In all children with impaired consciousness, the preservation of vital functions according to ABC guidelines (airway, breathing, circulation) has absolute priority. The diagnosis and treatment must be performed simultaneously. A quantitative assessment of the disorder of consciousness has to be rapidly carried out. The standard instrument for this is the Glasgow Coma Scale (GCS; [4]), which is scored between 3 and 15, with 3 being the worst and 15 the best. It is composed of three parameters: best eye response (A), best verbal response (V), and best motor response (M). The components of the GCS should be recorded individually; for example, A4V3M3 yields a GCS score of 10. The Pediatric Glasgow Coma Scale (PGCS) has been validated for children under 2 years of age ([5]; Table 1). Brainstem reflexes are not considered in the GCS.
Table 1 Pediatric Glasgow Coma ScaleBrief neurological examination
A brief neurological examination includes testing of the eyes and motor function as well as for the presence of meningism.
Eyes.
A brief examination includes testing of eyeball position and pupillomotor function. Non-convulsive status epilepticus should not be overlooked. Open eyes with gaze deviation to the side are highly suggestive of an ictal state. The pupils are usually wide in this case.
Unilateral pupillary areflexia to light indicates transtentorial herniation into the supratentorial space or increased intracranial pressure.
Bilaterally dilated pupils are found in cerebral anoxia or ischemia. However, catecholamine administration or intoxication by anticholinergics, amphetamines, cocaine, and carbon monoxide can mimic similar pupillary findings. Intoxication by cholinergics, barbiturates, or opiates is possible in the case of equally narrow pupils on both sides.
In cases of impaired consciousness with unilaterally/bilaterally nonreactive dilated pupil(s), an emergency CT of the skull must be performed prior to further diagnostic workup [1, 2].
Motor skills.
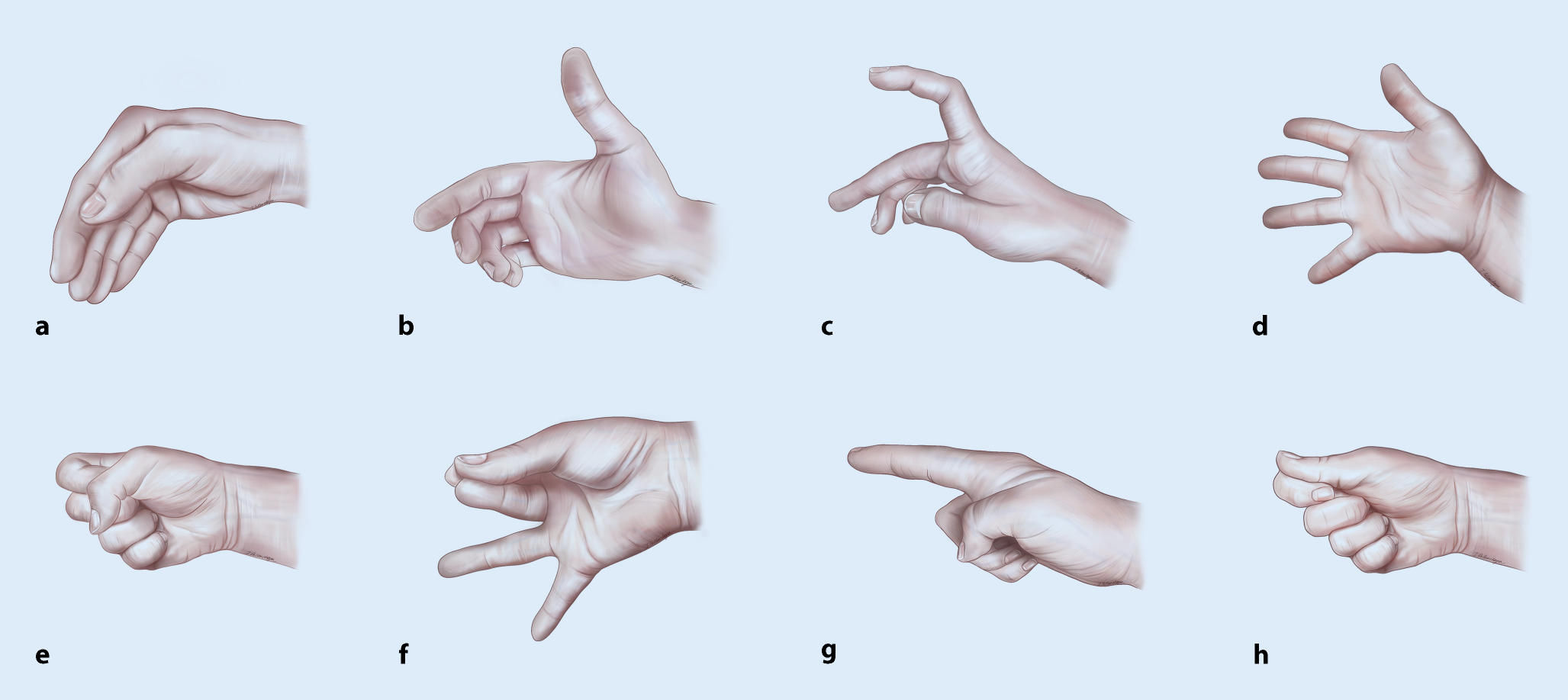
The most common cause of acute hemiparesis in children is postictal paresis (Todd’s paresis), but stroke or encephalitis is also possible. Symmetrical decorticate posturing or decerebrate posturing indicates brainstem dysfunction (herniation, trauma, hemorrhage).
Meningism in childhood is mainly due to meningitis, while subarachnoid hemorrhage is much less common. In young children, meningism is not obligatory in meningitis. Attention should be paid to the tension or bulging of the fontanel.
Physical examination
In particular, attention must be paid to the respiratory pattern, skin findings, halitosis, and evidence of trauma. Hematomas at atypical sites are found in child abuse.
Kussmaul breathing is indicative of (diabetic) ketoacidosis, while periodic (Cheyne–Stokes) or apneic respiration indicates diencephalic or brainstem involvement. The combination of bradypnea, arterial hypertension, and bradycardia is referred to as Cushing’s triad. It is a late sign of increased intracranial pressure and is usually indicative of impending herniation of the medulla oblongata.
Prolonged recapillarization time of > 3 s, petechiae, or exanthema is suggestive of infection or shock. Jaundice beyond the neonatal age suggests liver failure.







留言 (0)