
記住我
Coronary artery disease (CAD) is considered the major burden of cardiovascular diseases, causing up to 80% of deaths from cardiovascular disease all over the world.1
For patients with acute coronary syndrome (ACS), percutaneous coronary intervention (PCI) was proved to have a prognostic benefit regarding death, myocardial infarction, hospitalization with ACS, and the urgent need for revascularization.2,3 However, similar degree of benefit has not been proven in patients with chronic coronary syndrome (CCS).4,5 Despite this, successful PCI in patients with CCS has been shown to improve symptoms, exercise tolerance, and quality of life (QoL).6
Although the extent of benefit of PCI as an initial strategy in the management of CCS remains debatable, the guidelines recommend an initial approach with optimal medical therapy (OMT) including intensive medical treatment, control of risk factors, and lifestyle modifications as first-line therapy, with PCI reserved for those who remain symptomatic.7 The growing belief that PCI offers more effective symptomatic relief rendered PCI popular and—to a great extent—a routine in the initial management of patients with CCS.
We tried to evaluate the magnitude of benefit of invasive strategy regarding major adverse cardiovascular events, as well as symptomatic relief and its impact on QoL, putting into consideration the placebo effect of PCI, and whether an attempt for an early invasive strategy is deserved, especially when PCI is currently considered a safe procedure with a low complication rate.8
This study was designed to evaluate the midterm (up to 6 months) outcomes of PCI with OMT versus OMT alone in patients with CCS.
2. Patients and methodsThe 2019 ESC guidelines for diagnosis and management of CCS7 defined six most frequently encountered clinical scenarios in patients with suspected or established CCS as follows: (1) patients with suspected CAD and “stable” anginal symptoms and/or dyspnea, (2) patients with new onset of heart failure (HF) or left ventricular dysfunction and suspected CAD, (3) asymptomatic and symptomatic patients with stabilized symptoms 1 year after initial diagnosis or revascularization, (4) patients with angina and suspected vasospastic or microvascular disease, and (5) asymptomatic patients in whom CAD is detected at screening.
2.1. Patient selectionThis study enrolled 210 patients who presented at the outpatient clinic of cardiology department, Faculty of Medicine, University of Alexandria.
2.2. Inclusion criteriaAll patients had a diagnosis of CCS based on objective evidence of ischemia, together with angiographically significant (>70%) lesion(s) involving one or more coronary arteries subtending a large area of myocardium. The objective evidence of ischemia included at least one of the following:
Resting ECG: >1.0 mm ST-segment deviation from the baseline or >2.0 mm T-wave inversion (or pseudonormalization, if T waves were previously inverted) in ≥2 contiguous leads. Treadmill exercise tolerance test: >1.0 mm horizontal or downsloping or ≥2 mm upsloping ST-segment deviation from baseline in ≥2 contiguous leads.9 Nuclear stress (exercise or dipyridamole) SPECT myocardial perfusion imaging: >1 scintigraphic perfusion defects (reversible or partial reversible).10 2-Dimensional stress echocardiography either with exercise (treadmill or bicycle ergometer) or with dobutamine.11 Multislice CT coronary angiography showing significant coronary lesion(s).9 2.3. Exclusion criteria Recent acute coronary syndrome. Coronary anatomy not suitable for PCI: ○ Left main coronary disease >50% with a SYNTAX score >32. ○ Coronary arteries technically unsuitable or hazardous for PCI. ○ Patients with nonsignificant CAD in whom PCI would not be considered appropriate or indicated. Previous coronary artery bypass grafting (CABG). EF < 30% (<35% if patient has 3-vessel disease including >70% LAD proximal stenosis). Concomitant valvular heart disease likely to require surgery or affect prognosis during follow-up. Severe noncardiovascular comorbidities limiting survival. 3. MethodsAt the time of coronary angiography, a written informed consent was obtained from all patients that they will be blinded (throughout the study period) to the nature of the procedure and what type of treatment they will receive. One hundred five patients underwent PCI with OMT in accordance with the current guidelines (reference to CCS ESC guidelines7) including dual antiplatelet therapy (PCI group). The other 105 patients were assigned to OMT alone, including a single antiplatelet therapy and a placebo tablet (medical-therapy group) (Tables 1 and 2).
Table 1 - Angiographic characteristics in both groups PCI (n = 105) Medical-therapy (n = 105) P Rt dominance, No. (%) 92 (88) 89 (85) .489 Distribution of involved vs. LAD, No. (%) 79 (75) 81 (77) .801 RCA, No. (%) 50 (48) 50 (48) .98 CX, No. (%) 44 (42) 38 (36) .365 OM1, No. (%) 11 (10) 11 (10) .973 D1, No. (%) 6 (5) 9 (9) .333 RI, No. (%) 1 (1) 3 (3) .411 Involved vs. .994 Single vessel, No. (%) 45 (43) 45 (43) .998 2 vessels, No. (%) 36 (34) 36 (35) ≥3 vessels, No. (%) 24 (23) 23 (22) Serial lesions, No. (%) 34 (32) 33 (31) .878 CTO, No. (%) 26 (25) 23 (22) .687 Calcifications, No. (%) 23 (22) 19 (18) .514 Lesion types .549 A, No. (%) 4 (4) 8 (8) .562 B, No. (%) 54 (51) 52 (49) C, No. (%) 46 (44) 45 (43) Lesions' characteristics Total No. of lesions 180 218 Total occlusion, No. (%) 24 (26) 26 (23) .744 Bifurcating lesion, No. (%) 25 (27) 30 (27) .965 Aorto-ostial lesions, No. (%) 15 (16) 19 (17) .823 Tortuous lesions, No. (%) 4 (4) 5 (5) .933 Eccentric lesions, No. (%) 21 (23) 32 (29) .329 Total lesion length, (mm) Min–max 7–98 5–98 Mean ± SD 34.19 ± 19.91 32.81 ± 19.89 .621 Mean diameter stenosis, (%) Min–max 80–100 70–100 Mean ± SD 90.82 ± 6.44 60.20 ± 6.67 .507 Calcifications, No. (%) 23 (22) 19 (18) .512 Thrombotic lesions, No. (%) 4 (4) 3 (3) .524 Syntax score Min–max 1–29 0–29 Mean ± SD 12.81 ± 7.52 12.42 ± 7.651 .833P, P value for comparing between PCI and medical groups.
*Statistically significant at P ≤ .05.
All patients were followed up at 1-month, 3-month, and 6-month intervals after randomization. The primary end point was major adverse cardiac events (MACE) including death, myocardial infarction, hospitalization for acute coronary syndrome, and the need for urgent revascularization. The secondary end points included the improvement in angina severity as assessed by using the Canadian Cardiovascular Society class12; physical limitation, angina stability, and angina frequency as assessed by using the Seattle Angina Questionnaire (SAQ)13; QoL as assessed by using the EQ-5D-5L questionnaire14 and 6-minute walk test (6MWT).15
3.2. Statistical analysis of dataData were fed to the computer and analyzed using IBM SPSS software package version 20.0 (Armonk, NY: IBM Corp). Qualitative data were described using number and percent. The Kolmogorov-Smirnov test was used to verify the normality of distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation (SD), median, and interquartile range. Significance of the obtained results was judged at the 5% level. The used tests were as follows:
1. Chi-square test: For categorical variables, to compare between different groups. 2. Fisher exact test or Monte Carlo correction.Correction for chi-square when more than 20% of the cells have expected count less than 5.
3. Student t test: For normally distributed quantitative variables, to compare between two studied groups 4. ANOVA with repeated measures: For normally distributed quantitative variables, to compare between more than two periods or stages, and post hoc test (Bonferroni adjusted) for pairwise comparisons. 5. Mann-Whitney U test: For abnormally distributed quantitative variables, to compare between two studied groups. 6. Kruskal-Wallis test: For abnormally distributed quantitative variables, to compare between more than two studied groups, and post hoc (Dunn multiple comparisons test) for pairwise comparisons. 7. Spearman coefficient: To correlate between two distributed abnormally quantitative variables. 4. Results 4.1. Demographic characteristics of the study populationTable 3 provides an overview of demographic characteristics, clinical characteristics, and risk factors of the study population.
Table 3 - Patients' characteristics and risk factors PCI (n = 105) Medical-therapy (n = 105) P Sex Male (%) 67 (64) 61 (58) Female (%) 38 (36) 44 (42) .89 Age (years) Min–Max 39–86 37–92 .26 Mean ± SD 60.92 ± 9.84 59.36 ± 10.29 BMI Min–Max 22.8–36.2 22.8–35.4 .76 Mean ± SD 28.983 ± 3.149 28.854 ± 2.988 Hypertension (%) 68 (65) 65 (62) .67 DM (%) 70 (67) 70 (67) 1 IRDM (%) 53 (50) 50 (48) .784 Dyslipidemia (%) 31 (29) 29 (28) .879 Current smoking (%) 7 (7) 12 (10) .326 Family history of CAD (%) 13 (12) 14 (13) .838 COPD (%) 3 (3) 5 (5) .47 CKD (%) 11 (10) 9 (8) .624 PVD (%) 6 (6) 11 (10) .208 History of MI 4 (4) 4 (4) 1 History of PCI 18 (17) 15 (14) .572BMI, body mass index; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; IRDM, insulin-requiring diabetes mellitus; MI, myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vascular disease; SD, standard deviation.
All patients were complaining of angina class II or III. In the PCI group, 45 patients (43%) presented with angina CCS class II and 60 patients (57%) presented with angina CCS class III, while in the medical-therapy group, 37 patients (35%) presented with angina CCS class II and 68 patients (65%) presented with angina CCS class III. Table 4 shows the list of medications received in both groups. In the PCI group, one patient did not receive aspirin because of allergy.
Table 4 - List of medications received in both groups PCI group (n = 105) Medical-therapy group (n = 105) P Aspirin (%) 104 (99) 105 (100) .318 Plavix (%) 87 (83) 0 (0) .0001 Ticagrelor (%) 18 (17) 0 (0) .0001 High-intensity Statin (%) 105 (100) 105 (100) 1 Beta-blockers (%) 102 (97) 102 (97) 1 Calcium channel blockers (%) 7 (7) 10 (9) .605 ACEi (%) 33 (31) 40 (38) .313 ARBs (%) 36 (34) 32 (30) .557 Antianginals (%) 59 (56) 68 (65) .206ACEi, angiotensin-converting enzyme inhibitors; ARBs, aldosterone receptor blockers; PCI, percutaneous coronary intervention.
The median duration of symptoms before enrollment was 5 months (mean 8.32 ± 2.17 in the PCI group vs 2.98 ± 1.73 in the medical-therapy group). All patients had anginal CCS class II or III (34% of patients had angina class II while 66% had angina class III).
Resting ECG was used for inclusion in 42% of patients, EST in 21%, resting echocardiography in 29%, stress echocardiography in 4%, myocardial perfusion imaging in 4%, and MSCT-CA in 13% of the patients.
The median value of left ventricular ejection fraction was 60 (mean 59.41 % ± 9.16 in the PCI group and 60 ± 8.245 in the medical-therapy group).
4.1.1. Primary outcome (MACE)After 6 months of follow-up, there was no statistically significant difference between PCI and medical-therapy group regarding MACE (Table 5).
Table 5 - Comparison between medical and PCI according to MACE MACE PCI group (n = 105) Medical-therapy group (n = 105) χ2 P No. % No. % Revascularization 3 2.8 4 3.8 0.148 FEP = 1.000 ACS 4 3.8 5 4.8 0.116 FEP = 1.000 MI 0 0.0 1 0.9 1.005 FEP = 1.000 Death – – – – – – Stroke – – – – – – Others 2 1.9 0 0.0 2.019 FEP = .248 Total MACE 7 6.7 7 6.7 0.000 1.000χ2, chi-square test; ACS, acute coronary syndrome; FE, Fisher exact; MACE, major adverse cardiovascular events; MI, myocardial infarction; P, P value for comparing between the studied groups; PCI, percutaneous coronary intervention.
In the PCI group, four patients had unplanned hospital admission with NSTE-ACS (one patient after 2 months, one patient after 4 months, and the remaining two patients after 6 months of the indexed PCI), two of them underwent myocardial revascularization (one patient after 2 months and the other patient after 6 months and had intervention to the target vessel). In addition, one patient underwent myocardial revascularization as an outpatient because of recurrent chest pain. No deaths or cerebrovascular accidents occurred. One female patient had threatening vaginal bleeding; another patient had intracerebral hemorrhage.
In the medical-therapy group, six patients had unplanned hospital admission with NSTE-ACS (one patient with MI after 6 months, one patient with unstable angina after 5 months, and the remaining four patients with unstable angina after 6 months of enrollment). Two of those patients underwent myocardial revascularization: one patient after 5 months and the other patient after 6 months of enrollment. Another patient underwent myocardial revascularization as an outpatient because of worsening chest pain.
4.1.2. Secondary outcomesThe improvement in CCS angina class in the PCI group was significantly higher than the medical-therapy group (P < .001). Forty-eight patients (46%) in the PCI group showed improvement by two or more classes against only two patients in the medical-therapy group (Table 6). In the PCI group, chest pain improved completely after 1 month in six patients (6%) and in 16 more patients after 3 months of follow-up to reach a total of 32 patients (30%) after 6 months of follow-up. However, in the medical-therapy group, chest pain did not resolve completely in any of the patients.
Table 6 - Comparison between PCI and medical-therapy groups according to the increment in CCS from the beginning of enrollment until 6-month follow-up CCS increment PCI group (n = 105) Medical-therapy group (n = 105) χ2 P No. % No. % No change or deterioration 4 4 19 18 59.117* <.001* Improve by one class 53 50 84 80 Improve by two or more classes 48 46 2 2χ2, chi-square test; CCS, chronic coronary syndrome; P, P value for comparing between PCI and medical-therapy groups; PCI, percutaneous coronary intervention.
*Statistically significant at P ≤ .05.
Two cases were not able to perform 6MWT because of severe osteoarthritis, one in each group. In the PCI group, two cases did not complete the test because of unplanned hospital admission due to ACS: one in the second month of follow-up and the other in the fourth month of follow-up. In the medical-therapy group, one case did not perform 6MWT in the sixth month because of unplanned hospital admission in the fifth month of follow-up.
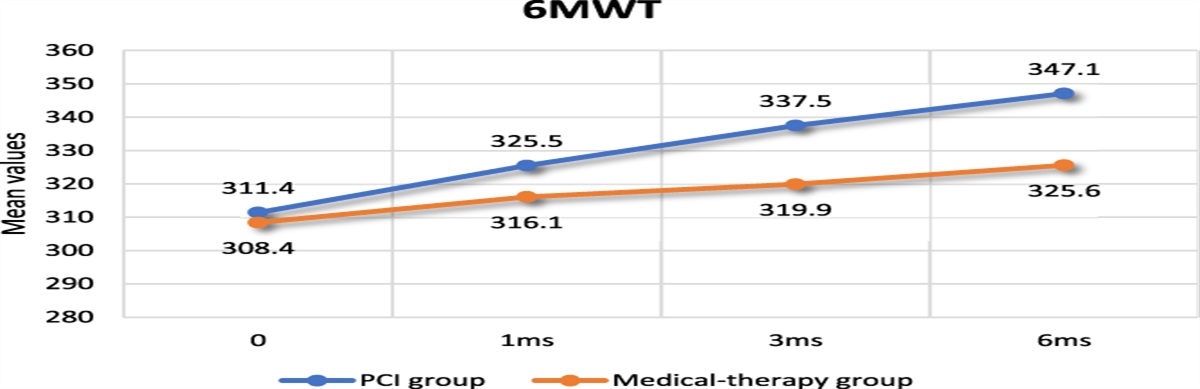
The increment of the distance in 6MWT over 6 months in the two groups was statistically significant although being higher in the PCI group (P < .001), as shown in Figure 1.
 Figure 1.:
Figure 1.: Comparison of the mean values of 6MWT in both groups from the baseline and over 6 months of follow-up.
4.1.4. Seattle Angina QuestionnaireTwo cases in the PCI group and one case in the medical-therapy group did not complete the 6-month follow-up score because of ACS and unplanned hospital admissions.
The improvement in physical limitation, angina frequency, and angina stability (assessed by SAQ score) and the improvement in QoL (assessed by using the EQ-5D-5L score) over 6 months in the two groups were statistically significant and higher in the PCI group (P < .001 for each), as shown in Figure 2.
 Figure 2.:
Figure 2.: Comparison of the mean values of SAQ physical limitation, angina frequency, and angina stability and EQ-5D-5L in both groups from the start of enrollment till 6 months of follow-up.
All the three elements of SAQ showed that the most significant improvement was after the first month of PCI; the mean values increased after 1 month from the baseline by 3.96 (56.7%) for physical limitation, by 1.08 (65%) for angina frequency, and by 1.99 (63.8%) for angina stability. The same was also noted for the EQ-5D-5L score; the mean value increased by 0.18 after the first month (69.2%), which is more than 69% of the total increment in the score over 6 months of follow-up.
4.1.5. The additional effect of supervised aerobic exercise to medical treatmentSeven patients from the medical-therapy group underwent an aerobic exercise supervised by a cardiologist. Regarding the comparison between the rest of the medical-therapy group and the subgroup of patients who underwent a supervised aerobic exercise, the improvement in 6MWT was higher in this subgroup but without statistical significance (P = .714). The improvement in angina frequency as assessed by using SAQ was significantly higher in this subgroup (P = .001). However, there was no significant difference between both groups regarding the remaining items of SAQ or the QoL as assessed by using the EQ-5D-5L score after 6 months of follow-up.
On the other hand, there was a statistically significant improvement in favor of the PCI group in physical limitation, angina stability as assessed by using SAQ, and QoL as assessed by using the EQ-5D-5L score after 6 months of follow-up (P = .008, .011, and .004, respectively).
5. DiscussionOur study highlighted the lack of a significant prognostic value of PCI over medical therapy in patients with CCS, despite the observed significant improvement in symptoms and QoL. The current guidelines of the management of CCSs recommend an initial approach with OMT, including intensive medical therapy, a reduction of risk factors, and lifestyle intervention as first-line therapy, followed by PCI in the second-line management, especially for those patients who remain symptomatic.7
In this study, PCI-based initial management strategy using drug-eluting stents (DES) did not prove to reduce the primary end point compared with a strategy of OMT in patients with CCS.
The RITA-2 trial16 showed that using PTCA for the treatment of patients with angina resulted in higher rates of all-cause mortality or MI as compared with those who were treated medically. This was explained later by the periprocedural and postprocedural complications and more frequent repeat coronary angiographies of patients who were managed with PTCA. On the other hand, Bucher et al17 had conducted a systematic review of six randomized controlled trials comparing PTCA with medical therapy in nonacute CAD. They found that PTCA might be associated with better improvement in angina, lower rates of MI, death, and the need for repeated revascularization than medical treatment (P < .001). The same results were observed among older patients (75 years or older) with chronic angina by the TIME investigators.18
The COURAGE trial19 included 2287 patients with objective evidence of myocardial ischemia and significant CAD randomized to PCI with OMT versus OMT alone. During a median follow-up of 4.6 years, they found no significant difference between both groups regarding death from any cause and nonfatal myocardial infarction (19% vs. 18.5%, P = .62). However, in a COURAGE substudy, angioplasty provided better outcomes in patients with large ischemic burden assessed by using a stress test with nuclear imaging than the medical-therapy group.20 In addition, the medical-therapy group showed a higher rate of additional revascularization because of unresponsiveness to maximized medications or worsening of ischemia than the PCI group, although they used bare-metal stents (32.6% compared with 21.1% HR, 0.60; 95% CI, 0.51 to 0.71; P < .001).
Hueb et al21 in the MASS II trial assigned 611 patients with stable angina and multivessel CAD to undergo CABG, PCI, or medical treatment. At 5 years of follow-up, there was no statistical difference in the incidence of composite events (death, MI, or need for repeated revascularization because of refractory angina) between PCI using bare-metal stents and medical treatment (RR, 0.93; 95% CI, 0.67 to 1.30). However, the need for repeated revascularization with BMS was higher than the medical therapy group (11.2% vs. 9.4%, P = .021). Even after longer period of follow-up reaching 10 years,22 the death rate remained comparable although the rate of MI was significantly higher with medical therapy (20.7 vs. 13.3%; P < .01) and the rate of repeated revascularization was high in the PCI and the medical-therapy group (41.9% and 39.4%, respectively).
After a median follow-up of 3.3 years in the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, Maron et al23 found no significant statistical difference between the routine-invasive and conservative strategies regarding the primary end point, cardiovascular death, MI, hospitalization for unstable angina, HF, or resuscitated cardiac arrest (P = .34). The conservative strategy showed higher incidence of hospitalization for unstable angina (P = .02) while the invasive strategy showed a higher rate of hospitalization for HF (P < .01).
All these studies had confirmed that PCI, as an initial management strategy, did not reduce the risk of death, MI, or other MACEs when added to OMT. This similarity of event rates between both lines of management could be explained by the fact that probability of future events is always associated with vulnerable plaques (plaques at risk of becoming unstable, rupturing, and inciting thrombosis), rather than stable plaques associated with stable CAD. Lesions that are responsible for death, acute events, and MI are usually not severe enough to induce ischemia on stress testing. On the other hand, lesions causing ischemia usually do not tend to rupture.
The enrollment of patients in previous studies, like our study, was based on angiographic findings, with or without noninvasive documentation of ischemia.
However, when FFR was used
留言 (0)