1. IntroductionIt is estimated that coronavirus disease 2019 (COVID-19) has caused almost 15 million deaths during the first two years of the pandemic [
1]. Most patients with COVID-19 experience mild, self-limiting disease. However, the disease might be complicated by severe interstitial pneumonia that may result in acute hypoxemic respiratory failure and death [
2]. Known predictors of disease severity and a poor outcome are the male sex, comorbidities, advanced age, obesity, elevated biomarkers of organ damage, elevated biomarkers of inflammation, lymphopenia, evidence of substantial lung involvement, and the presence of hypoxemia [
3,
4]. Delayed antibody response against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigens has been identified as a predictor of in-hospital mortality [
5,
6]. The presence of neutralising antibodies within the first weeks of the disease is also associated with earlier virus clearance and the probability of survival [
7]. However, this topic remains controversial because previous studies have reported an association between high antibody titres in hospitalised patients and more severe disease [
8,
9,
10,
11]. Anti-S antibodies play a crucial role in recovering from COVID-19. Neutralising anti-S antibodies prevents the virus from entering cells, limits the extent of infection, and thus prevents the development of tissue damage in the affected organs, like lungs or myocardium [
12,
13]. Anti-S monoclonal antibodies administered at the early stage of the infection prevent the development of severe disease [
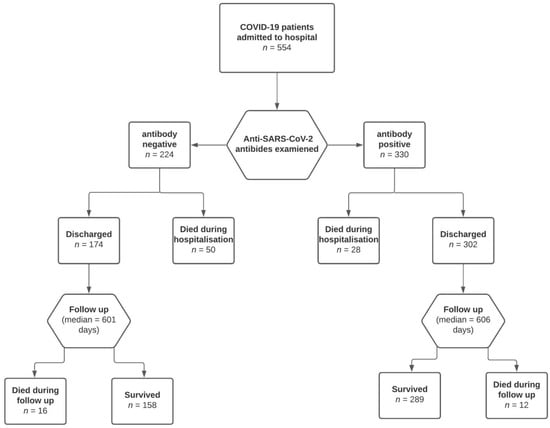
14]. Therefore, the early development of anti-S antibodies might result in lower organ damage, less severe disease, and a better long-term prognosis. The effects of the dynamics of anti-S antibody response on the long-term prognosis of COVID-19 patients is yet to be determined. The aim of our study was to assess the effects of delayed anti-S antibody response on the risk of in-hospital death and on the risk of death during the long-term follow-up in discharged COVID-19 patients. 3. ResultsA total of 554 patients (330 men and 224 women) met the inclusion criteria and were included in the study. Overall, 330 (63.0%) patients had positive IgG or IgM anti-S SARS-CoV-2 antibodies at the time of hospital admission. IgM antibodies were positive in 326 patients (58.8%), and IgG antibodies were positive in 244 patients (46.6%). Only six IgG-positive patients had negative IgM antibodies. A significantly higher proportion of the patients with negative anti-S SARS-CoV-2 antibodies died during the hospital stay and during the follow-up (
Table 1). The baseline characteristics of the cohorts of antibody-positive and antibody-negative patients are provided in
Table 1. The severity of the disease categories in the cohorts, according to the NIH, is provided in
Table 2. Patients with negative anti-S SARS-CoV-2 IgM and IgG antibodies at the time of admission were referred to the hospital sooner, had lower CRP and D-dimer concentrations, and were hospitalised longer. They were also more likely to be admitted to an intensive care unit and more often required invasive mechanical ventilation (
Table 1). In the multivariate analysis, the negative anti-S SARS-CoV-2 IgM and IgG antibodies were associated with a higher risk of in-hospital death, independent of their age, time from symptom onset to admission, CRP, D-dimer, number of comorbidities, disease severity and baricitinib therapy (
Table 3). In the Cox regression model, the negative anti-SARS-CoV-2 antibodies at the time of admission were associated with a higher risk of death during the follow-up, independent of age, time from symptom onset to admission, CRP, D-Dimer, number of comorbidities, disease severity, and baricitinib therapy (
Table 4,
Figure 2). The results of the analyses are provided in the
supplementary material (Supplementary Materials, Tables S1–S15) in more detail. 4. Discussion
This study has confirmed that the absence of detectable anti-S SARS-CoV-2 IgM and IgG antibody production at the time of hospital admission is associated with an increased risk of in-hospital death and all-cause death after hospital discharge in unvaccinated naive COVID-19 patients. This association was irrespective of age, number of comorbidities, the time from disease onset to antibody assessment, and other possible confounders. These findings contribute to the evidence that the development of anti-S SARS-CoV-2 antibodies counteracts the pathomechanisms precipitating the progression of tissue injury and the development of more severe disease. Our study also suggests that the effect on prognosis lasts for a long time after hospital discharge. The value of our study is further highlighted by the fact that it was conducted on the unvaccinated and immunologically naive population, and thus the results were not confounded by any pre-existing anty-SARS-CoV-2 immunity. Similar results will be difficult to obtain in the future because of mass vaccination campaigns and the high prevalence of natural immunity.
There is a large body of evidence connecting more severe disease to more vigorous antibody response in COVID-19. Several studies have found a positive association between antibody titres and disease severity and the probability of the risk of death in patients hospitalised with COVID-19. The authors of these studies have proposed that more severe disease stimulates more intensive antibody production [
8,
9,
10,
11]. This association was also apparent while measuring neutralising activity [
9,
11]. On the other hand, there is evidence suggesting that the prompt development of antibodies is associated with more favourable outcomes [
5,
6,
7].The main difference between the studies that have connected higher titres of anti-SARS-CoV-2 antibodies with severe and fatal disease [
8,
9,
10,
11] and later studies that identified the protective role of the early development of strong antibody response [
5,
6,
7] is the temporal factor. The studies that identified the early antibody response as a protective factor assessed it at the early stages of the disease. On the other hand, authors that found an association between strong antibody response and more serious disease measured them later in the course of the disease or after its resolution.De Vito et al. [
5] found that a lower antibody titre against SARS-CoV-2 in the early stage of the disease is associated with a higher risk of in-hospital death from COVID-19, irrespective of age. However, the number of participants in their study was relatively small, and the follow-up was only 40 days. They did not measure neutralizing activity. Zohar et al. [
6] found a delayed IgG1 anti-S response in COVID-19 nonsurvivors and survivors of moderate disease compared with survivors of severe disease. They also found it compromised Fcγ receptor binding and Fc effector activity in the nonsurvivors and proposed that this impairment is associated with a deficient humoral immune response. However, they found no association between anti-S IgM antibody titres and disease severity during the first week of the disease. During the second week of the disease, they found higher IgG and IgM titres in the survivors of severe disease compared with the survivors of moderate disease and the nonsurvivors. They found no difference in neutralising activity or in the titres of anti-N antibodies across the groups. The time of follow-up was 30 days. Dispinseri et al. [
7] found that the presence of neutralising anti-S antibodies within the first weeks of the disease is associated with earlier virus clearance and a higher probability of survival. They suggested that a compromised immune response is a major trait of patients with severe COVID-19 [
7]. Atyeo et al. [
17] also emphasised the role of the anti-S antibody response as a factor shifting the disease trajectory towards a milder course. Although anti-SARS-CoV-2 IgG titres in survivors were not greater compared with deceased patients, their immune response was characterised by higher titres of anti-S IgM but decreased functional antibody responses to the nucleocapsid antigen. They found no difference in neutralising activity between the deceased and convalescent patients. They measured the antibody response approximately nine days after the onset of symptoms.According to our results and the evidence of the studies cited above, we suggest that a delayed antibody response is more likely to occur in the early acute phase of severe or critically ill COVID-19 patients and is associated with poor outcomes. However, later in the disease course of severe or critical illness, the production of antibodies rises significantly and eventually overtakes the production of antibodies in patients with less severe disease. Higher anti-SARS-CoV-2 antibody production is also associated with the more severe disease after disease resolution. Yan et al. [
18] found that survivors of severe disease had higher titres of anti-SARS-CoV-2 antibodies one year after the resolution of an acute infection. Hansen et al. [
19] also found a positive correlation between disease severity and antibody titres in convalescent individuals. Therefore, the anti-S SARS-CoV-2 antibody response in severe cases develops later; however, the results presented higher antibody titres in the convalescent stage.Our study also found that patients with negative anti-S SARS-CoV-2 antibodies at the time of hospital admission have a higher risk of all-cause death after hospital discharge. The novelty of our study lies in the relatively long median follow-up length. Our results suggest that the effects of delayed antibody response in COVID-19 last for a long period after hospital discharge. The endpoint in our study was the all-cause death, and we were unable to analyse the specific causes of death in the deceased patients due to the lack of autopsies conducted on deceased patients during the pandemic. The exact mechanism that leads to an impaired prognosis (lasting for months) after hospital discharge in patients with delayed antibody response needs to be clarified by further studies. We propose that the more severe organ damage and its sequelae caused by more severe disease in antibody-negative subjects might contribute to the increased risk of all-cause death after hospital discharge. However, there might be other mechanisms because we were unable to analyse the precise causes of death in the deceased patients. García-Abellán et al. [
20] found weaker antibody responses in patients suffering from persistence after the resolution of acute COVID-19 and suggested that antibody-mediated immune reaction plays an important role in the recovery phase.There is substantial evidence that deregulated and compromised immune responses play a pivotal role in the pathogenesis of severe disease in COVID-19 [
21]. Severe disease is associated with reduced CD3+, CD4+ CD8+, and natural killer cells [
22], a higher neutrophil to lymphocyte (N/L) ratio, and higher concentrations of proinflammatory cytokines [
15]. The presence of more severe disease is also associated with a lower total concentration of immunoglobulins in the acute stage of the disease [
21,
22].Anti-S antibodies play a crucial role in the ability of the host to clear SARS-CoV-2 and to recover from infection. Virus-neutralising anti-S antibodies bind to the receptor-binding domain and prevent interaction with angiotensin-converting enzyme 2 (ACE2), inhibiting virus entry [
23]. Blocking the interaction between SARS-CoV-2 and ACE2 in tissues not only prevents the infection of cells, but also counteracts the inhibitory effects of viral S-protein on ACE2 activity. The binding of SARS-Co-2 virions to ACE2 significantly decreases its activity in tissues, which contributes to the stimulation of the inflammatory response and probably plays a crucial role in cytokine storm development and progression [
24,
25]. Engineered ACE2 with augmented binding affinities for S-protein acting as decoys prevents the development of lung injury in a mouse model [
26]. Monoclonal antibodies that bind to the receptor binding domain of the SARS-CoV-2 S-protein have the ability to prevent the development of severe disease if administered at the early stage of the infection [
14]. Neutralizing anti-S antibodies are also regarded as being responsible for the protection against severe disease and lung and other organ injuries in vaccinees and convalescent patients and are not fully diminished by the occurrence of new variants and subvariants [
27,
28]. The fact that more severe disease eventually leads to higher antibody titres is believed to be caused by higher viraemia and a much stronger antigen-driven extrafollicular response [
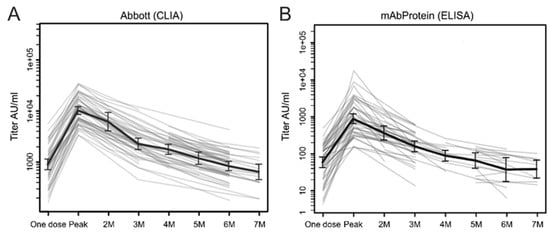
27]. The production of immunoglobulins in COVID-19 usually starts within the first or second week of infection and peaks at two months [
29].Patients with positive anti-S SARS-CoV-2 antibodies at the time of hospital admission presented with higher CRP and D-dimer concentrations. However, the CRP concentration was not associated, and the D-dimer concertation was positively associated with a higher risk of death during hospitalisation but not during the follow-up in multivariate analyses. CRP and D-dimer are well-known prognostic markers of higher in-hospital mortality regarding COVID-19 [
3,
4]. Latifi-Pupovci et al. [
30] described the positive correlation between CRP and D-dimer concentrations with antiSARS-CoV-2 IgG in the acute stage of the disease. To the best of our knowledge, the nature of these associations has not been elucidated yet.This study has several limitations. We only used qualitative methods for antibody detection. Therefore, we were unable to assess the association between antibody titres with the prognosis of the disease. We used point-of-care lateral flow serological tests for quantitative analysis because they represent a more available, faster, less expensive, and less elaborate method compared with enzyme-linked immunoassays, making them a better alternative in an environment with strained human and financial resources during the COVID-19 pandemic. The point-of-care tests used in our study are characterised by a sensitivity of > 98% and a specificity of 100% relative to the enzyme-linked immunoassays [
31,
32]. Additionally, due to the observational character of our study and the recruitment of consecutive patients, the patient cohorts are not methodically matched for age and comorbidities. However, we do not suggest that this led to a significant bias because there is not a statistically significant difference in the medians of age and number of comorbidities and their distribution between the cohorts. We also mitigated the effects of possible confounders by using multivariate analysis. We also performed a collinearity analysis to assess if the variables in the regression models are truly independent. The results are provided in the
supplementary material. The time from disease onset to admission was significantly shorter in patients with negative anti-S SARS-CoV-2 antibodies, but these associations were not present in the multivariate models. We only assessed the anti-S, not ani-N, antibodies; therefore, we are unable to conclude if the dynamic of anti-N response is also associated with a higher risk of in-hospital death and death after hospital discharge. The previous study by Zohar et al. [
6] found a delayed anti-S response but no anti-N response in COVID-19 nonsurvivors. Additionally, there is substantial evidence that anti-S antibodies are crucial in the recovery from COVID-19 [
23,
25,
26,
28]. There is even evidence that anti-N antibodies might contribute to the pathogenesis of the cytokine storm in COVID-19 [
33]. Therefore, we focused on anti-S antibody response and utilised just the test to assess the presence of anti-S antibodies. The follow-up period was not uniform for all patients; however, there was no difference in the median length of the follow-up between the cohorts; therefore, we suggest that this fact did not create a bias in the results. The baricitinib treatment was utilised in patients admitted from March 2021 according to the institutional guidelines. The institutional board decided to add baricitinib to the institutional guidelines according to the results of a study by Rodriguez-Garcia et al. [
34]. There was no difference in baricitinib utilisation between the cohorts, and baricitinib treatment was included in the multivariate analysis; therefore, we suggest that baricitinib treatment did not create a bias in the results. The causes of death in the patients that died during the hospitalisation were assessed by autopsies. However, the autopsy is also not an absolutely exact method to determine the cause of death regarding COVID-19 [
35].







Comments (0)