
記住我






Anthropology integrates complementary perspectives to comprehensively examine the historical and contemporary forces that shape human society, behavior, and biology. This holistic approach is helpful in identifying important biocultural determinants of well-being. Incorporating anthropological perspectives into tropical medicine research can consequently provide important frameworks for understanding disease progression and long-term health patterns. For example, embodiment theory considers how human bodies are shaped by lived experiences, physically transforming in response to social and environmental interactions [1, 2]. Incorporating embodiment theory into infectious disease research provides a framework to assess the ways that lived experiences translate into biological realities. Here, we argue that an understudied area of embodiment theory is how environmental interactions associated with sociopolitical and economic circumstances (i.e., inequality, marginalization, segregation, resource access, infrastructure quality) alter exposure to important microbes and pathogens—including those responsible for tropical diseases—with lasting implications for immune system development, function, and long-term health outcomes.
The importance of embodiment in shaping human health has been increasingly recognized and discussed in the field of biological anthropology [3,4,5], but additional work is needed to clarify how these pathways contribute to variation in immune system development and the emergence of enduring health and social inequities. In this article, we present an overview of the embodiment concept, briefly exploring the pathways by which embodiment may occur, focusing specifically on environmental correlates to pathogen exposure and resulting changes in immune function. We then present an anthropological case study on the immune-related embodiment of environmental conditions (e.g., exposure to neglected tropical diseases) using preliminary data from the Rural Embodiment and Community Health (REACH; REACHresearch.org) study, a project investigating how health inequities and systemic racism may shape long-term well-being in the USA.
Embodiment OverviewEmbodiment is central to the study of human well-being and the emergence of health inequities. As first outlined by social epidemiologist Nancy Krieger, embodiment reflects an “ecosocial” theory of disease causation, recognizing that humans are both cultural and biological beings and considering how external interactions and exposures become internalized through physiological and developmental pathways to ultimately alter individual health [1, 2]. Central to the concept of embodiment is a focus on local ecology, necessitating examination of dynamic interactions between organisms sharing a particular ecosystem [6, 7], with implications for key health determinants (e.g., resource acquisition, disease exposure, experienced psychosocial stress) and associated downstream health inequities. Overall, an embodiment framework encourages researchers not to assume physical differences between individuals or populations are innate, but to instead consider how these differences may be shaped by dynamic variation in social and environmental contexts across the life course [1].
While embodiment research can be used to help explain positive health patterns [2], it has been more commonly used to document how poor health outcomes are shaped by patterns of power (e.g., constrained agency due to structural inequalities), production, consumption, and reproduction [5, 6, 8, 9]. For instance, increased exposure to pathogens, chronic psychosocial stress, and unequal access to resources are all outcomes known to influence long-term health patterns that have been linked with low socioeconomic status, institutional and interpersonal discrimination (e.g., racism, sexism, ageism, homophobia), and infrastructural neglect [4, 10,11,12]. Because sociocultural factors and lifestyle patterns impact individual interactions with the environment and subsequent exposure to microbes and pathogens, researchers using biocultural approaches are well suited to explore the process and consequences of embodiment. Relevant biocultural methodologies include interview data, biomarker and anthropometric measures, and epigenetic/metagenomic sequencing. Anthropological research across a variety of settings has demonstrated how biomarker analyses may capture hard to quantify aspects of lived experiences, such as chronic stress (i.e., through repeat measures of cortisol levels) and associated health patterns [5, 13], as well as links between structural lifestyle changes, exposure to important microorganisms (e.g., intestinal parasites and microbes that influence gut microbiota composition), and immune function [14,15,16,17]. As evidenced by these select studies, a biocultural toolkit is well suited to synthesize and connect lived experiences with downstream physiological effects, thus documenting how both large-scale structural forces and local-level realities shape the process of embodiment [8].
Overarching Pathways of EmbodimentContinued methodological refinements have allowed researchers to more definitively demonstrate the specific mechanisms by which lived experiences become embodied, including recent work drawing on epigenetic, microbiome, and immune function measures. Here we discuss these embodiment pathways in more detail, with special focus on pathogen exposure and immune system development and function (Fig. 1).
Fig. 1
Pathways and effects of embodied immunity. Solid black lines represent direct effects of disease exposure (linked with resource access and living conditions) and immune activity. Gray checked lines represent factors that alter energy availability, thereby shaping immune system development and function. Green rectangles are the social, political, and environmental factors that become embodied. Blue ovals are the immediate downstream effects of those environmental factors. Orange rounded rectangles represent measurable embodied outcomes. These embodied effects can occur in previous generations (purple box) and affect children (red box) through intrauterine environments, inherited living conditions, and epigenetic changes. While the measurable embodied outcomes are separated here, it is important to recognize that all three discussed here affect one another. Figure created with Microsoft PowerPoint
EpigeneticsThe field of epigenetics provides quantifiable insights into the mechanisms by which environmental conditions can produce embodied phenotypes. Epigenetic research measures environmentally sensitive DNA modifications that impact gene expression—including chemical modifications to DNA and DNA-associated proteins (i.e., histones) —but do not change an individual’s underlying DNA sequence [18, 19]. These epigenetic modifications are functionally important because they affect which genes are expressed. Epigenetic measures are useful in embodiment research because, unlike DNA bases which are typically fixed across the lifespan, epigenetic modifications are sensitive to environmental exposures (e.g., nutrition, psychosocial stress, and toxins). A large body of research has focused on documenting links between environmental conditions and epigenetic modifications during early development [19, 20]. Furthermore, there is increasing evidence that the environmental experiences of prior generations may influence epigenetic patterns in descendants [21], which provides a biological basis for the embodiment of historical trauma [19, 22, 23].
Gut Microbiome MeasuresThe composition and activity of the gut microbiome—defined as the collective genome of the 100 trillion bacteria and other microbes residing in the intestinal tract—is also influenced by individual living conditions and local environment, including diet, household infrastructure, and healthcare access/medication history [17, 24]. The gut microbiome is established early in life and is influenced by a range of factors [19], including delivery method at birth [25,26,27,28], post-birth feeding method (i.e., breast vs. formula feeding) [29], and antibiotic use [30,31,32,33]. Importantly, each of these factors is shaped by resource access (e.g., to quality medical care and parental leave to support breastfeeding) and living conditions (e.g., exposure to microbes linked with unhealthy gut microbiota development), thereby providing a biological pathway by which embodiment may occur and shape long-term health outcomes.
The development of the microbiome during early development influences health outcomes throughout the life course and across generations [26, 27, 34]. Like epigenetic modification, pathological gut microbiome profiles can negatively affect the gestational environment and may therefore contribute to the intergenerational transmission of poor health [24]. Microbiome composition also appears to shape immune system and digestive tract development. A healthy and diverse microbiome protects against certain pathogens and supports digestive processes (e.g., vitamin synthesis and fiber break down), while a microbiome experiencing dysbiosis (i.e., an imbalance of beneficial/pathogenic species) can potentially lead to pathological states such as hyperinflammation [26, 27, 34]. Early microbiome-linked immune effects may in turn alter the risk of developing health inequity-related chronic conditions. For example, racial disparities in gastrointestinal health are evident in the USA, with Black adults exhibiting elevated rates of certain gastrointestinal cancers (e.g., stomach, small intestinal, and colorectal cancer) and higher resulting mortality rates than white adults [35, 36]. This pattern has been attributed in part to higher hyperinflammatory immune responses elicited by exposure to pathogenic bacteria or parasites, but also due to gut microbiota dysbiosis [15, 36,37,38]. Child environmental exposure and related microbiome development may consequently play a key role in the emergence of health disparities later in life.
Immune System Development and FunctionRecent work has started to consider links between embodiment pathways and infectious disease patterns [15, 24, 39, 40], highlighting clear connections between embodiment pathways and infectious disease risk that should be explored further [15, 39]. For instance, the Eukaryotic Microbiome (i.e., the collective genome of non-bacterial members of the intestinal microbiome that includes fungal, protozoal, and helminthic species) is an area of microbiome research that has received surprisingly little attention but may have important implications for embodiment processes and immune function [41]. Interactions with these microorganisms during development have been implicated in shaping long-lasting immune activity and subsequent long-term health outcomes.
The Old Friends Hypothesis, for example, contends that a specific branch of the immune system (i.e., type 2 immunity), evolved in response to macroparasite infection [42,43,44]. Relatively recent changes in sanitation infrastructure, hygiene practices, and medical care limit exposure to these “old friends,” potentially resulting in immune dysregulation that favors pro-inflammatory pathways and causes the body to overreact to harmless or self-produced stimuli. These immune changes ultimately increase the risk of chronic inflammatory diseases (e.g., allergies, autoimmune diseases, cardiovascular disease) and are hypothesized to contribute to the relatively high prevalence of these conditions in high-resource, low pathogen areas [42, 45]. Still, while pathogen exposure during key developmental periods may produce enhanced immune regulation in later life, the immune responses elicited by contracting parasitic infections and other tropical diseases are also energetically expensive and may result in delayed growth and cognitive development, as well as other negative health outcomes [46,47,48]. Thus, by shaping long-term immune function and developmental outcomes, environmental exposures to pathogens and associated immune responses demonstrate how the embodiment of early life experiences (e.g., parasite load) may alter adult well-being (e.g., immune profiles, adult height, educational attainment).
Problematically, previous studies investigating links between infection-related changes in lasting immune function have largely been conducted in higher-resource areas (i.e., testing factors linked with allergies and asthma risk in these populations) [49,50,51,52]. Additional research is therefore needed to assess the embodiment of infectious disease exposure in low-resource, marginalized groups, particularly low-resource areas facing high tropical disease risk. Given that these communities are often characterized by harmful environmental exposures (e.g., pathogens and pollutants), widespread poverty, and high levels of psychosocial stress that may negatively impact immune function [4, 10,11,12], embodiment likely contributes substantially to health outcomes. Yet, few studies have conceptualized these health outcomes using embodiment theory to understand lasting immune impacts associated with living in a high-pathogen environment, especially during key developmental periods. Biocultural anthropological frameworks and methods are well suited to address this need. Here, we provide a preliminary case study that demonstrates the application of an anthropological embodiment framework to investigate how living conditions, resource access, and pathogenic exposures during development may interact to influence immune system development.
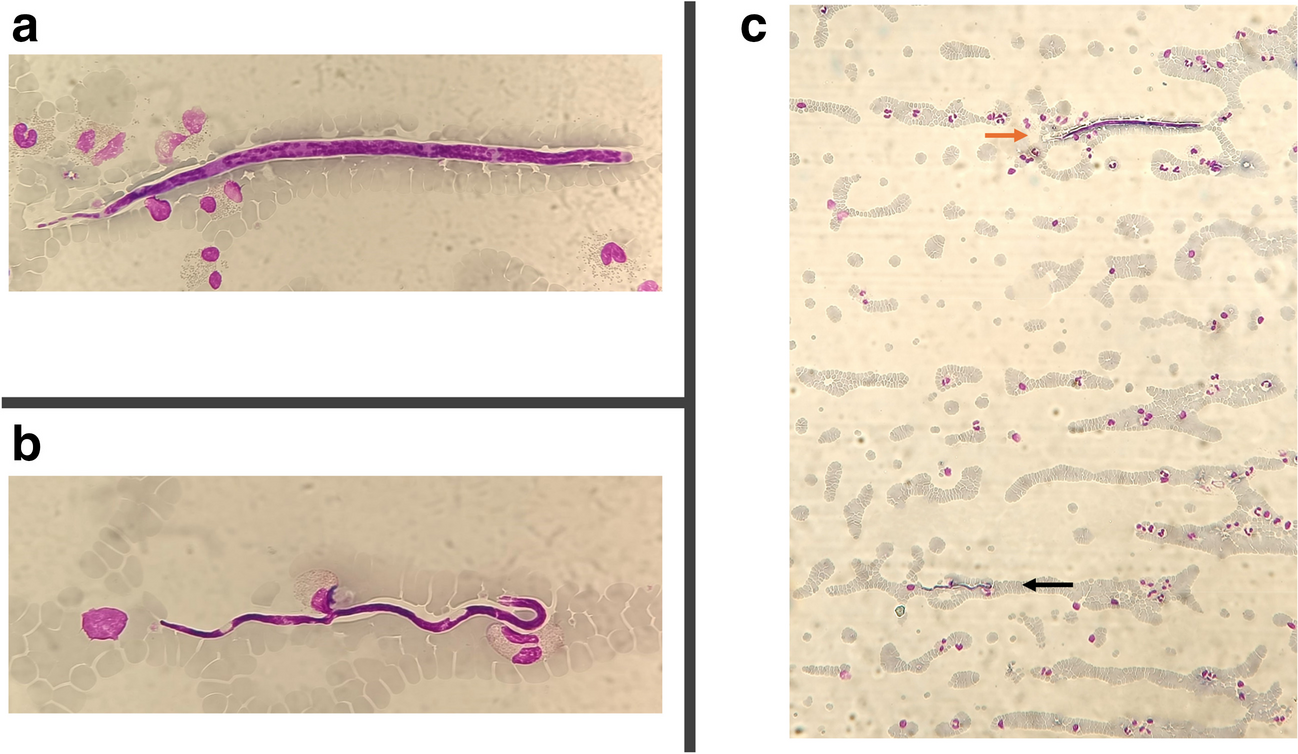
Embodiment Case Study: the Rural Embodiment and Community Health (REACH) StudyThe Rural Embodiment and Community Health (REACH; https://www.reachresearch.org/) study was established in 2019 with the goal of investigating the prevalence of neglected tropical diseases and relationships between lifestyle variation, ecological factors, and health patterns in low-income rural regions of the USA through the lens of embodiment. The project focuses on the impact of exposure to intestinal parasites (e.g., protozoal and helminth infections) and pathogenic bacteria (e.g., Helicobacter pylori) on growth, development, and immune function. The long-term consequences of these infections can include malnutrition, iron deficiency, stunted growth, and delayed cognitive development for intestinal parasites [53], and possible intestinal inflammation and increased gastrointestinal cancer risk later in life for H. pylori [36]. However, infection symptoms vary substantially across populations and individuals, likely due to variation in both physiology and embodied experiences. Embodiment processes linked with exposure to parasites and other gastrointestinal pathogens remain poorly studied in the USA; it is therefore unclear how these types of environmental exposures may be embodied and contribute to prevalent health disparities evident among minoritized and low-resource communities within this high-income country [15, 54,55,56,57].
Moreover, the burden posed by gastrointestinal parasites in the USA is currently unknown due to limited research interest, medical testing, and national attention; however, historical data from the 1930s through 1980s suggest endemic levels of infection [55, 57,58,59,60,61,62]. The elimination of parasites has never been conclusively demonstrated, and there is good reason to believe that infections continue to be prevalent, especially in the Southern USA where high poverty rates and environmental factors (e.g., soil conditions and climate) favor infection spread [55, 63]. The hypothesis that parasite infection may still be prevalent in the USA has been gaining traction in recent years [15, 54,55,56,57]. Recent evidence from studies conducted in the Southern USA indicates that several types of parasitic infections are present, including protozoa (i.e., single-celled eukaryotes) and helminths (i.e., parasitic worms) [15, 54,55,56,57].
Thus, parasite infection may represent an underexplored set of lived experiences in the USA that alter individual biology and contribute to the development of long-term health inequities and associated socioeconomic disparities. As has been demonstrated in lower-income countries, the long-term effects of infection-related embodiment may be especially impactful during childhood when the immune system is developing, leading to context-dependent lasting immune effects [46, 64]. Immune challenges during early life have been shown to affect long-term immune cell production patterns, with implications for lifelong immune function and later health outcomes. Measuring specific immune marker concentrations can consequently provide important information on immune system development, status, and exposure histories. For instance, the antibody immunoglobulin E (IgE) is critical in adaptive immune responses to macroparasites. Likewise, exposure to other pathogens, like viruses and bacteria, may elicit acute, inflammatory immune responses to clear the infections (e.g., the production of C-reactive protein [CRP]) and longer lasting humoral immune activity (e.g., immunoglobulin G [IgG]) [65,66,67,
留言 (0)