
記住我
Aortic stenosis (AS) is one of the most common type S of acquired valvular heart disease, with increased incidence with age progression as 3%‘9% of adults over 75 years of age develop AS.1–3
Transcatheter aortic valve implantation (TAVI) has been developed and is becoming an attractive alternative to conventional surgical (SAVR) treatment for patients with severe AS.4,5 The two most widely used TAVI systems are the Edwards SAPIEN with a balloon-expandable bio prosthesis and the CoreValve System with a self-expandable bio prosthesis.6
TAVI is considered a safe and effective minimally invasive treatment modality in elderly patients who are not eligible for surgery or who are carrying an unacceptably high perioperative risk for surgical treatment.7–10TAVI is associated with prompt postprocedural recovery and allows for early ambulation in comparison with conventional surgery.11 The superiority of TAVI compared to SAVR has been recently established by the PARTNER Trial and preliminary randomized data confirmed that TAVI compared to SAVR are similar regarding postproce-dural outcomes and mortality, and is becoming a safe and effective treatment option.12
Permanent pacemaker implantation (PPI) and heart conduction disturbances are the most common complications of TAVI. Several predictors of PPI after TAVI have been consistently identified. Mortality has not been increased in patients undergoing surgical aortic valve replacement (SAVR) or trans-catheter aortic valve implantation that required a PPI. Some physicians may advocate that this complication does not increase mortality and is “part of the procedure.”13,14
The validation of clinical benefits of transfemoral TAVI vs SAVR still requires further investigational studies to be adopted as treatment of choice in patients with severe aortic stenosis. The aim of this study was to evaluate early postprocedural outcome results in patients with symptomatic AS and treated with TAVI (transfemoral access), or SAVR.
2. Patients and methodsOur study was a prospective cohort study which included 60 patients diagnosed with severe aortic valve stenosis admitted to the National Heart Institute, Cairo, Egypt from the period of April 2018 to April 2020 to undergo aortic valve replacement.
An interdisciplinary team of cardiac surgeons and interven-tional cardiologists reviewed all cases and formed a consensus on treatment selection (TAVI vs SAVR) based on following criteria.
2.1. Inclusion criteria for aortic valve replacement (a) Patients > 65years. (b) Diagnosis of Severe aortic stenosis based on conventional echocardiography with:Aortic valve area <1 cm2. Mean gradient >40mmHg. Peak gradient >65 mmHg. Peak velocity >4m/s. 2.2. Inclusion criteria for TAVI procedure Aortic valve area <1 cm2 measured by conventional echocardiography. Mean gradient >40mmHg measured by conventional echocardiography. Peak gradient >65mmHg measured by conventional echocardiography. Peak velocity >4m/s measured by conventional echocardiography. Aortic valve annulus diameters from 20 to 26 mm measured by multi-slice CT in TAVI Population. Diameter of ascending aorta 3 cm above the annulus maximum 45 mm measured by multi-slice CT in TAVI Population. Diameter of iliac and femoral arteries above 7 mm measured by multi-slice CT in TAVI population 2.3. Exclusion criteria for aortic valve replacement (a) Prior pacemaker implantation. (b) Prior Cardiac resynchronization therapy (CRT). (c) Implantable cardioverter defibrillators. (ICD) (d) “Valve in a valve” procedures for prior failed surgical bio prosthesis. (e) Prior SAVR. (f) Concomitant aortic root replacement procedures. 2.4. Exclusion criteria for TAVI procedure Femoral, iliac, or Aortic disease hampering catheterization. Aortic Aneurysm. Carotid or vertebral arteries obstruction ≥70%. Coagulopathy. Myocardial infarction or cerebrovascular accidents within one month. Tricuspid or mitral valvular insufficiency of sever degree. Left ventricular or atrial thrombus. Atrial fibrillation. Previous aortic valve replacement. Sepsis or active endocarditis. Hypersensitivity or contraindication to any medication used in the study. Previously conduction defects. Congenital Aortic valve. Supra aortic and subaortic stenosis. Concomitant procedure on another valve (eg, mitral or tricuspid valve repair or replacement. Patients who had did transapical TAVI. Aortic Annular diameter < or > 27 mm. Prior surgical aortic replacement. Prior pacemaker. Prior ICD. Prior CRT. Concomitant aortic root replacement procedures. Aortic regurgitation more than mild degree. All patients were subjected to ethical considerations including written informed consent about the type of the study from all patients or their closest relatives. After full assessment, eligibility, and consent patients were assigned consecutively to undergo aortic valve replacement into two main groups if they met the inclusion criteria of our study 2.4.1 Group I: surgical aortic valve replacement groupThis group included 20 patients who underwent aortic valve was replacement by the standard surgical procedure via a median sternotomy.
2.4.2 Group II: transcatheter aortic valve implantation group This group included 40 patients, and was subdivided into two subgroups based on bioprosthetic valve used to replace the aortic valve. Group A: CoreValve (self expandable valve) included 20 patients. The CoreValve Evolute R device (Medtronic) currently available in four device sizes of 23, 26, 29, and 34 mm, allowing the treatment of native valves with a perimeter of 56.5–94.2 mm. Consists of a tricuspid valve obtained from porcine pericardial tissue, mounted and sutured inside a self-expandable nitinol frame Group B: Edwards SAPIEN (balloon expandable valve) subgroup included 20 patients.The Sapien 3 transcatheter heart valve (THV) (Edwards Lifesciences) is the fourth generation in the balloon-expandable Sapien series of devices. It is available in four valve sizes (20, 23, 26, and 29 mm). The Sapien 3 valve is designed with a cobalt-chromium frame, three bovine pericardial tissue leaflets, and a polyethylene terephthalate (PET) skirt at its inflow portion and an outer PET sealing skirt to reduce paravalvular leakage
The primary endpoint was the prevalence of early postoperative clinical complications after trans-catheter aortic valve implantation versus surgical aortic valve replacement and the secondary endpoints were the composite of post procedural inhospital to 6 months all cause mortality and complications
All study population were subjected to written informed consent, detailed medical history, full clinical examination, standard preoperative laboratory, standard chest X-ray, EURO-SCORE II calculation.
Electrocardiogram was recorded preoperatively to detect baseline parameters and exclude conduction disorders, during hospitalization period, 1, 3, and 6 months after hospital discharge to detect any conduction disorders.
Conduction disorders (CD) were defined as the presence of at least one rhythm abnormality including
I, II, III degree AV block, Left bundle branch block (LBBB), Right bundle branch block (RBBB), Left anterior or posterior hemiblock.A transthoracic echocardiogram was performed for all patients, as standard preoperative assessment, followed by postoperatively. It was performed using Siemens cardiovascular ultrasound machine. Echocardiography was used to evaluate the cardiac chambers according the American Society of Echocardi-ography and the European Association of Cardiovascular Imaging, confirm the presence and severity of AS, assess the degree of valve calcification, LV function and wall thickness, and detect the presence of other associated valve disease or aortic pathology. Also postoperative assessment of transvalvular pressure gradient and measurement of valve area were considered in combination with ventricular function, size, and wall thickness.
Multislice Computed tomography was preoperatively done to all patients undergoing TAVI, for scanning and assessment of aortic root, ascending aorta, abdominal aorta, iliac and femoral arteries were performed for patients without contraindications. Also degree of calcifications of Aortic annulus was also assessed.
Coronary angiography was performed preopertaively to all study population using Siemens Hybrid Machine to assess coronaries, additionally TAVI procedure was performed via femoral approach facilitated by Siemens Hybrid machine.
All patients enrolled in our study were continuously assessed perioperatively until hospital discharge, then follow up at 1, 3, and 6 months after discharge where clinical, ECG, and echocardiographic follow up were done, to assess incidence of postprocedural complications, and to evaluate the incidence and timing of perioperative conduction disturbances requiring a new permanent pacemaker implantation.
2.5. Statistical analysisData were analyzed using IBM SPSS 23.0 for windows (SPSS Inc, Chicago, IL) and NCSS 11 for windows (NCSS LCC., Kaysville, UT). Quantitative data were expressed as mean ± standard deviation (SD). Qualitative data were expressed as frequency and percentage.
The following tests were performed to evaluate obtained data, Independent-samples t test of significance was used when comparing between two means. Mann-Whitney U test was used when comparing two means of not normally distributed data. Chi-square (X2) test of significance was used in order to compare proportions between two qualitative parameters. Fisher Exact test is a test of significance that was used in the place of chi square test in 2 by 2 tables, especially in cases of small samples. Probability (P-value):P-value ≤ .05 was considered significant, P-value ≤ .001 was considered as highly significant and P-value >.O5 was considered insignificant.
3. Results 3.1. DemographicsOur study enrolled 60 patients with the diagnosis of severe aortic stenosis assigned to have aortic valve replacement by either SAVR or TAVI.
There were no statistically significant difference between SAVR and TAVI groups regarding general demographic characteristics as age, gender, weight, height, and BMI (Table 1).
Table 1 - Baseline demographic characteristics of SAVR group and TAVI group SAVR group N = 20 Mean ± SD TAVI Group N = 40 Mean ± SD P Age (years) 74.4 ± 4.72 76.2 ± 3.69 .111 Weight (kg) 72.6 ± 5.0 71.98 ± 5.2 .654 Height (cm) 168.8 ± 3.9 167.9 ± 3.8 .414 BMI (kg\m2) 28.4 ± 2.71 26.3 ± 4.51 .06 N % N % P Gender Male 13 65 25 62.5 .809 Female 7 35 15 37.5On preoperative clinical assessment of comorbidities, NYHA class and calculation of EUROSCOREII, Prevalence of diabetes mellitus was significantly higher among TAVI vs SAVR group (67.5% vs 30%, P = .005). There were no statistically significant differences between both study groups as regards other comorbidities such as Smoking, Hypertension, CKD, and COPD. Additionally, there was no significant difference between both groups as regards to preoperative NYHA class assessment (Table 2).
Table 2 - Preprocedural assessment of comorbidities and clinical status in SAVR and TAVI group SAVR group N = 20 N (%) TAVI group N = 40 N (%) χ2t test∗ P Smoking 5 (25%) 9 (22.5%) 0.04 .829 Diabetes mellitus 6 (30%) 27 (67.5%) 7.58 .005 Hypertension 12 (60%) 22 (55%) 0.14 .714 NYHA I 7 (35%) 10 (25%) 0.66 .718 II 6 (30%) 11 (27.5%) 0.04 .839 III 3 (15%) 7 (17.5%) 0.06 .81 IV 5 (25%) 12 (30%) 0.164 .685 Previous cerebrovascular stroke 2 (10%) 3 (7.5%) 0.11 .741 Previous Myocardial Infarction 3 (15%) 4 (10%) 0.324 .57 Previous PCI 1 (5%) 3 (7.5%) 0.133 .714 Peripheral vascular disease 2 (10%) 4 (10%) 0.0 1.0 COPD 2 (10%) 5 (12.5%) 0.081 .776 CKD 9 (45%) 17 (42.5%) 0.033 .854 Mean ± SD Mean ± SD Creatininclearance (ml\min) 91.3 ± 23.3 93.2 ± 22.5 0.301∗ .764 EUROSCORE II (%) 5.6 ± 0.56 10.3 ± 0.43 36.01∗ <.001Our study showed a significant difference between SAVR and TAVI groups in preoperative calculated EUROSCOREII, which was higher in TAVI groups with mean of 10.3% ± 0.4% compared to 5.6% ± 0.56% among SAVR (P< .001) (Table 2).
3.3. Preprocedural echocardiography assessmentPreoperative echocardiographic assessment of study population showed no statistical significant difference between SAVR and TAVI group regarding Left Ventricular Ejection Fraction, Mean aortic pressure gradient, Maximum aortic pressure gradient, and Pulmonary artery pressure. Additionally, there was no significant difference between both groups on assessment of other valvular affection.
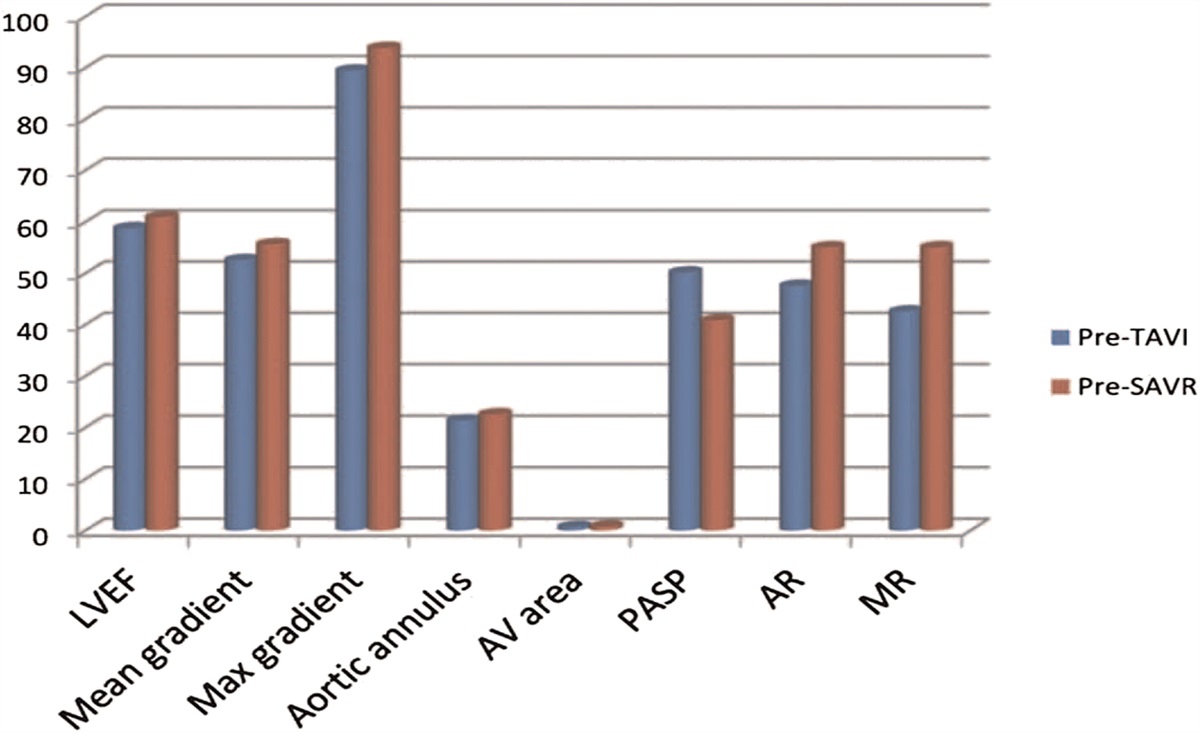
There was a statistically significant difference between both studied groups as regards aortic valve area and Aortic annulus diameter of preprocedural echocardiographic measured parameters, as mean AV area was 0.76 ± 0.21 cm2 in SAVR group vs 0.64 ± 0.14 cm2 in TAVI group, P-value .04, mean aortic annulus diameter was 21.3 ± 1.44 mm in SAVR group vs 20.3 ± 1.35 mm in TAVI group, P-value .002 (Table 3, Fig. 1).
Table 3 - Preprocedural echocardiographic assessment of study groups SAVR group N = 20 Mean ± SD TAVI group N = 40 Mean ± SD t test\MW P LVEF (%) 60.9 ± 9.4 58.7 ± 5.7 0.325 .671 Mean gradient (mmHg) 55.6 ± 15.9 52.6 ± 15.61 0.596 .556 Max gradient (mmHg) 93.8 ± 25.7 89.4 ± 17.5 0.645 .521 Aortic annulus (mm) 22.5 ± 1.44 21.3 ± 1.35 3.17 .002 AV area (cm2) 0.76 ± 0.21 0.64 ± 0.14 2.1 .04 PASP (mmHg) 40.8 ± 23.9 50.1 ± 21.3 1.83 .06 N (%) N (%) Aortic regurgitation 11 (55%) 19 (47.5%) X2 = 0.3 .548 Mitral regurgitation 11 (55%) 17 (42.5%) X2 = 0.837 .36 Figure 1.:
Figure 1.: Difference in preprocedural echocardiographic data between both studied groups.
3.4. Prosthetic valve featuresAll patients in TAVI group underwent the procedure via transfemoral approach representing. A valve size of 23, 25, 27, and 29 mm were used with the following percentage 20%, 20%, 55%, and 5%, respectively in SAVR group. Also a valve size of 23, 26, 29, and 31 mm were used with the following percentage 2.5%, 50%, 45%, and 2.5%, respectively in TAVI group.
In TAVI group 4 types of valves were used; Edwards SAPIEN (10 patients), Edwards SAPIEN XT (10 patients), Medtronic CoreValve (12 patients), and Medtronic CoreValve Evolute R (8 patients) (Table 4).
Table 4 - Prosthetic valve features used in both SAVR group and TAVI group SAVR group N = 20 N (%) TAVI group N = 40 N (%) N (%) Prosthesis size (mm) 23 4 (20%) 1 (2.5%) 25 4 (20%) 0 (0.0%) 26 0 (0.0%) 20 (50%) 27 11 (55%) 0 (0.0%) 29 1 (5%) 18 (45%) 31 0 1 (2.5%) Prosthesis type Mechanical 20 (100%) 0 (0.0%) CoreValve 0 (0.0%) 12 (57.5%) CoreValve evolute 0 8 Edwards SAPIEN 0 10 Edwards SAPIEN XT 0 10Postoperative echocardiographic assessment of study population showed no statistically significant difference between SAVR and TAVI group regarding Left Ventricular Ejection Fraction, Mean aortic pressure gradient, Maximum aortic pressure gradient, and Aotic valve annulus. Additionally, there was no significant difference between both groups on assessment of other valvular affection.
There was a statistically significant difference between both studied groups as regards aortic valve area and Pulmonary artery pressure of postprocedural echocardiographic measured parameters, as Aortic valve area was 2.3 ± 1.21 cm2 in SAVR group VS 1.6 ± 1.11 cm2 in TAVI group, P-value .01. Pulmonary artery pressure diameter was 16.5 ± 8.29mmHg in SAVR group vs 25.1 ± 11.3 mmHg in TAVI group, P value .001 (Table 5, Fig. 2).
Table 5 - Post procedural echocardiography assessment of SAVR group and TAVI group SAVR group N = 20 Mean ± SD TAVI group N = 40 Mean ± SD t test\MW∗ P LVEF (%) 63.5 ± 10.44 61.6 ± 8.17 0.855 .171 Mean gradient (mm Hg) 15.6 ± 10.9 18.3 ± 10.71 1.96∗ .156 Max gradient (mm Hg) 28.8 ± 15.7 29.4 ± 17.5 0.945∗ .721 Aortic annulus (mm) 22.7 ± 1.9 22.9 ± 2.75 0.432 .113 AV area (cm2) 2.3 ± 1.21 1.6 ± 1.11 2.71∗ .01 PASP (mmHg) 25.5 ± 8.29 35.1 ± 11.3 3.37 .001 N (%) N (%) Aortic regurge 4 (20%) 9 (22.5%) X 2 = 0.3 .548 Mitral regurge 3 (15%) 7 (17.5%) X 2 = 0.837 .36 Figure 2.:
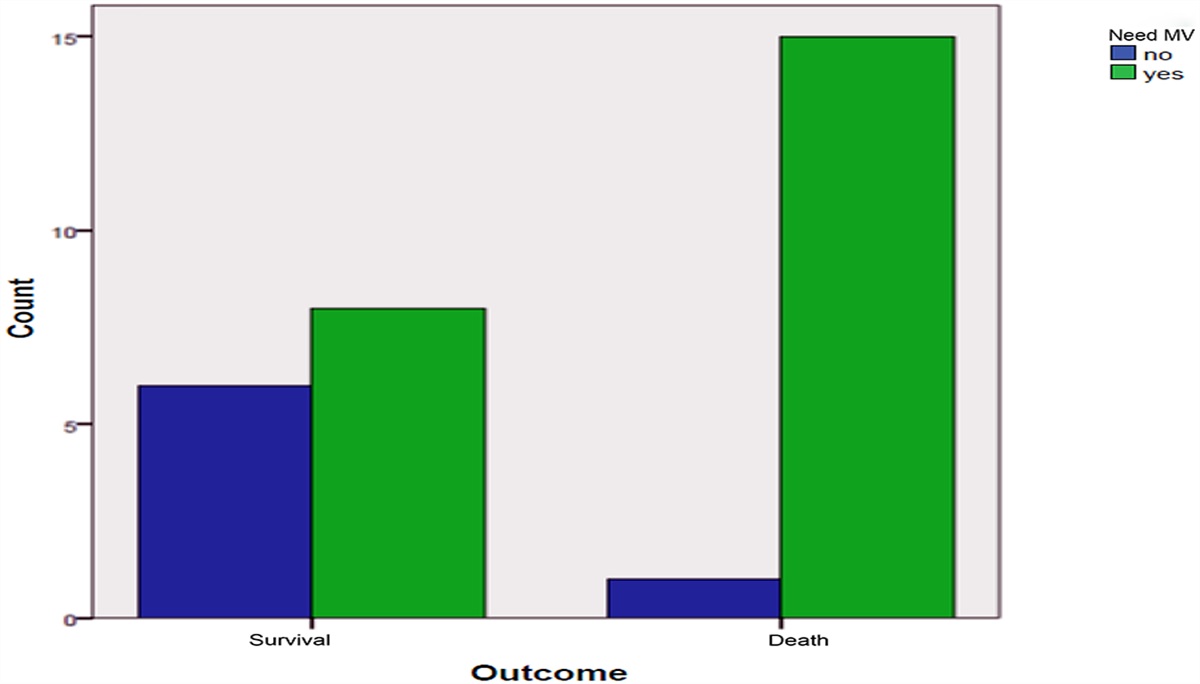
Figure 2.: In hospital complications between SAVR group and TAVI group.
3.6. Postprocedural incidence of conduction defectsOn evaluating all conduction disorders among study population in the early postoperative period, there was a significant increase in incidence among TAVI group compared to SAVR group (20 patients, 50% vs 4 patients, 20%, P-value .03), additionally LBBB was significantly the most common form of conduction disorders among TAVI compared to SAVR group (11 patients, 27.5% vs 1 patient, 5%, P value .04) while there were no significant difference between both groups regarding other types of Conduction disorders. There was no significant difference between both groups as regards requirement of permanent pacemaker implantation (1 patient, 5% in SAVR group vs 3 patients, 7.5% in TAVI group, P value .714 (Table 6).
Table 6 - Comparison between SAVR group and TAVI group as regards incidence of postoperative conduction disturbances SAVR group N = 20 N (%) TAVI group N = 40 N (%) P All CD 4 (20%) 20 (50%) .03 LBBB 1 (5%) 11 (27.5%) .04 LBBB + first degree AVB 1 (5%) 2 (5%) 1.0 RBBB 1 (5%) 1 (2.5%) .611 Complete heart block 1 (5%) 5 (12.5%) .159 Need for PPM implantation 1 (5%) 3 (7.5%) .714LBBB was the most common conduction disorder observed after TAVI (27.5%) followed by CHB (12.5%) and LBBB + first degree AVB (5%).
3.7. Follow up 1 month after hospital dischargeAt 1 month follow up of enrolled patients, we found a statistically significant difference between both groups as regards incidence of all forms of conduction disorders (3 patients, 15% in SAVR group vs 17 patients, 42.5% in TAVI group, P value .03), although LBBB was the commonest type of conduction disorder among both study groups yet there was no statistical significant difference, P-value = .249. While there were non-significant differences between the both groups regarding other types of conduction disorders. Only one patient in TAVI group required Permanent pacemaker implantation (Table 7).
Table 7 - Comparison between SAVR group and TAVI group as regards incidence of conduction disturbances at one month follow up SAVR group N = 20 N (%) N (%) TAVI group N = 40 N (%) N (%) P All CD 3 (15%) 17 (42.5%) .03 LBBB 1 (5%) 9 (22.5%) .09 LBBB + first degree AVB 1 (5%) 3 (7.5%) .311 RBBB 1 (5%) 2 (5%) 1.0 RBBB + first degree AVB 0 (0.0%) 2 (5%) .479 Complete heart block 0 (0.0%) 1 (2.5%) .479 Need for PPI 0 (0.0%) 1 (2.5%) .479At 3-month follow up of enrolled patients, we found no statistically significant difference between both groups as regards incidence of all forms of conduction disturbances (2 patients, 10% in SAVR group vs 8 patients, 20% in TAVI group, P-value .327), although LBBB was the commonest type of conduction disorder among both study groups yet there was no statistical significant difference, P-value = .369 (Table 8).
Table 8 - Comparison between SAVR group and TAVI group as regards incidence of conduction disturbances at three months follow up SAVR group N = 20 N (%) TAVI group N = 40 N (%) P All CD 2 (10%) 8 (20%) .327 LBBB 1 (5%) 5 (12.5%) .369 LBBB+1-AVB 0 (0.0%) 1 (2.5%) .746 RBBB 1 (5%) 1 (2.5%)
留言 (0)