
Remember me





The entire cohort of OME patients consisted of 53 women (50.5%) and 52 men (49.5%), the mean age was 50.5 ± 16.3 years, and the age range was 18 to 90 years (Table 1). Seventy-seven patients (73.3%) had one affected ear and 28 patients (26.7%) had two affected ears. We therefore performed an analysis of 133 affected ears. There were 65 patients (80 affected ears) in the COVID-19 group and 40 patients (53 affected ears) in the control group.
Table 1 Demographic and clinical characteristics of patients in the COVID-19 and control groups.*Characteristics of patients in the COVID-19 and control groupsThe most common aural symptoms in the COVID-19 group were hearing loss (86.2%) and aural fullness (72.3%); significantly fewer patients in the control group reported aural fullness (47.5%, P = 0.011). Only 12 patients (18.5%) in the COVID-19 group and 5 patients (12.5%) in the control group reported transient earache (P = 0.421). The duration of aural symptoms before visiting the clinic was 16.5 ± 16.4 days in the COVID-19 group and 79.3 ± 81.4 days in the control group (P < 0.001).
Twenty-one patients (32.3%) in the COVID-19 group reported previous OME and complete resolution for more than 6 months. A greater percentage of patients in the control group had a history of OME (50%), but the difference was not significant (P = 0.071). The control group had significantly higher percentages of patients with previous of tympanocentesis (40.0% vs. 13.8%, P = 0.002) and VTI (22.5% vs. 6.2%, P = 0.029). The two groups had similar percentages of patients with hypertension (13.8% vs. 15.0% P = 0.87), diabetes mellitus (6.2% vs. 5.0%, P = 1.0), and uterine fibroids, breast cancer, bladder cancer, and other non-head and neck benign or malignant tumors (24.6% vs. 12.5%, P = 0.132).
We also analyzed the initial ABG and tympanometry results in 133 ears. The difference in the initial average ABG in the COVID-19 group (22.8 ± 8.4 dB, range: 10.0 to 47.5 dB) and the control group (25.8 ± 10.6 dB, range 10.0 to 53.8 dB) was only 2.9 ± 1.9 dB (P = 0.0784). Overall, 65 of 80 ears (81.25%) had a type B tympanogram, and the other 15 ears (18.75%) had a type C tympanogram in COVID-19 group.
Treatments and outcomes of patients in the COVID-19 and control groupsThe patients received various treatments for OME, mainly intranasal steroid, nasal decongestant, mucolytics (Table 2). A small number of patients were prescribed oral antibiotics, systemic steroids, or ear drops that contained a corticosteroid and an antibiotic. Significantly more patients in the COVID-19 group received a nasal decongestant (56.9% vs. 35%, P = 0.029), but the two groups did not differ in the other types of other conservative treatments. Significantly more patients in the control group received tympanocentesis (65% vs. 41.5%, P = 0.02).
Table 2 Treatments and outcomes of patients in the COVID-19 and control groups*At the time of the follow-up assessment (62 to 165 days following the first visit), the COVID-19 group had 42 patients (64.6%) who had complete resolution, 20 (30.8%) who had improvement, and only 3 (4.6%) who had persistent OME. In contrast, the control group had 21 patients (52.5%) with persistent OME. The COVID-19 group had a significantly better outcome than the control group (P < 0.001).
Factors associated with OME outcomeWe then performed a logistic regression analysis to investigate the relationship between different variables and OME outcome, in which “complete resolution” and “improvement” were considered as good outcomes, and “persistence” was considered a poor outcome (Table 3). The univariate (unadjusted) logistic regression analysis indicated that outcome was associated with previous COVID-19, duration of aural symptoms, history of OME, history of tympanocentesis, and history of VTI.
Table 3 Univariate logistic regression analysis of the association of different variables with OME outcome of complete resolution or improvementWe then performed multivariate analyses using three different models that adjusted for different confounding factors (Table 4). The significance of the relationship between previous COVID-19 and OME remained after adjustment for age and sex (Model I), duration of aural symptoms, history of OME, history of tympanocentesis, and history of VTI (Model II), and all six of these variables (Model III).
Table 4 Multivariate logistic regression analysis of variables associated with OME outcome of complete resolution or improvement in models that adjusted for different confounders*We analyzed the recovery times in the 62 patients in COVID-19 group who had good outcomes (complete resolution or improvement; Table 5). For this analysis, we classified the recovery time as less than 2 weeks, 2 to 4 weeks, 4 to 8 weeks, and more than 8 weeks. Twenty-one patients (33.9%) had relief of symptoms within 2 weeks and 30 patients (48.4%) had relief of symptoms in 2 to 4 weeks. The duration of aural symptoms before the initial presentation was associated with the time needed for recovery after initial presentations (P = 0.025). None of the other analyzed parameters were significantly associated with recovery time.
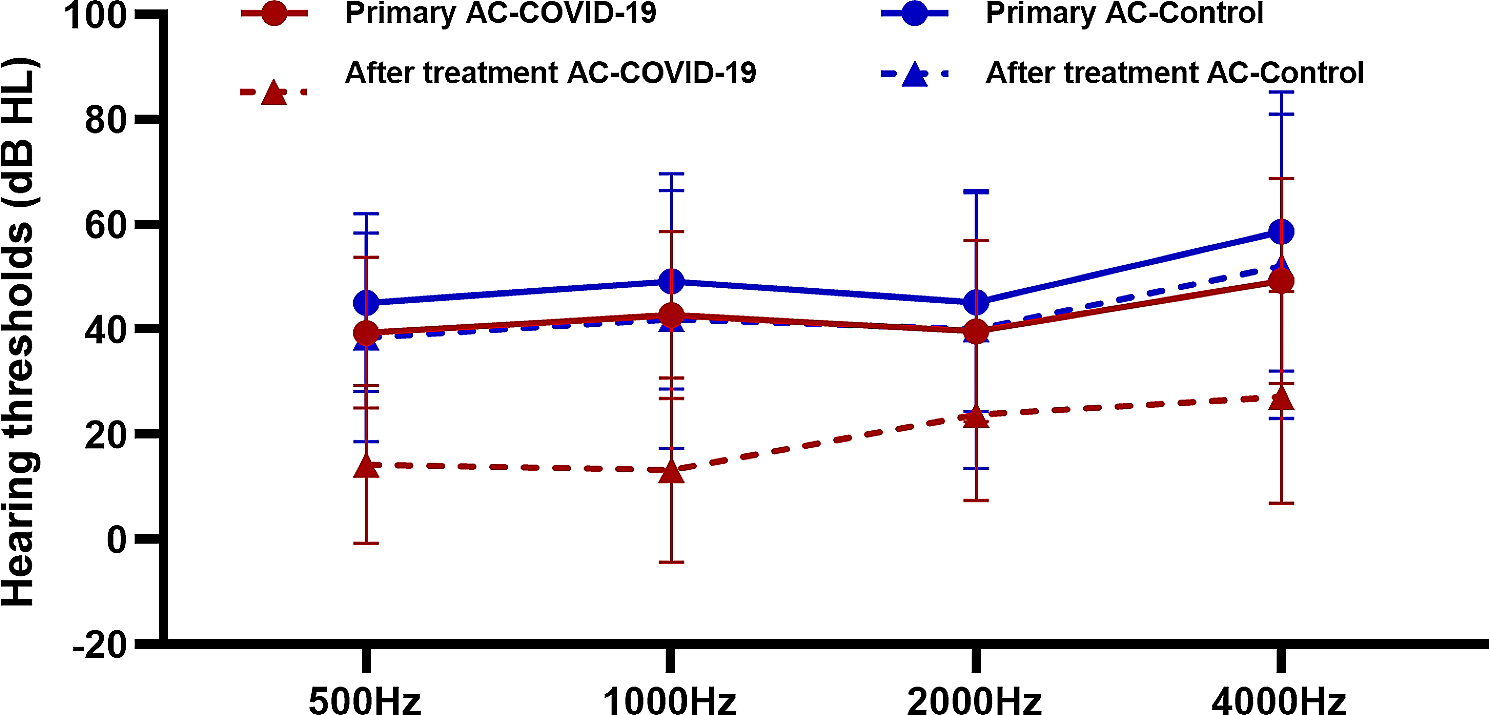
Table 5 Relationship of patient characteristics with time needed for OME outcome of complete resolution or improvement.*We used PTA and tympanography to assess the hearing thresholds at the primary clinic visit and the last visit after treatment in 45 of 65 patients (69.2%) in the COVID-19 group and 29 of 40 patients (72.5%) in the control group (Fig. 1). These data were for 74 patients and 96 ears. After treatment, the average ABG decreased to 10.5 ± 9.3 dB (range: 0–36.3 dB) in the COVID-19 group and decreased to 19.6 ± 12.2 dB (range: 0–43.8 dB) in the control group (P < 0.0001). Thus, the COVID-19 group had a significantly greater improvement in hearing threshold.
Fig. 1
Hearing thresholds at four frequencies before and after treatment in the COVID-19 and control groups
Comments (0)