RMT increased Pimax by 32% in people with chronic tetraplegia. This improvement in inspiratory muscle strength affected some aspects of load magnitude perception but had no effect on load detection threshold. For load magnitude perception, there was an overall decrease in Borg effort ratings after the 6-week intervention that was not related to the increase in Pimax. However, there was a training-related increase in Pipeak during loaded breaths, which decreased the slope of the relationship between Borg rating and Pipeak. That is, for a given change in Pipeak, the inspiratory loads were perceived to be less effortful when inspiratory muscle strength improved. The higher Pipeak offset the increase in Pimax so that contraction intensities (%Pimax) for the six resistive loads remained the same despite improvements in inspiratory muscle strength. Consequently, the perceptual response to loading did not change after RMT when Borg rating was plotted against Pipeak (%Pimax).
Our expectation that improvements in Pimax would reduce the relative contraction intensities of the inspiratory muscles, leading to a given inspiratory load being perceived as less effortful, did not eventuate. Borg ratings decreased after the training intervention, but the active and sham groups had similar changes. This suggests a “learning” effect despite the 6-weeks between test sessions. Participants had no experience breathing with an added resistive load and may have been more comfortable with the inspiratory loading setup during the second test session. In our previous study [14], a similar decrease in Borg ratings was observed in healthy able-bodied participants when the load magnitude perception task was repeated about a week apart with no other intervention. Eastwood et al. [16] suggested that changes in breathing patterns could explain the learning effect observed for progressive threshold loading where maximal threshold pressure increased and rate of perceived exertion decreased over successive days when there was no change in Pimax. In the present study, there was no difference in resting breathing values between test sessions (Table 2), but participants may have slightly altered inspiratory times for loaded breaths after their first session of the load magnitude perception task (Table 3), as will be discussed later. Alternatively, Boswell-Ruys et al. [3] reported in the primary study that the resistance of the sham training device was not negligible, requiring a threshold pressure of 3.6 cmH2O. It is possible then that the stimulus generated by the sham device was sufficient to induce a training effect on Borg ratings without increasing inspiratory muscle strength. The learning-effect explanation seems more plausible, which would have significant implications for previous training studies in healthy able-bodied participants as they do not include a control (sham) group for comparison [e.g. 5, 6]. Pimax increased by 51% and 60% in those previous studies, almost twice as large as the 32% improvement obtained in this study, so the likelihood of a training-related decrease in load ratings as reported in [5, 6] is greater if a training effect was present. Since the contribution from a learning effect on load ratings cannot be determined in those previous studies, their findings should be interpreted with caution as the training-related decreases in perceived magnitudes may be overstated.
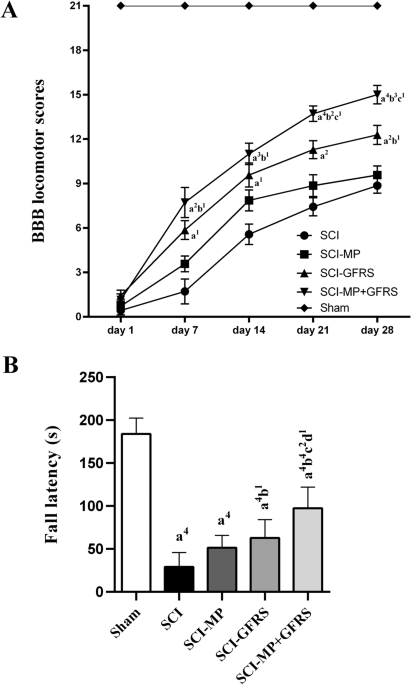
RMT did not directly lower Borg ratings. However, the 32% improvement in inspiratory muscle strength decreased the slope of the relationship between Borg rating and Pipeak by 38% (Table 4) so the change in perceived magnitude of an inspiratory load was less sensitive to a given change in absolute Pipeak. This decrease in slope magnitude was achieved primarily through an increase in Pipeak, which was unexpected as the same set of resistive loads was used for both test sessions. In healthy able-bodied participants, Pipeak did not increase after inspiratory muscle training for loads ranging from 3.5 to 50.6 cmH2O/l/s when inspiratory flow was unconstrained [6]. For people with chronic tetraplegia, it is not clear why there was a consistent increase in Pipeak in the active group after training (Fig. 3B). It appears that participants were unaware that the force of contraction generated by the strengthened inspiratory muscles was more than adequate to overcome the added resistance to breathing. The loss or impairment of afferent inputs from muscles acting on the chest wall is probably important here as the increase in Pipeak kept contraction intensity (central drive) the same after training, as indicated by the lack of a training-related difference in slopes between Pipeak (%Pimax) and log-transformed resistance, a behaviour more consistent with an open-loop control system. As a result, when Borg rating was plotted against Pipeak (%Pimax) to represent contraction intensity (Fig. 3D), the training effect on slope magnitude disappeared. That is, for a given change in contraction intensity, the inspiratory loads were perceived to be just as effortful irrespective of the absolute Pimax. A constant relationship between load ratings and contraction intensity was also observed in healthy able-bodied participants after training [5, 6]; although, constancy was achieved via different means to those with chronic tetraplegia. Here, contraction intensities were maintained as slope magnitudes were reduced whereas in healthy able-bodied participants load ratings and contraction intensities both decreased, shifting the relationship between load rating and Pipeak to the left. Regardless, these findings support the suggestion by Luu et al. [12] that load magnitude perception in chronic tetraplegia reflects the contraction intensity of the inspiratory muscles and not the absolute inspiratory muscle force, and as in healthy able-bodied participants [5, 6], is not affected by training-induced changes in Pimax.
As mentioned earlier, participants seemed to have altered their breathing pattern during loaded breaths in the second session of the load magnitude perception task. The direct relationship between the perceived magnitude of an inspiratory load and inspiratory time in the first test session (Table 4) replicates what has been reported previously [e.g. 11, 12, 17]. However, after the 6-week intervention, the positive relationship between Borg rating and inspiratory time was inverted in the sham group when Pipeak was used as the covariate in the mixed linear model; no change in the relationship was observed in the active group, perhaps due to the increased Pipeak after training. When Pipeak was expressed as a percentage of Pimax, the relationship between Borg rating and inspiratory time changed from positive to negative in both the active and sham groups. Whether this behaviour is normal or limited to chronic tetraplegia is unknown. Of the previous studies that have repeated a load magnitude perception task in the same participants, two did not investigate the relationship between load ratings and inspiratory time [5, 14] and the other assumed a positive relationship and divided load ratings by a fixed power of inspiratory time [6]. Inspiratory time was identified as an important component in the learning effect observed for progressive threshold loading [16]. For that task, inspiratory times decreased following successive tests, presumably to increase the recovery time of the inspiratory muscles and prolong endurance. Here, the inverse relationship in the second test session indicates longer inspiratory times were associated with lower Borg ratings. While inspiratory times appeared to increase during the second session, there was no accompanying decrease in inspiratory flow, and hence pressure, that would be required to reduce load sensations. Further investigations are needed to understand the relationship between load ratings and inspiratory time as our findings suggest that a positive relationship should not be assumed when testing non-naïve participants or conducting repeated sessions on the same participants.
Increased Pimax did not lower load detection thresholds. Nor did repeating the load detection task in the sham group after the training intervention, although the underestimation of detection thresholds in the sham group prior to training may have masked any learning effect (Fig. 2A). These results reproduce those found in healthy able-bodied participants [5, 13, 14] and indicate that load detection is not dependent on inspiratory muscle strength.
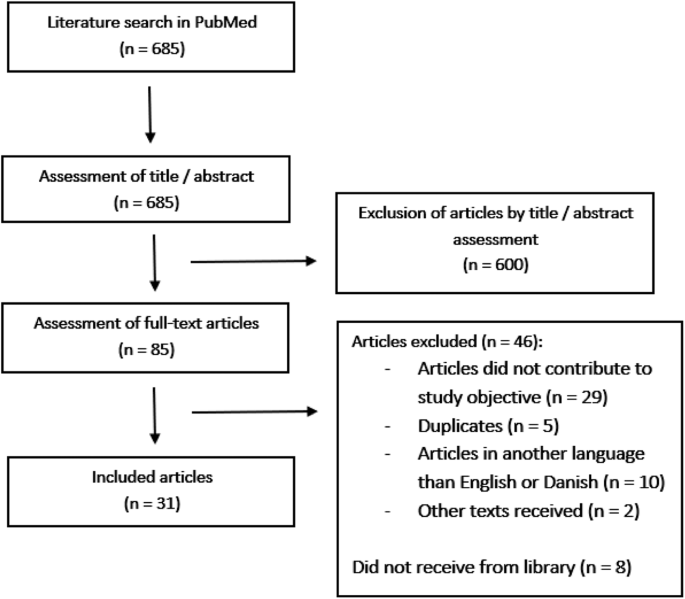
Not all participants completed the load detection and load magnitude perception tasks (Fig. 1), and this limitation resulted in an unevenly distributed study population for level of injury and motor completeness (Table 1). However, neither factor alone indicates the level of inspiratory muscle impairment as Pimax was similar between the sham and active groups prior to RMT (Table 2). Moreover, our findings showed that, for respiratory sensations, contraction intensity was the determining factor in a participant’s perceived effort of an inspiratory load. As this was a secondary analysis of a randomised controlled trial, it is possible that the present study was not adequately powered to compare differences between the sham and active groups for our non-significant findings.
In conclusion, our findings present a dichotomy for recommendation of RMT as part of rehabilitation for people with chronic tetraplegia. On the one hand, improved inspiratory muscle strength reduced the slope of the relationship between Borg rating and absolute Pipeak, which suggests RMT has the potential to lessen the increase in perceived effort when the resistance to breathing increases. For example, this would occur during respiratory distress from pneumonia or exercise, exacerbations of asthma or airway disease, or from weight gain. On the other hand, RMT did not produce an overall decrease in Borg effort ratings across the loads, which suggests a limited benefit in prescribing RMT solely to reduce perceived effort of breathing at rest. However, this should not be considered a contraindication for RMT as increasing inspiratory muscle strength also reduces respiratory complications and improves quality of life [3]. Selection of a suitable training load that will increase muscle strength while minimising breathing discomfort is therefore important to optimise recovery. The comparable relationships between Borg effort rating and contraction intensity for people with chronic tetraplegia and able-bodied controls [12] suggest training protocols that are well tolerated by able-bodied participants will equally be well tolerated by people with chronic tetraplegia, as long as training protocols are based on changes in contraction intensity relative to maximum rather than the physical properties of the load.

留言 (0)