
記住我
The World Health Organization considers sepsis as a global priority. According to the ACCP/SCCM criteria, sepsis was defined as systemic inflammatory response syndrome (SIRS) and documented infection while sepsis with at least one sign of organ hypoperfusion or malfunction was classified as severe sepsis. Septic shock was defined as severe sepsis plus systemic mean blood pressure <60 mmHg.1 Recently, Sepsis-3 defines sepsis as a life-threatening organ dysfunction caused by an unbalanced host response to infection. It is the main etiology of intensive care unit (ICU) admissions and a leading cause of critical illness and mortality all over the world. It causes more than 5 million deaths annually, with 30% global mortality.2
Sepsis produces complex immunological, coagulation, and circulatory changes that may lead to organ dysfunction and failure known as septic shock.3Sepsis-related coagulopathy may present as mild laboratory alterations up to severe disseminated intravascular coagulation (DIC), which is implicated in microvascular dysfunction leading to organ failure. Moreover, DIC may deplete coagulation factors and platelets, leading to bleeding.4
Septic individuals with severe DIC might present with purpura fulminans or clinically less obvious microvascular fibrin deposition, with multiple organ dysfunction being the most common symptom. Severe bleeding, or even concomitant hemorrhage and thrombosis, could be the primary symptom.5 In patients with severe sepsis, abnormal coagulation, particularly DIC, is an important and independent predictor of clinical prognosis.6
Because sepsis and septic shock are medical emergencies, early detection and treatment, especially among high-risk patients, improves outcomes. As a result, biomarkers that allow for early categorization and identification of patients who are at a higher risk of death are required. The short pentraxin C-reactive protein (CRP) and procalcitonin (PCT), the prehormone of calcitonin, are the 2 most well-studied and used indicators in patients with sepsis. Even so, their ability to distinguish sepsis from other inflammatory diseases or predict outcome is limited. CRP is sensitive but not very specific because it is elevated in all inflammatory illnesses. PCT is better at distinguishing between infectious and noninfectious causes of critical illness than CRP. Despite this, they only provide limited information about the prognosis of severely ill patients.7 According to the current Surviving Sepsis Campaign (SCC) report, PCT can also be used to support decreasing the duration of antimicrobial therapy in patients with sepsis (poor recommendation, low quality of evidence).8 In the first 24 hours of admission, Arora et al. reported no significant relationship between PCT levels and mortality in patients with severe sepsis and septic shock.9 Other markers including vascular endothelial growth factor and presepsin are useful markers for the evaluation of patients with sepsis.10,11
More precise therapy methods and improved patient quality of life would be possible if these clinical syndromes could be recognized and risk-stratified more accurately.12
Pentraxin-3 (PTX3), an acute phase protein, has recently emerged as a promising sepsis biomarker. The typical range for PTX3 is undetectable to 1.5 ng/mL.13 It is a prototype member of the long pentraxin subfamily and a key component of humoral innate immunity. In response to proinflammatory stimuli, PTX3 is expressed in a variety of cells, including dendritic cells and macrophages. It is also found in neutrophil extracellular traps and is saved in neutrophil granules. PTX3 recognizes microorganisms, activates complement, and aids pathogen detection by phagocytes once released, boosting pathogen clearance, adjusting inflammatory responses, and encouraging tissue remodeling.14
Critically ill patients, ranging from SIRS to sepsis and septic shock, have higher levels of PTX3. As a result, it has been investigated as a sepsis prognostic marker. In a comprehensive review and meta-analysis, PTX3 was suggested to be a significant predictor of illness severity and death in sepsis.15
2. Aim of the workBecause the early diagnosis and prognosis of sepsis are still a great challenge, we aimed to evaluate the role of PTX3 in the prediction of clinical outcome and its correlation with coagulopathy in critically ill patients with sepsis.
3. Patients and methodsWe performed a single-center prospective observational study on thirty patients, diagnosed with sepsis, who were admitted to the critical care department in Cairo University Hospitals in Egypt. Each participant or their legal representatives signed a written informed consent form.
All consecutive patients, 18 years or older, were diagnosed with sepsis according to the ACCP/SCCM criteria.1 A Sequential Organ Failure Assessment (SOFA) score is used to characterize each patient with sepsis and the degree of his organ dysfunction.16 The presence of infection can be identified by showing positive clinical manifestation with a positive pathogen culture. Patients with mixed types of shock, long steroid intake, or history of malignancy were excluded from this study. The sepsis-induced coagulopathy (SIC) diagnostic criteria include 3 items: platelet count, international normalized ratio (INR), and SOFA score.17
Age, sex, comorbidities, mean arterial blood pressure (MAP), site of infection, SOFA score (at admission and after 7 days), length of ICU stay, need of mechanical ventilation, and clinical outcome on day 28 were recorded for all participants.
Serum and plasma samples were collected for the different assays (complete blood count, platelet count, coagulation profile) on day 1 and day 7, aiming to study coagulopathy in all the studied patients. Blood samples for PTX3 were collected within 24 hours of the ICU admission and after 7 days and stored at −20˚C until analysis and then measured by using enzyme-linked immunoassay (ELISA). All color reagents were brought to room temperature before using wash buffer, and they were mixed together in equal volumes. The PTX3 standard was reconstituted with deionized or distilled water. All samples, standards, and controls were treated before being added to the microplate. The optical density of each well was determined within 30 minutes using a microplate reader. The duplicate readings for each standard, control, and sample were averaged, and the average zero standard optical density was subtracted. A standard curve was created by reducing the data using computer software capable of generating a log/log curve fit. A standard curve was generated for each set of samples assayed. The minimum detectable dose of human PTX3 ranged from 0.007 to 116 ng/mL. The mean minimum detectable dose was 0.025 ng/mL.
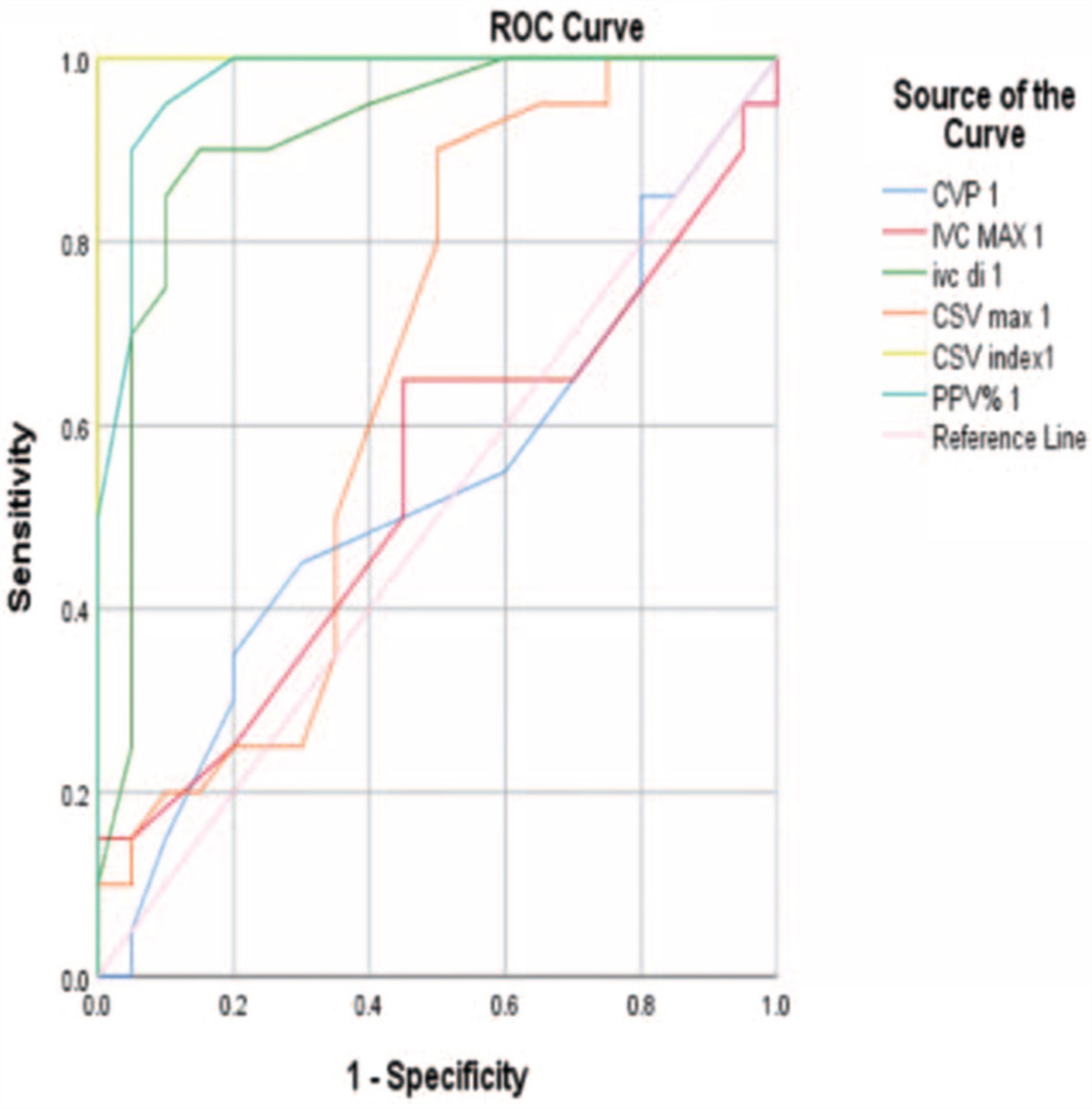
3.1. Statistical analysisData were coded and entered using the statistical package SPSS version 16. Data were summarized using mean, median, and standard of deviation for quantitative variables and numbers and percentages for qualitative values. Comparison between groups was performed using the chi-square test for qualitative variables, the Student t test for quantitative variables when normally distributed, and the Mann-Whitney U test for quantitative data when not normally distributed. Correlations between variables were performed using the Spearman correlation coefficient. The receiver operating characteristic (ROC) curve was constructed with area under curve analysis performed to detect best cutoff value of pentraxin for detection of mortality. The confidence interval was set to 95%, and the margin of error accepted was set to 5%. P values less than or equal to .05 were considered statistically significant.
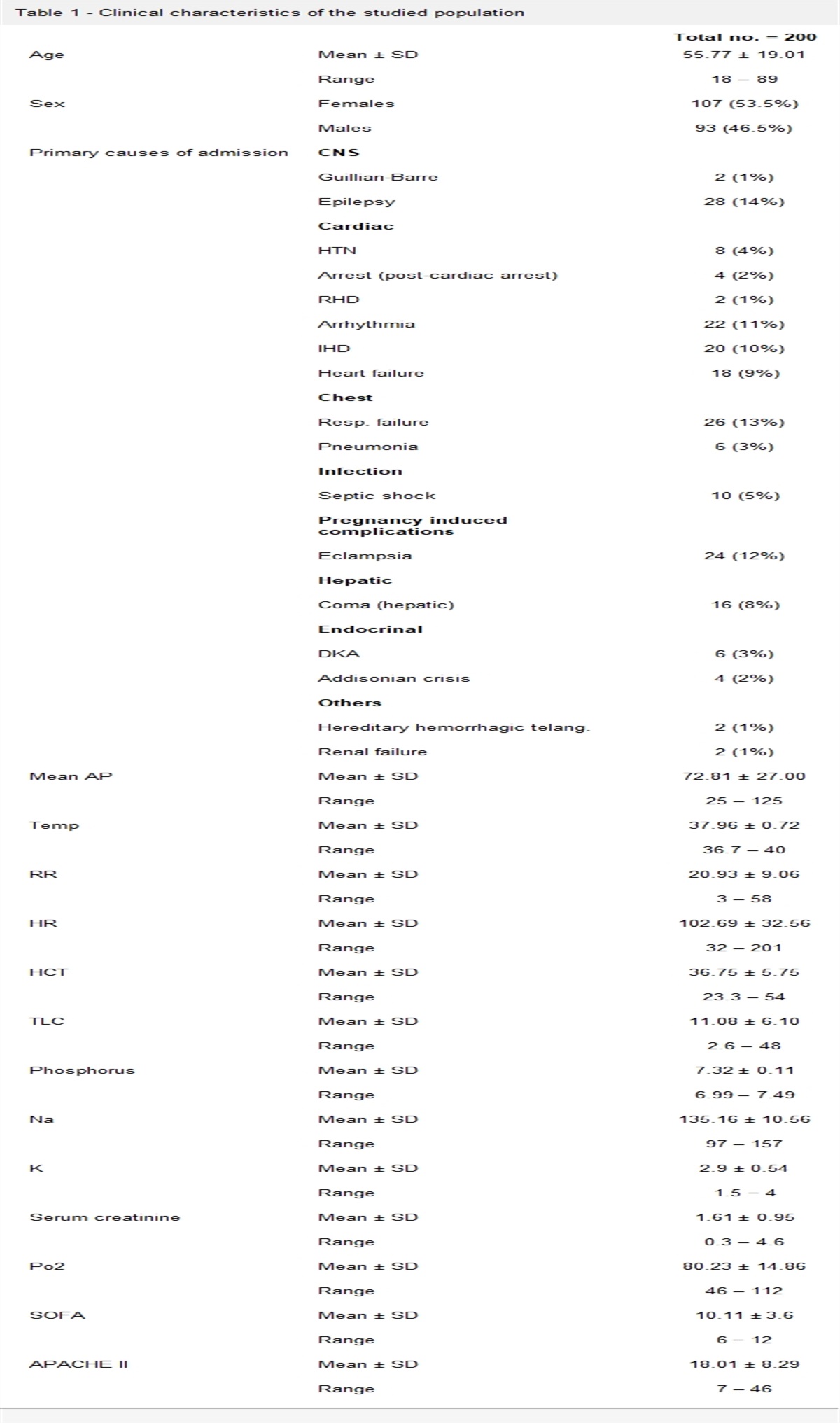
4. Results 4.1. Study populationThirty patients with severe sepsis and septic shock who were admitted to the critical care department of Cairo University Hospitals in Egypt were included in this study (21 male patients and 9 female patients), with a mean age of 64 (±13) years. As regards the source of sepsis, chest infection was the source of sepsis in 54% of patients, bed sores (20%), urinary tract infection (13%), surgical wound infection (6.5%), and central nervous system infections (6.5%).
On studying all groups of patients on day 1 of ICU admission, the MAP, SOFA score, platelet count, and PTX3 level were 73.2 mmHg (±6.12), 7.3 (±2.9), 253.77/µL (±124.1), and 5.98 ng/mL (±2.16), respectively, while on day 7, they were 79.99 mmHg (±10.9), 7.23 ± (4.68), 218.77/µL (±104.1), and 7.4 ng/mL (±4.08), respectively (Table 1).
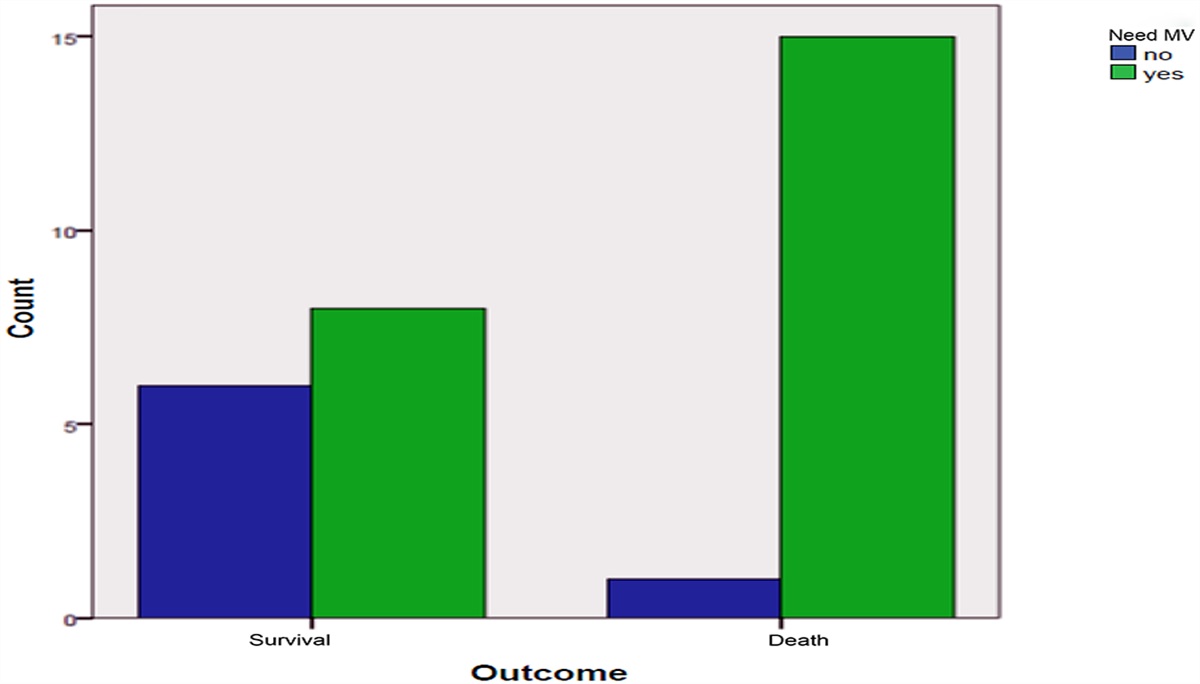
Table 1 - Demographic and clinical parameters in all-cases group Parameter All cases (Mean ± SD) Age (years) 64.27 ± 13.3 Sex, N (%) Male 21 (70%) Female 9 (30%) MAP Day 1 73.27 ± 6.125 Day 7 79.97 ± 10.92 SOFA score Day 1 7.30 ± 2.902 Day 7 7.23± 4.681 SAPS II 46.17 ± 15.812 Mechanical ventilation, N (%) Yes 23 (77%) No 7 (23%) Overt bleeding, N (%) Yes 14 (47%) No 16 (53%) Mortality, N (%) Nonsurvivors 16 (53%) Survivors 14 (47%) PLAT Day 1 253.77 ± 124.108 Day 7 218.77 ± 104.152 PTX3 Day 1 5.9867 ± 2.16 Day 7 7.4033 ± 4.08We divided the patients according to mortality into 2 groups: survivors (14 patients) and nonsurvivors (16 patients), with an ICU mortality of 53%. Nonsurvivors were more critical than survivors, indicated by a significantly higher SOFA score on day 7 (10.7 ± 2.2 vs. 3.3 ± 2) and a higher requirement for mechanical ventilation (93.8% vs. 57.1%) (Figure 1) (Table 2). We found no statistically significant relation between mortality and the source of infection, MAP, or platelet count.
 Figure 1.:
Figure 1.: Number of patients with and without the need for mechanical ventilation in each group (survivors and nonsurvivors).
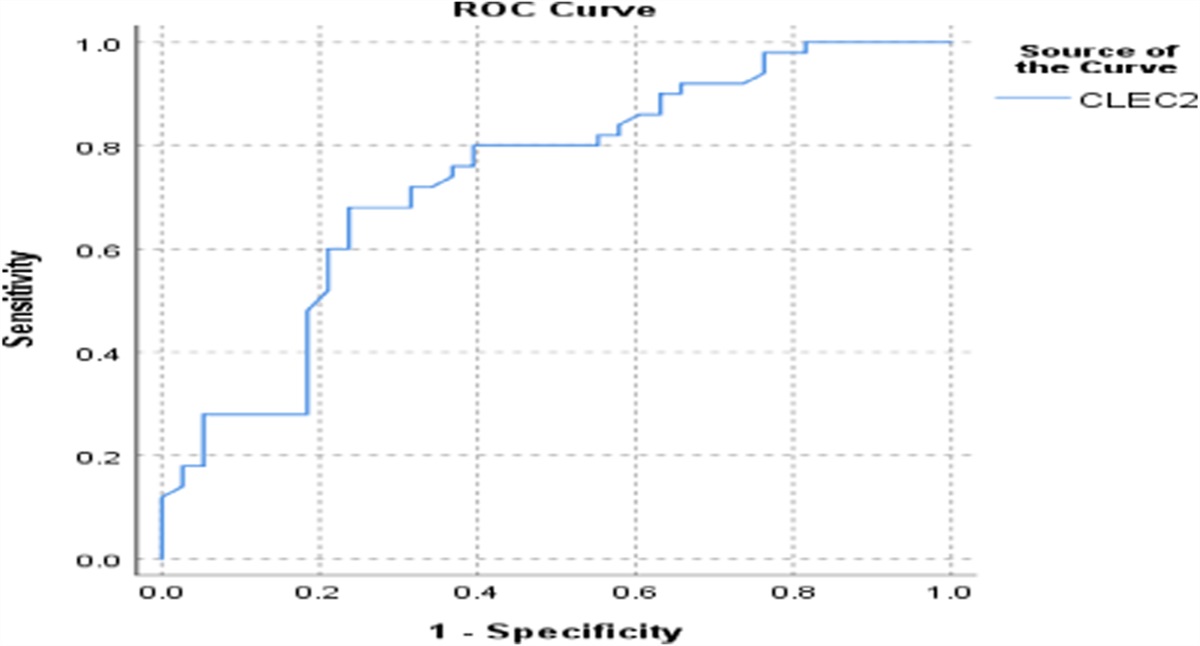
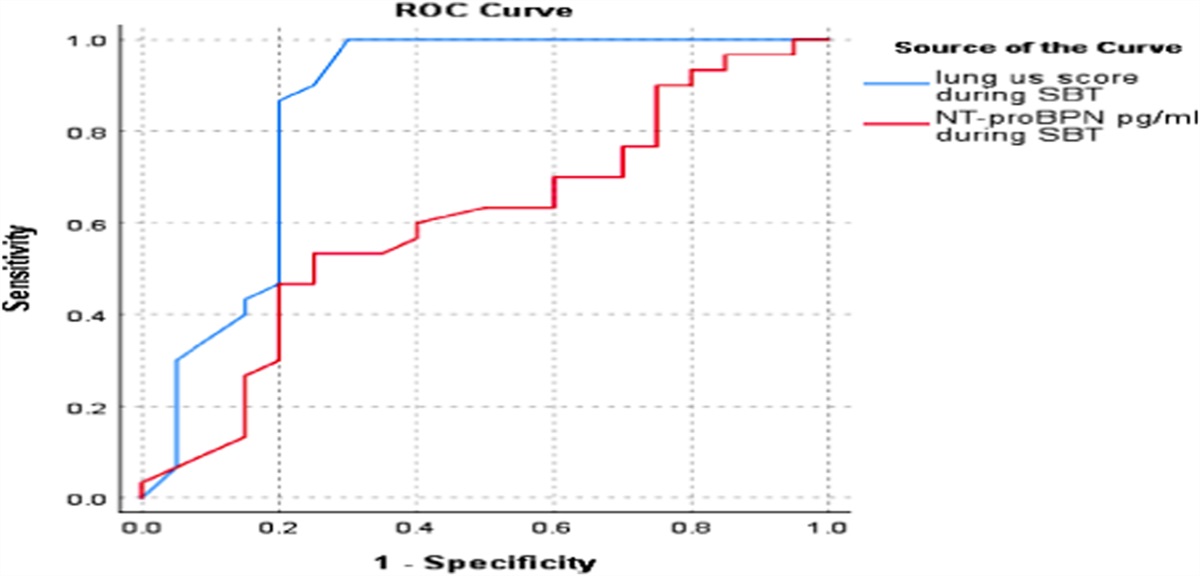
Table 2 - Mean SOFA score, MAP, and platelet count on D1 and D7 in survivors and nonsurvivors (mean [± standard deviation]) Parameters Survival (n = 14) Nonsurvival (no = 16) P Mean ± standard deviation SOFA D1 6.2 ± 2.7 8.3 ± 2.8 .07 SOFA D7 3.3 ± 3.5 10.7 ± 2.2 <.01 MAP D1 74.5 ± 7.8 71.9 ± 3 0.22 .22 MAP D7 81.3 ± 8.4 81.2 ± 16.4 .17 PLAT D1 192.6 ± 54.8 307.3 ± 143.7 .15 PLAT D7 241.5 ± 53.2 173.2 ± 117.9 .42On studying PTX3 level on day 1, there was no statistically significant relation between PTX3 level and mortality, although it was higher than normal in both groups (6.2 ± 1.7 ng/mL in survivors vs. 5.8 ± 2.5 ng/mL in nonsurvivors). On day 7, PTX3 levels were significantly higher in nonsurvivors than in survivors (11.8 ± 3 ng/mL vs. 4.2 ± 1.7 ng/mL, respectively) (Table 3). Furthermore, on ROC curve analysis, PTX3 on the first day was not a predictor for mortality (AUC = 0.348; P value .144) (Figure 2). On day 7, PTX3 was a significant predictor of mortality with 100% sensitivity and specificity with a cutoff level >6.95 ng/mL (AUC = 1.00; P value <.001) (Figure 3).
Table 3 - Mean PTX3 levels in survivors and nonsurvivors PTX 3 in day 1 and 7 Survivor (No = 14) Nonsurvivors (No = 16) P Mean ± standard deviation PTX3 D1 6.2 ± 1.7 5.8 ± 2.5 .17 PTX3 D7 4.2 ± 1.7 11.8 ± 3 .01 Figure 2.:
Figure 2.: ROC curve of PTX3 on day 1 in all patients.
 Figure 3.:
Figure 3.: ROC curve of PTX3 on day 7 in all patients.
For more optimum results, we studied the relationship between rising PTX3 levels and mortality. All nonsurvivors had rising levels of PTX3 in contrast to only 21.4% of survivors, and this was highly significant (Figure 4). A ROC curve was established to assess the relation between delta change of PTX3 from day 1 to day 7 and mortality. Delta PTX3 on day 7 was a significant predictor of mortality with 100% sensitivity and 91.7% specificity with a cutoff value >1.7 ng/mL (AUC = 0.992; P value <.001) (Figure 5). This highlights the importance of the rising level of PTX3 as a prognostic marker and its relation to mortality.
 Figure 4.:
Figure 4.: Number of patients with and without rising PTX3 in each group (survivors and nonsurvivors).
 Figure 5.:
Figure 5.: ROC curve of delta PTX3 on day 7 in all patients.
An interesting point of our study was the relation between PTX3 level and coagulopathy. First, we studied the relation between PTX3 and platelet count; there was negative correlation between PTX3 change and platelet count change (r = −0.7), which was statistically significant (P = .0003) (Figure 6). On studying the relation between PTX3 level and INR as a marker of coagulopathy, we found a positive correlation between change of PTX3 and INR (r = +0.7), which was statistically significant (P = .0007) (Figure 7).
 Figure 6.:
Figure 6.: Correlation between PTX3 level change and platelet count change in all patients.
 Figure 7.:
Figure 7.: Correlation between PTX3 level change and INR change in all patients.
On studying the relation between PTX3 level and coagulopathy, an important point was the incidence of bleeding. Fourteen of our patients got overt bleeding: one was from the survival group and the rest were from the nonsurvival group. On day 7, patients with overt bleeding had significantly higher PTX3 levels than patients without bleeding (11.4 ng/mL ± 3.2 vs. 5.7 ng/mL ±3), but there was no significant relationship on day 1. Furthermore, all the 14 patients who got overt bleeding had rising levels of PTX3 in comparison with only 31.2% of patients without overt bleeding (Tables 4 and 5).
Table 4 - Mean PTX3 levels on day 1 and day 7 in groups of patients with and without overt bleeding PTX 3 in day 1 and 7 No overt bleeding Overt bleeding P Mean ± standard deviation PTX3 D1 6.1 ± 1.5 5.8 ± 2.8 .211 PTX3 D7 5.7 ± 3.7 11.4 ± 3.2 .005Sepsis has been known as a major cause of morbidity in the ICU. Its mortality is associated with the severity of sepsis and the degree of organ dysfunction.18 Many severity scores, such as SOFA, SAPSII, and APACHE II, as well as biomarkers such as CRP and PCT, were used to investigate the outcome in patients with sepsis. However, they have limited information on sepsis prognosis. In contrast to CRP, the prototypic long pentraxin PTX3 is produced early by various cell types, including macrophages, myeloid dendritic cells, and endothelial cells, in response to inflammatory signals such as interleukin-1 and tumor necrosis factor-α. PTX3 is, moreover, stored in specific granules of neutrophils and then released in response to microbial recognition.19
In our study, we tried to evaluate the prognostic value of PTX3 in thirty critically ill patients who were admitted to the ICU because of sepsis, defined according to ACCP definitions.16 To achieve this goal, we divided the patients according to mortality into 2 groups: survivors (47%) and nonsurvivors (53%).
As expected, nonsurvivors were more critical than survivors, which is indicated by a significantly higher SOFA score on day 7 and a higher requirement for mechanical ventilation.
Our main finding was that PTX3 could be a promising predictor of patient outcome. Severe sepsis was associated with high PTX3 levels on day 7 because it was significantly higher in nonsurvivors than in survivors. Furthermore, on ROC curve analysis on day 7, PTX3 was a significant predictor of mortality with 100% sensitivity and specificity with a cutoff level >6.95 ng/mL. However, there was no statistically significant relationship between PTX3 level and mortality in day 1 although PTX 3 level was higher than normal in both groups of patients. In addition, on ROC curve analysis, PTX3 on the first day was not a significant predictor for mortality.
It was noticed that all nonsurvivors had a rising level of PTX3 from day 1 to day 7 in comparison with only 19% of survivors. Delta PTX3 change on day 7 was a significant predictor of mortality in ROC curve analysis with 100% sensitivity and 91.7% specificity with a cutoff value >1.7 ng/mL. This highlights the importance of the rising level of PTX3 as a potential marker of patient outcome.
Our findings go with what was mentioned by Mauri et al. who reported that, although high PTX3 levels in the first 5 days after sepsis onset were linked to a worse outcome, the initial PTX3 levels on ICU admission did not differ between survivors and nonsurvivors.20 Furthermore, Caironi et al. discovered that plasma PTX3 concentrations were greater in nonsurvivors compared with survivors on day 1 and were connected with severity in a large multicenter randomized controlled experiment. While PTX3 levels on day 7 had a significant predictive value for 90-day death, PTX3 level on day 1 was not linked with 90-day mortality after adjusting for all variables in patients with severe sepsis or septic shock.21 In addition, a study conducted by Huttunen R. et al. found a high correlation between high levels of PTX3 from day 1 to day 4 with mortality.22
By contrast, Perez-Martin et al.23 suggested a prognostic value of a single determination of plasma PTX3 level on day 1 of admission as an early predictor of in-hospital 28-day mortality in patients with septic shock, defined according to the latest Sepsis-3 criteria. These contradictory results could be related to the heterogeneity of the different studies with different individuals. Both our study and that of Mauri and Caironi were designed with patients with severe sepsis and septic shock according to the first ACCP definition of sepsis based on the concept of SIRS. Patients were also randomized at the time of enrollment. Perez-Martin et al., on the other hand, studied a group of patients who all fit the new definition of septic shock. Furthermore, the date of the mortality analyses differed (90-day mortality vs. 28-day in-hospital mortality). In addition, there is a difference in the timing and frequency of PTX3 analysis because Perez-Martin et al. measured it once on the day of admission, whereas in our study, we did follow PTX3 on day 1 and day 7, giving us the chance to discover the significant relationship between rising levels of PTX3 and bad outcomes.
Because coagulopathy is considered an independent predictor of clinical outcome in patients with severe sepsis, we investigated PTX3 in relation to coagulopathy by observing the occurrence of bleeding, platelet count, INR, and SOFA score. We realized a consistent association between PTX3 levels and the incidence of bleeding; PTX3 levels were significantly higher in patients with overt bleeding than in patients without bleeding on day 7. Furthermore, all the patients with overt bleeding had a rising level of PTX3 from day 1 to day 7 in comparison with 31% in patients without overt bleeding. We found a significant negative correlation between PTX3 change and platelet count. In addition, PTX3 levels were positively correlated with INR values, which was statistically significant.
Our data coincide with that published by Mauri et al.,20 who found a good correlation between PTX3 and sepsis-associated coagulopathy investigated by plasminogen activator inhibitor 1, whereas Raija Uusitalo-Seppälä et al. found weak correlation between PTX3 level and platelet count. The difference in strength of correlation between our study and that of Raija may be explained by the category of studied patients because they studied patients with suspected infection at emergency room, and it may also be related to the medications used in ICU during treatment of patients with sepsis.24
In view of the heterogenous and unpredictable responses of the immune system to infection, a single parameter may not be enough to predict the outcome of sepsis. We hereby highlight the need to involve PTX3 in clinical scoring systems with other biomarkers, which would strengthen each other with more accurate mortality prediction.
6. ConclusionOur study supports the benefit of PTX3 analysis in predicting outcome in patients with sepsis. Both the detection of a high PTX3 level on day 7 of admission and the recognition of its rising level during the hospital stay are associated with disastrous outcomes and a higher incidence of bleeding. Our findings strongly recommend using PTX3 and including it in different scoring systems of sepsis severity that may guide therapy and put intervention plans.
6.1. LimitationIt was beyond the scope of our study to compare different biomarkers predicting morbidity and mortality in patients with sepsis. Further studies with a larger number of patients are needed to reach agreement on the exact timing of testing of PTX3 and search for a clear cutoff value. Another limitation is that this study is a single-center study, so multicenter studies according to new sepsis definitions are suggested to unveil the importance of this unique biomarker in predicting sepsis outcome.
References [1]. Calandra T, Cohen J. The international sepsis forum consensus conference on definitions of infection in the intensive care unit. Crit Care Med 2005;33:1538–1548. [2]. Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med 2016;193:259–272. [3]. Angus DC, Wax RS. Epidemiology of sepsis: An update. Crit Care Med 2001;29: S109–S116. [4]. Levi M. Current understanding of disseminated intravascular coagulation. Br J Haematol 2004;124:567–576. [5]. Zeverleder S, Hack CE, Willemin WA. Disseminated intravascular coagulation in sepsis. Chest 2005;128:2864–2875. [6]. Levi M, de Jonge E, van der Poll T. Plasma and plasma components in the management of disseminated intravascular coagulation. Best Pract Res Clin Haematol 2006;19:127–142. [7]. van Engelen TSR, Wiersinga WJ, Scicluna BP, et al. Biomarkers in sepsis. Crit Care Clin 2018;34:139–152. [8]. Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med 2017;43:304–377. [9]. Arora S, Singh P, Singh PM, et al. Procalcitonin levels in survivors and nonsurvivors of sepsis: Systematic review and meta-analysis. Shock 2015;43:212–221. [10]. El-Akabawy H, Abo Hamela M, Gaber A, Abozekry A. Prognostic value of vascular endothelial growth factor in sepsis syndrome. Egypt J Crit Care Med. 2016;4:119-126. [11]. El-Shafie M, Taema Kh, El-Hallag M, et al. Role of presepsin compared to C-reactive protein in sepsis diagnosis and prognostication. Egypt J Crit Care Med. 2017;5:1-12. [12]. Coopersmith M, De Backer D, Deutschman C, et al. Surviving Sepsis Campaign: Research priorities for sepsis and septic shock. Intensive Care Med 2018;44:1400–1426. [13]. Fazzini F, Peri G, Doni A, et al. PTX3 in small vessel vasculitides: an independent indicator of disease activity produced at sites of inflammation. Arthritis Rheum 2001;44:2841–2850. [14]. Mantovani A, Garlanda C, Doni A, Bottazzi B. Pentraxins in innate immunity: From C-reactive protein to the long pentraxin PTX3. J Clin Immunol 2008;28:1–13. [15]. Lee YT, Gong M, Chau A, et al. Pentraxin-3 as a marker of sepsis severity and predictor of mortality outcomes: A systematic review and meta-analysis. J Infect 2018;76:1–10. [16]. Singer M, Deutschman C, Seymour C, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016;315:801–810. [17]. Iba T, Arakawa M, Di Nisio M, et al. Newly proposed sepsis-induced coagulopathy precedes International Society on Thrombosis and Haemostasis Overt-Disseminated Intravascular Coagulation and Predicts High Mortality. J Intensive Care Med. 2020;35:643–649. [18]. Weng L, Zeng X, Yin P, et al. Sepsis-related mortality in China: A descriptive analysis. Intensive Care Med 2018;44:1071–1080. [19]. Camozzi M, Rusnati M, Bugatti A, et al. Identification of an antiangiogenic FGF2-binding site in the N terminus of the soluble pattern recognition receptor PTX3. J Biol Chem 2006;281:22605-22613. [20]. Mauri T, Bellani G, Patroniti N, et al. Persisting high levels of plasma pentraxin 3 over the first days after severe sepsis and septic shock onset are associated with mortality. Intensive Care Med 2010;36:621–629. [21]. Caironi P, Masson S, Mauri T, et al. Pentraxin 3 in patients with severe sepsis or shock: The ALBIOS trial. Eur J Clin Invest 2017;47:73–83. [22]. Huttunen R, Hurme M, Aittoniemi J, Huhtala H, Vuento R, Laine J, et al. (2011) High Plasma Level of Long Pentraxin 3 (PTX3) Is Associated with Fatal Disease in Bacteremic Patients: A Prospective Cohort Study. PLoS One 2011;6:e17653. [23]. Perez-San Martin S, Suberviola B, GarciaUnzueta MT, Lavin BA, Campos S, Santibañez M. Prognostic value of plasma pentraxin 3 levels in patients with septic shock admitted to intensive care. PLoS One 2011;15:e0243849. [24]. Uusitalo-Seppälä R, Huttunen R, Aittoniemi J, et al. Pentraxin 3 (PTX3) is associated with severe sepsis and fatal disease in emergency room patients with suspected infection: A prospective cohort study. PLoS One 2013;8:e53661.
留言 (0)