
Remember me


Vagus nerve stimulation is an additive therapy for the treatment of refractory epilepsy, approved in Europe since 1994 and in the United States since 1997.
The VNS Therapy® system (LivaNova PLC, Houston, TX, USA) consists of an implanted, battery-powered pulse generator that delivers, via an implanted electrode, electrical signals to the vagus nerve at regular intervals (“OFF time”) of, e.g., 3 or 5 min with predefined stimulation ON times of, e.g., 30 s—around the clock, every day and every night. In addition, by means of a magnet, the patient or caregiver can externally trigger an additional, usually stronger “on-demand stimulation” in the VNS generator with the aim of thereby interrupting an already ongoing seizure. Finally, the newer VNS generator models available since 2013 and 2017 (Model 106 AspireSR® and Model 1000 Sentiva®, respectively, LivaNova PLC) offer—in addition to the aforementioned basic functions—the possibility of “responsive” autostimulation: These generators can detect heart rate. If there is now a rapid increase in heart rate above a predefined threshold, this is interpreted by the generator as “ictal tachycardia,” which leads via a closed-loop system to the triggering of additional, so-called autostimulation. This is sometimes preset to be stronger and usually last longer (e.g., 60 s) than the basic stimulation pulse and—as with triggering by means of a magnet—has the goal of interrupting an already ongoing seizure. All settings of the VNS stimulation parameters (“output current” [mA], signal frequency [Hz], pulse width [µs], signal ON and OFF times) are individually titrated and repeatedly checked or modified during the course of therapy to achieve the best balance between anticonvulsive effect and undesirable side effects.
Sleep-related breathing disorders under VNSCommon side effects described early on include stimulus-dependent hoarseness, voice disturbance, and coughing [21]. In addition, effects on sleep or daytime wakefulness were also described early on: A positive effect on objective sleep parameters was shown for VNS in epilepsy in a study of 15 children [12]. In two studies of adults, prolonged sleep latency, as a marker for improved daytime vigilance, was found after 3 and 6 months, respectively, in patients with no more than 1.5 mA VNS stimulation current in multiple sleep latency tests, independent of anticonvulsant response. However, at higher current levels (> 1.5 mA), this effect appeared to be reversed [11, 22]. As a plausible explanation for a reduction in sleep quality especially under high VNS current levels, it was shown retrospectively that VNS stimulation induces sleep-related respiratory disturbances [14, 23, 25, 28]. This observation was confirmed in two comparative studies: In the first [23], polysomnographies were performed for 16 patients before and after initiation of VNS therapy, with recording of an apnea–hypopnea index (AHI) > 5/h in one patient before VNS and in five patients under VNS, with AHI values between 6 and 11/h, in each case indicating a mild sleep apnea syndrome (SAS). A later study with a similar design [28] pointed in the same direction: Whereas SAS was found in only two of the 18 patients studied before VNS therapy, VNS caused a worsening in AHI in one of these two (but an improvement in the other) and new-onset sleep apnea in four of the 18 patients. The cause of apnea induction by VNS seems to be accidental costimulation of the lateral branches of the vagus nerve, the recurrent nerve, and the superior laryngeal nerve, which leads to a toning of their motor supply areas in the pharynx and on the left vocal cord and thus to—laryngoscopically proven—restriction of the airway during VNS-ON phases [37]. Attempts to counteract these VNS-induced apneas with continuous positive airway pressure (CPAP) therapy proved ineffective in most patients [24]; in one patient with comorbidity of epilepsy and obstructive sleep apnea syndrome (OSAS), VNS had to be deactivated to enable adequate CPAP titration [7]. The reason for the ineffectiveness of CPAP on VNS apnea is likely due to the different pathophysiologies: Obstructive SAS is due to wall weakness of a hypotonic soft palate that cannot withstand the negative pressure during the inspiratory phase and collapses. In VNS-induced apnea, however, as described above, electrical stimulation leads to toning and constriction in the soft palate and thus to upper airway restriction, which cannot be prevented even by CPAP.
This problem is of clinical relevance: In around one tenth of the 225 patients who underwent implantation in Hamburg and then treated at our outpatient clinic, we have the clinical impression that with VNS an SAS has either newly developed or a pre-existing SAS has been relevantly worsened, as shown in the example in Fig. 2 of one of our patients. In her case, we were able to objectively identify the induction of relevant apneas in our sleep laboratory, which is affiliated to the “epilepsy monitoring unit”: We extended the usual polysomnography with an additional electrode at the neck, placing it directly over the point at which the VNS electrode cable is attached to the vagus nerve. This facilitated visualization of the VNS stimuli, enabling the correlation between VNS stimuli and the occurrence of sleep-related breathing disorders.
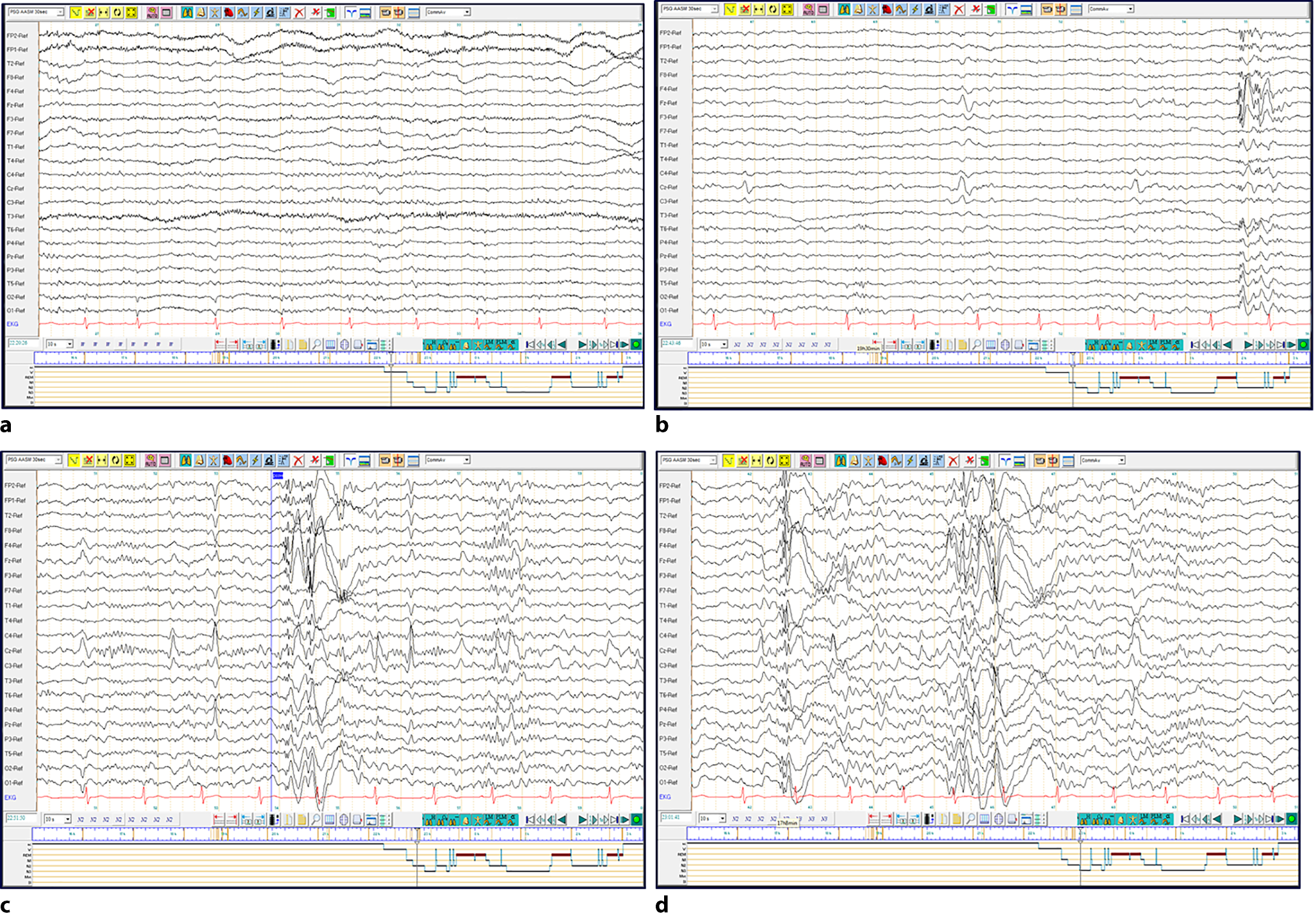
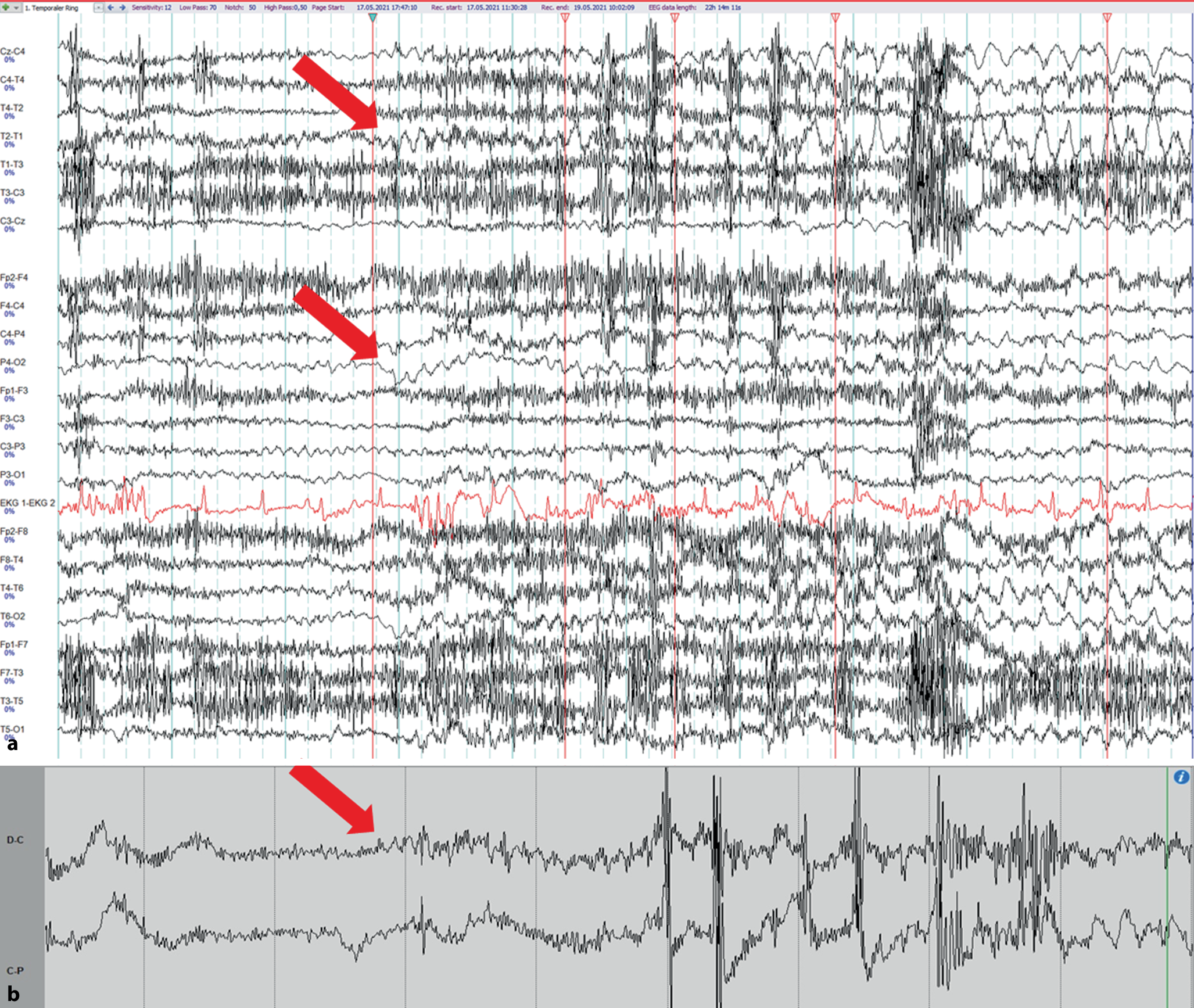
Fig. 2
Recording of vagus nerve stimulation (VNS)-induced apnea in extended polysomnography. A 30‑s polysomnography in non-rapid eye movement sleep with an additional electrode over the attachment point of the VNS stimulation electrode on the vagus nerve (EMG channel 1, green) to visualize the activity of the VNS. With the onset of the stimulation phase, apnea is evident at the cessation of nasal flow with reduced and opposing thoracic/abdominal excursions. At the end of VNS stimulation, breathing resumes. With the usual delay of 10–30 s, consecutive oxygen desaturation occurs. During the night studied, and under a VNS output current of 1.75 mA, this female patient was found to have 22 times more respiratory disturbances per minute of sleep in VNS-ON phases than in VNS-OFF phases; 45% of all VNS-ON phases were accompanied by respiratory disturbances
The induction of sleep-related respiratory disturbances has been increasingly perceived as a numerically and substantively relevant problem in the past 7 years, possibly due to the fact that we have been increasingly working with the autostimulation described above, i.e., the automatic activation of a 60‑s additional impulse in the VNS generator in the event of an abrupt increase in heart rate. Cardiac accelerations of this kind occur during sleep not only in the context of ictal tachycardia, but also, for example, by arousals or autonomic alarm reactions in sleep-related respiratory disorders. Thus, a chain of events consisting of apnea—heart rate increase—VNS autostimulation (with a duration of 60 s) can then lead to a further now longer and stronger apnea, which, if this happens frequently, can drastically worsen possibly pre-existing sleep apnea (for incidence, see above), with the aforementioned consequences in the epileptological–somnological vicious cycle (see Fig. 1).
Sleep apnea is a disease-aggravating risk factor in patients with epilepsy, as shown, e.g., in a polysomnographic study of older epilepsy patients: The subgroups with poor vs. good response to antiseizure medication differed mainly with respect to the presence or degree of comorbid SAS [4].
Therefore, if on the one hand VNS can trigger or worsen sleep apnea and on the other hand sleep apnea is an epilepsy-worsening risk factor, the physician (and patient!) may find themselves facing a therapeutic dilemma: The goal of VNS therapy in difficult-to-treat epilepsy is to improve the seizure situation and not to worsen it.
Arousals and increased vigilance under VNSInduction of respiratory disturbances is not the only mechanism by which VNS therapy can lead to sleep fragmentation. In recent years, we have been able to objectively identify an increased occurrence of arousals in VNS-ON in some patients in polysomnographic monitoring diagnostics without prior VNS-related respiratory disturbance.
It is possible that here VNS stimulation has a direct cerebral arousal effect. The vagus nerve has direct projections to the reticular formation, via the nucleus of the solitary tract to the ventrolateral preoptic thalamus and via the parabrachial nucleus to the locus coeruleus and dorsal raphe nuclei and, thus, to regions functionally related to mood and sleep–wake regulation. The VNS could trigger direct stimulation of noradrenergic and dopaminergic systems in the pons and midbrain, resulting in increases in arousal and vigilance, respectively [12].
Supporting evidence for neuroanatomical hypotheses of this kind was found in animal models using behavioral observation, invasive EEG [15], multiunit recordings, calcium imaging [5], immunohistochemical studies [1], and functional MRI [3], with signs of stimulation-correlated VNS activation of the locus coeruleus, cholinergic and noradrenergic subcortical efferents, dopaminergic substantia nigra, and dopaminergic ventral tegmentum.
Such arousal induction by VNS could explain the VNS-associated movement times during sleep described by Hallböök in 2005 in a group of 15 children, as well as the prolongation of multiple daytime sleep latencies in patients with VNS at an output current < 1.5 mA measured by Malow in 2001 [12, 22].
During the day, an arousal effect by VNS (or equally by DBS) could be highly positive for patients with epilepsy: Vigilance could improve, psychomotor tempo could accelerate, with supportive effects on cognitive skills. It could possibly also shorten postictal loss of consciousness or somnolence, potentially reducing the risk of sudden unexpected death in epilepsy. These are all effects that have already been described in the literature based on empirical observations of patients undergoing VNS therapy, and for which an explanation could be found here.
However, if such an induction of arousal and vigilance occurs during the night, this has negative consequences for sleep continuity and quality. Sleep fragmentation thus induced can—as can the induction of SAS—lead to the somnological–epileptological vicious cycle described above and thus, as consequence, to an exacerbation of seizures and worsening of vigilance and quality of life: The desired effect of VNS would thus be antagonized. Therefore, we find ourselves in the same therapeutic dilemma as we have already found in patients with ANT-DBS (see section on ANT-DBS [35]).
Management of VNS-induced sleep disordersAs a solution, our Hamburg center started to perform a day/night bilevel therapy for patients with VNS-induced sleep disorders in 2016, similar to the procedure for our patients with sleep fragmentation under DBS. A therapy concept of this kind is facilitated and made feasible by a generator model that has been available since 2017 and which allows for the programming of two different therapy programs: With output current, ON-time, OFF-time, pulse width and signal frequency, all parameters can now be set specifically for the time of day; the times at which the generator automatically switches between the day and night program are programmed according to the patient’s lifestyle.
During the day, we employ the commonly used parameters with, e.g., output current of 1.5–1.75 mA, pulse width of 250 μs, frequency of 20 Hz, and 30 s ON-time for the normal mode stimulus and 60 s ON-time for autostimulation. At bedtime, the program switches to a weaker “night program” with reduced “output current”, e.g., 0.625 mA, 0.75, or 1 mA for “normal mode” and autostimulation, and only 30 s ON-time for autostimulation. This information is based on our own clinical experience at our center; multicenter studies or recommendations are not yet available. Under such a day/night bilevel therapy, we often see good clinical effects on mood, daytime vigilance, and also with regard to better seizure control. A worsening of the seizure situation after switching from standard VNS therapy to (at night more weakly dosed) bilevel therapy has not occurred in any of our patients to date.
In patients with VNS generator models without the possibility of day–night conversion, VNS-induced sleep disturbances could be mitigated by lowering the general output current to values < 1.5 mA or/and by reducing the ON time to 21 s for the normal-mode stimulus and 30 s for autostimulation: 21‑s apnea has considerably less clinical relevance than 30‑s apnea. The pulse width should be limited to 250 μs and the signal frequency to 20 Hz.
Indication for nocturnal modification of VNS therapyNocturnal reduction of VNS therapy intensity is by no means indicated in all VNS patients. Rather, this should be discussed (with reference to the lack of evidence from any later multicenter studies to date) with those patients in whom there is already clinical suspicion (or polysomnographic evidence) of a VNS-induced sleep disorder, as well as initially, before initiation of VNS therapy, in patients with SAS, in order to avoid worsening.
Comments (0)