1. IntroductionmRNA vaccines have been implemented worldwide following the outbreak of the coronavirus disease (COVID-19) pandemic. A two-dose regimen of the BNT162b2 vaccine by Pfizer-BioNTech confers 95% protection against COVID-19 [
1]. In Japan, public vaccination began in February 2021, and according to the Ministry of Health, Labour, and Welfare of Japan, 79% of the total population (100 million people) had received two vaccine doses by February 2022. Furthermore, 50% of the total population received a third dose in May 2022. In addition to group vaccinations in public spaces, primary-care physicians administered individual vaccinations in Japan.One major issue following the mRNA vaccination for COVID-19 concerns the vaccine’s ability to confer long-term immunity. Several reports have provided evidence that indicates the antibody titers increase dramatically following the administration of two doses of the mRNA vaccine; however, these titers then decrease rapidly [
2,
3,
4,
5]. As the antibody titers decrease, so does the clinical effectiveness of the vaccination [
6]. Thus, repeated booster vaccinations within a short interval are crucial to prevent disease and community spread.Another issue with regard to the COVID-19 vaccination concerns interindividual differences in vaccine immunity. Even in a healthy population, the range of antibody titers after vaccination is widely distributed. Some factors, such as male sex or alcohol consumption habits, may influence interindividual differences [
7]. In certain groups, such as older adults and those with autoimmune diseases or cancer, some individuals have reportedly shown an inadequate immune response to the COVID-19 vaccination and were poor responders [
7,
8,
9,
10,
11,
12,
13].Detection systems for anti-SARS-CoV-2 spike receptor-binding domain (RBD) antibodies are readily available in the Japanese healthcare system. The chemiluminescent enzyme immunoassay (CLIA) produced by Abbott Laboratories is one such system used worldwide. Nevertheless, data on the normal range of the antibody titers for the SARS-CoV-2 spike RBD after two doses of the COVID-19 vaccination in healthy Japanese individuals are limited. A high antibody titer has been shown to correlate with solid immunity against COVID-19 [
6], although antibody production reflects only a part of the vaccine immunity.
This study aimed to assess the monthly mean antibody titer in Japanese adults aged <65 years after the second dose of BNT162b2. Through converting antibody titers into a mean titer percentage in relation to Japanese individuals aged <65 years, we compared the antibody titers between different groups, such as older adults or patients with an autoimmune disease, regardless of the time of the titer determination after the second dose.
2. Materials and Methods 2.1. Study Design
This single-center prospective study, conducted in Izumo City, Shimane Prefecture, Japan, involved individuals and patients who had received SARS-CoV2-mRNA vaccinations with Pfizer-BioNTech BNT162b2 (first and second doses) from April to October 2021 at medical clinics and public spaces. During this period, approximately 3000 vaccinations were administered to 1500 outpatients and healthy individuals residing in the vicinity of the Sugiura Clinic.
Blood samples for antibody testing were collected four times: on the day of the second vaccination (one dose), 2–3 weeks after the second dose (peak), 3 months after the second dose, and 6 months after the second dose of vaccination. Individuals who underwent at least two blood collections at a different time, other than the four previously mentioned time points, were included in the study. Information on all of the participants was collected, including medical information, smoking and alcohol consumption habits, and side-effects of vaccination, such as fever and total IgG serum levels. The study was approved by the Ethics Committee of MEDIKS (Sapporo, Japan) with approval no. MX-4150FN-151448 and the Shimane University Institutional Committee of Ethics (Shimane, Japan) with approval no. 4913. Written informed consent was obtained from all participants.
2.2. Participants
Inclusion criteria comprised volunteers aged 20–65 years who had received a BNT162b2 vaccination at the Sugiura Clinic from 14 September to 31 October 2021 and who provided written informed consent to participate in this study. Those with a history of COVID-19 or those who had received immunosuppressive therapies were excluded. In total, 81 healthy individuals aged <65 years (39 men, 42 women) were enrolled. The mean age ± standard deviation (SD) was 42.2 ± 11.9 years. We also included 38 individuals (age, >65 years; men, 50%) who attended the Sugiura Clinic with chronic diseases, such as hypertension but excluded those with autoimmune diseases. The mean age ± SD of the older adult group was 78.2 ± 6.0 years, and this group had not received immunosuppressive therapy. Furthermore, 14 patients with systemic lupus erythematosus (SLE) (women, 100%) who attended the Sugiura Clinic and received immunosuppressive treatments were also recruited. All of the patients with SLE were in remission, and the mean SLE disease activity index (SLEDAI) was 1.14 ± 1.45. The mean age ± SD in this group was 42.2 ± 11.9 years, and all of the patients had received a median dose of 5.6 ± 3.0 (range, 1–12) mg/day of oral prednisone. Other standard immunosuppressive treatments included hydroxychloroquine in 11/14 (78.5%) patients and tacrolimus in 10/14 (71.4%) patients. All of the participants, including the volunteers, older adults, and patients with SLE, provided their written informed consent prior to participation in this study.
2.3. Measurement of Antibody Titers
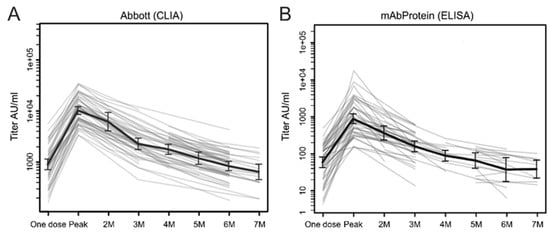
The anti-SARS-CoV-2 spike RBD antibody titers were assessed using two detection systems. The CLIA, from Abbott Laboratories (Chicago, IL, USA), is used worldwide and was obtained under contract by Nihon Rinsho, Inc. (Kyoto, Japan) for commercial antibody testing. This system detects the anti-SARS-CoV-2 spike RBD IgG using an ARCHITECT i2000R analyzer (Abbott Laboratories). The cutoff and upper detection limits were 50 and 80,000 arbitrary units (AUs)/mL, respectively. The second detection system was a sandwich enzyme-linked immunosorbent assay (ELISA) system (E-S-001), newly developed by mAbProtein, Inc. (Izumo City, Shimane, Japan) to detect anti-SARS-CoV-2 spike RBD IgG type antibodies in the serum. The lower detection limit was 0.4 AU/mL, which was determined by adding two standard deviations to the mean optical density (OD) obtained from 50 assays of the zero standard. All the samples in the study were measured using the CLIA (Abbott) and ELISA (mAbProtein) systems, with the antibody titers showing a significant correlation (r = 0.841, p < 0.001, Pearson’s test).
2.4. Kinetic GraphA program using the R language,
https://CRAN.R-project.org/package=AntibodyTiters (accessed on 30 September 2021), enabled us to visualize the raw antibody data at any sampling point in the form of kinetic graphs. At least two blood sampling points are required to generate a kinetic graph. The kinetic charts showed increases and decreases in antibody titers for individuals generally or for different categories of individuals, such as those aged 2.5. Antibody Data Comparison
Following data collection, the monthly mean titers following two doses of BNT162b2 in Japanese individuals aged <65 years were determined. The raw data of antibody titers of older individuals and patients with SLE were changed to percentages relative to the mean titer of the same sampling time as the individuals aged <65 years. At least two blood samples were obtained per person, and the mean percentage was calculated using two or more raw antibody titers. To compare healthy individuals and different categories of individuals, the mean percentages of the relevant groups were assessed. Multiple regression analysis was performed to determine the factors influencing high and low antibody level percentages.
2.6. Statistical Analysis
The data for the groups were compared using a Student’s t-test after confirming the raw data were normally distributed, whereas the inter-group data were compared using either Pearson’s or Spearman’s tests. All tests were two-sided, and a p-value < 0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism, Version 9.3.1 (GraphPad Software, San Diego, CA, USA) software.
4. DiscussionOur study design was similar to that of Naaber et al., who assessed the levels of anti-SARS-CoV-2 spike RBD antibodies in 122 Estonian healthcare workers using the CLIA system [
4]. Consistent with their findings, we found a significant increase in antibody titers (10-fold in the present study vs. 19-fold in the study by Naaber et al.) after the second dose of BNT162b2, as well as a subsequent rapid decrease to 50% of the peak titer at 2 months and 20% at 3 months (in both studies). Subsequently, the antibody titers declined gradually to 1/10 (the present study) or 1/20 (Naaber et al.) of the peak titers 6 months after the second dose. The rapid decay of the antibody titers for up to 3 months and a gradual decline during the following 3 months have repeatedly been reported in other studies [
2,
3,
4,
5,
6]. This pattern might reflect the initial humoral B and T-cell immune response generated through the two doses of the vaccine [
14], the half-life of the human immunoglobulin [
15], and the existence of memory B cells, which continuously produce small amounts of specific immunoglobulin for the SARS-CoV-2 spike RBD, as is the case following a COVID-19 infection [
16,
17].Researchers have concentrated on investigating the duration of the neutralization activity shown through vaccination-induced antibodies. According to Naaber et al., the inhibition of the S protein of five variants of concern (wild-type, Alpha, Beta, Gamma, Delta, and Kappa) and the binding of the angiotensin-converting enzyme 2 (ACE2) receptor in an in vitro ELISA waned at 3 months after the second dose [
4]. Another study involving 225 healthy Japanese medical workers who received two doses of BNT162b2 found that the half-life for neutralizing the activity to block SARS-CoV-2 virions from infecting target cells determined using immune sera was 67.8 days [
3]. A test-negative study conducted from May to September 2021 evaluated the duration of protection from COVID-19 conferred through two doses of BNT162b2 in a large Israeli population [
6]. During that study period, the Delta variant was prevalent in Israel, and an increased odds ratio of COVID-19 RT-PCR positivity was observed in individuals 146 days after BNT162b2 vaccination compared with that noted in individuals
6]. Based on these data concerning the Delta variant, a two-dose BNT162b2 vaccination appears to be effective for approximately 3–4 months.The serum levels of the anti-SARS-CoV-2 spike RBD antibody and its neutralizing activity after vaccination reflect the different aspects of acquired humoral immunity; however, several studies have shown a close association between the two [
3,
4]. A high antibody titer equates to a high neutralizing activity. In our study, the mean antibody titer 3 months after the second dose was 2332 ± 1751 IU/mL with the CLIA and 163.9 ± 121 IU/mL with the ELISA. These values might indicate the minimum titer required for protection from COVID-19, particularly the Delta variant.In this study, older adult men showed a poor response to the COVID-19 mRNA vaccination. Aging is a significant risk factor for severe COVID-19 [
18]. Although several studies have reported an impaired immune response to the COVID-19 vaccine in older individuals [
7,
13], older COVID-19-recovered individuals show improved antibody and cellular responses, similar to younger individuals [
13]. Therefore, booster doses are likely to be effective in the older population. Modifying the vaccination protocol, such as shortening the interval between doses or increasing the mRNA dose, might help improve the immune response in high-risk groups.We selected SLE as a disease model. In a study involving 90 patients with SLE who had received two doses of BNT162b2, Izmirly et al. reported that 29% of the patients produced significantly lower levels of anti-SARS-CoV-2 spike RBD antibodies compared with the healthy controls [
11]. Other investigators have reported that 13.2% of patients with autoimmune systemic diseases were non-responders to the COVID-19 vaccination [
9]. In autoimmune inflammatory rheumatic diseases, immunosuppressive therapies, such as glucocorticoids, rituximab, mycophenolate mofetil, and abatacept, can impede the detection of anti-SARS-CoV-2-specific antibodies [
10,
19]. In the present study, 5/14 (35.7%) patients showed extremely low titers of anti-SARS-CoV-2 spike RBD antibodies, namely,
19], even at reduced doses.
The main limitation of our study was its small sample size. When we initiated the study, the two-dose vaccination regimen had already started for the Japanese population. Nonetheless, we obtained at least 50 samples for the time 0, the peak, 3 months, and 6 months after the second vaccination. Due to significant interindividual differences, even in the healthy younger group, the mean and median titers of the antibodies always showed a considerable difference.
5. Conclusions
Some concerns associated with COVID-19 vaccination using the mRNA vaccine BNT162b2 have been raised. This study found, first, that there was a rapid decline in the antibody titers after the second dose, requiring additional vaccinations at brief intervals. Second, some groups, such as older adult men or patients receiving immunosuppressive therapy, might be poor responders to vaccination. Finally, as booster vaccination has been reported to be effective in maintaining high antibody levels, modified protocols, such as applying shorter intervals or increasing the vaccine dosage for high-risk groups, might be required.







Comments (0)