavity is present in the panoramic image, with a long posterior overlap along the nasal floor line
In cases of hypoplasia or atrophy of the maxillary sinus, three-dimensional reduction of the maxillary sinus displaces the anteromedial margin of the sinus posteriorly and the antral floor superiorly. The greater the anterior-posterior difference between numbers 2 and 3 (Fig. 6b), the larger the area between numbers 2 and 3 in the panoramic image (Fig. 6a), which causes an overestimation of the available maxillary bone in panoramic radiographs. In addition, the antral floor line is observed to be similar or superior to the hard palatal line.
Yoshida et al. revealed the influence of depression of the maxillary sinus anterior wall on panoramic radiographic appearance [17]. They showed that the diagonal line on a panoramic image was related to the depression of the anterior wall of the maxillary sinus. Since sinus volume decreased due to inward retraction of the maxillary sinus walls, including not only the anterior wall but also the medial or inferior wall, this phenomenon can be closely related to the imaging features presented in this paper. Therefore, in the panoramic features, the lateral region of the reduced maxillary sinus could be related to the diagonal line, the medial wall could be related to the triangular overestimated bone, and the floor could be related to the similar heights of the nasal and antral floors.
Normally, even if this phenomenon occurs, it does not cause problems. However, if alveolar bone resorption is severe and implant placement is considered in the maxilla, panoramic evaluation may cause overestimation of the available residual bone, particularly in the maxillary canine/premolar region. In addition, since the alveolar bone of the maxilla is in buccoversion, bone resorption causes an unfavorable bone shape in which implantation can be planned towards the nasal cavity [23]. This can influence the treatment plan. If the superior region of planned implant location is not the maxillary sinus, it may lead to changes in the plan regarding bone grafting and other considerations. Moreover, there could be possibilities of changing the implant location to a more favorable position. Therefore, if panoramic radiographs reveal the aforementioned features, careful evaluation of the residual bones using additional three-dimensional images is required accordingly.
The clinical importance of this information lies in the ability to acknowledge the potential occurrence of nasal cavity perforation as an accidental complication during the surgical procedure. Understanding the posterior extension of the nasal cavity in panoramic imaging and being aware of its presence are crucial in reducing complications resulting from nasal cavity perforation. This knowledge significantly influences the establishment of treatment plans, including the selection of appropriate implant types and their placement. In addition, it helps to properly decide the need for additional three-dimensional imaging, which may also influence the determination of the ideal implant placement position in the treatment plan.
The limitation of this report is that only three cases were presented and discussed, and it did not address how presented common panoramic features can manifest diversely in actual patients. Also, further research through well-designed experiments is necessary to investigate how phenomena such as nasal cavity pneumatization and sinus hypoplastic change increase with age and how these changes are reflected in panoramic imaging characteristics.
Comments (0)