
Remember me
First, I appreciate the efforts of clinicians, who have shown high responsiveness to design various “aerosol boxes,” to prevent health care workers from the infected aerosols during COVID-19 pandemic.
The “aerosol box,” first described by the clinician in Taiwan, for the containment of aerosol generated during airway management of patients with COVID-19, is a cubical transparent box with 2 holes on the clinician's side for airway procedures.1 However, they did not consider the risk to the assistant and other members in the same room and the effect of the aerosol, during and after removal of the aerosol box.
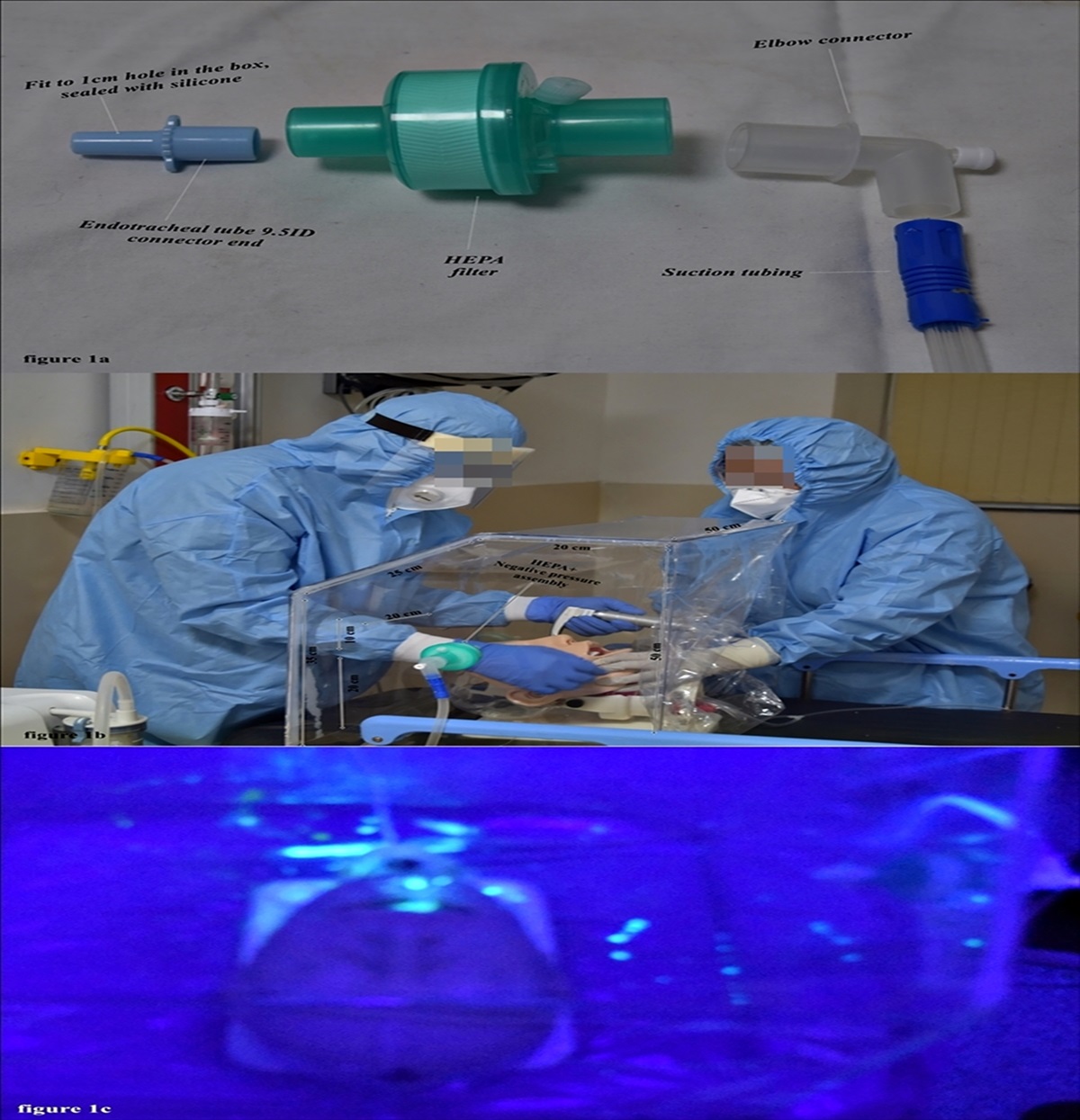
In a short span of time, many modified aerosol boxes were introduced with various modifications.2 Our team also designed a new modified aerosol box with negative pressure and a small HEPA filter with the help of tools easily available in the operating room and ICU (Fig. 1A). This new modified box has inclined upper end on the laryngoscopist side for better visibility and provides a comfortable position while managing the airway with the conventional laryngoscope (Fig. 1B), as most of the time the video laryngoscope is not available. The patient side in this new modified aerosol box can be covered with transparent disposable plastic drape with a slit in the middle, which provides access to the assistant's hand for maneuvering the airway during the intubation.
 Figure 1.:
Figure 1.: (A) HEPA filter and negative pressure suction assembly. (B) New modified aerosol box with measurements. (C) Fluorescent dye spread visualization under UV light.
The size of the cough particle ranges from 0.1 to 100 µm, and at the onset of expiratory effort during the glottis closure, high intrathoracic pressure up to 300 mmHg is generated.3 The airborne spread of aerosol may occur even at a distance of more than 3 m from a patient with respiratory disease. It is quite possible that the cough jet from a patient with respiratory disease contains pathogen and spread airborne diseases.4 This new modified aerosol box has only two holes at the laryngoscopist side with an additional small HEPA filter and negative pressure portable suction, which can produce a flow of 60 L/min and tolerate up to −713 mmHg pressure (Medela Dominant Flex). A wall mount suction port, which can produce a flow of 47.6 L/min, can also be attached to it. Hence, this has a practically lesser risk of spreading aerosol in the operation theater or emergency department outside the new modified aerosol box, even after removal of the aerosol box.
For easy understanding of this new modified aerosol box, a simulation of cough was performed in an airway manikin. For this simulation, the forced fluorescent dye with the help of pressurized air at the pressure of 300 mmHg was pushed through hypopharynx. This simulation showed diversion of droplets more toward the HEPA filter and negative pressure assembly (Fig. 1C, video). Because the cough simulated here is by using a crude method, the projectile direction, turbulence, and size of the droplets cannot be matched with the aerosol generated by the real cough. In addition, this box can be used while performing regional block of head and neck in an awake patient.5 Moreover, this box with a portable suction machine can be used for in-hospital shifting of patients with COVID-19 or other contagious respiratory disease.
References [1]. Canelli R, Connor CW, Gonzalez M, Nozari A, Ortega R. Barrier enclosure during endotracheal intubation. N Engl J Med 2020;382:1957–1958. [2]. Singh B, Singla SL, Gulia P, Kumar A, Bhanwala R. Aerosol containment device for use on suspected COVID-19 patients. Indian J Anaesth 2020;64(suppl 2):154–156. [3]. McCool FD. Global physiology and pathophysiology of cough: ACCP evidence-based clinical practice guidelines. Chest 2006 1;129:48S–53S. [4]. Lee J, Yoo D, Ryu S, et al. Quantity, size distribution, and characteristics of cough-generated aerosol produced by patients with an upper respiratory tract infection. Aerosol and Air Quality Research 2019;19:840–843. [5]. Jaichandran VV, Raman R. Aerosol prevention box for regional anaesthesia for eye surgery in COVID times. Eye (Lond) 2020;34(12):2155–2156
Comments (0)