



Remember me



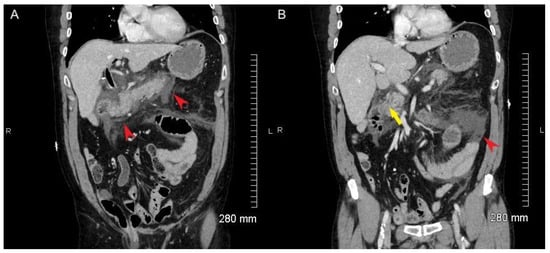



Figure 1. CT abdomen and pelvis with contrast demonstrates significant peripancreatic fluid and fat stranding extending to porta hepatis, consistent with acute pancreatitis (A,B, red arrowheads). The patient is status post cholecystectomy. There is pneumobilia, likely associated with prior cholecystectomy. The biliary tree is prominent with abnormal wall enhancement. The CBD measures 9 mm proximally and 5 mm distally. No definite signs of choledocholithiasis are seen in the distal CBD (B, yellow arrowhead).
Figure 1. CT abdomen and pelvis with contrast demonstrates significant peripancreatic fluid and fat stranding extending to porta hepatis, consistent with acute pancreatitis (A,B, red arrowheads). The patient is status post cholecystectomy. There is pneumobilia, likely associated with prior cholecystectomy. The biliary tree is prominent with abnormal wall enhancement. The CBD measures 9 mm proximally and 5 mm distally. No definite signs of choledocholithiasis are seen in the distal CBD (B, yellow arrowhead).
Figure 2. Intense 18F-FDG uptake (SUVmax = 13.3) along the CBD (coronal images, (A). PET, (B). PET/CT, (C). CT, (D). Trans-axial images, PET/CT and CT, (E). Sagittal images, PET/CT and (F). Maximum intensity projection, thought to be due to ERCP-induced inflammation. There is mild fat stranding adjacent to the CBD on the corresponding low-dose CT images without a definite radiopaque stone in the distal CBD. On MIP, intense uptake at common bile duct is noted (short arrow). There is a hypermetabolic lesion in the left lung (long arrow), confirmed to be a metastasis from colon cancer on biopsy. The patient has a remote history of colon cancer 26 years ago, status post-colectomy with ileostomy. Intense uptake in the bowel loops is secondary to metformin use.
Figure 2. Intense 18F-FDG uptake (SUVmax = 13.3) along the CBD (coronal images, (A). PET, (B). PET/CT, (C). CT, (D). Trans-axial images, PET/CT and CT, (E). Sagittal images, PET/CT and (F). Maximum intensity projection, thought to be due to ERCP-induced inflammation. There is mild fat stranding adjacent to the CBD on the corresponding low-dose CT images without a definite radiopaque stone in the distal CBD. On MIP, intense uptake at common bile duct is noted (short arrow). There is a hypermetabolic lesion in the left lung (long arrow), confirmed to be a metastasis from colon cancer on biopsy. The patient has a remote history of colon cancer 26 years ago, status post-colectomy with ileostomy. Intense uptake in the bowel loops is secondary to metformin use.
Figure 3. A follow-up MRCP 9 days after the 18F-FDG PET shows no evidence of acute cholangitis or acute pancreatitis. Coronal T2 weighted MIP imaging (SSTSE, slice thickness 30 mm) shows the CBD (arrow head) and main pancreatic duct (arrow). No lesions or abnormal findings within the CBD. The size of the CBD measures 6 mm.
Figure 3. A follow-up MRCP 9 days after the 18F-FDG PET shows no evidence of acute cholangitis or acute pancreatitis. Coronal T2 weighted MIP imaging (SSTSE, slice thickness 30 mm) shows the CBD (arrow head) and main pancreatic duct (arrow). No lesions or abnormal findings within the CBD. The size of the CBD measures 6 mm.
Comments (0)