


Remember me






A 67-year-old man underwent surgery for repair of an inguinal hernia. The clinical history of the patient included a surgical intervention after a traffic accident more than 40 years ago but was otherwise unremarkable. Due to complications, a laparotomy was necessary, and a postoperative CT was performed. A small bowel obstruction was ruled out, but the CT revealed multiple space-occupying lesions in the abdomen and pelvis with contrast enhancement. No visceral or bone lesions were identified. No spleen was present.
Initially, a malignant disease, particularly a lymphoma, was suspected, and magnetic resonance imaging (MRI) of the abdomen was performed for further evaluation. This confirmed the partially lobulated, well-defined lesions (Figure 1). In view of the previous surgery and the missing spleen, the differential diagnosis of multilocular ectopic splenic tissue (splenosis) was considered. 3. PET/CT ImagingTo avoid further interventions, a PET/CT with [68Ga]Ga-oxine-labeled RBCs was performed. Synthesis of [68Ga]Ga-oxine and RBC labeling procedures were adapted from [6,7]. A total of 8 mL of venous blood was taken from the patient in 2 mL of citrate anticoagulant buffer. The RBCs were separated from the plasma via centrifugation and heated to 48 °C for 10 min in order to induce heat denaturation and labeling with [68Ga]Ga-oxine. After three washing cycles with 0.9% saline, the labeled RBCs were resuspended. RBCs containing 188 MBq [68Ga]Ga-oxine were reinjected intravenously.Imaging was performed on a Biograph mCT 40 scanner (Siemens Healthineers, Germany). After an unenhanced, low-dose CT for anatomical correlation and attenuation correction, an early dynamic PET was acquired continuously for 300 s, beginning with i.v. tracer injection. Static PET images (5 min per bed position) were acquired 10 and 25 min after tracer injection.
All abdominal and pelvic masses showed a high tracer uptake increasing over time (Figure 2), with the highest uptake values measured in the subhepatic index lesion (Figure 1 and Figure 2, arrows): SUVmean: 69.1/94.1 at 10/25 min after tracer injection, respectively, showing an increase of 36% between the two time points. During the same interval, blood pool activity decreased (SUVmean: 9.6/6.8, −29%), indicating the removal of the labeled, heat-damaged RBCs from the blood by the functioning splenic tissue. The diagnosis of disseminated splenosis was confirmed. Since no symptoms were present and there was no evidence of an increased susceptibility to infections, no further treatment was necessary. 4. DiscussionThis case illustrates the advantages of high-resolution [68Ga]Ga-RBC-PET/CT for the differentiation of splenic tissue from malignancies. The spatial resolution of PET/CT is approx. 2 mm, while that of 99mTc single-photon emission computed tomography (SPECT) is 6–8 mm. PET/CT allows for voxel-based absolute uptake quantification and has the option of dynamic imaging for a time-resolved assessment of the tracer uptake.
In patients with small lesions, including accessory or maybe intrapancreatic spleens mimicking metastases of neuroendocrine tumors, this will be even more important and may avoid unnecessary surgical interventions with potentially severe complications [8,9,10]. It has been shown that the specificity of spleen scintigraphy is high, but its sensitivity for the detection of accessory spleens may be limited in non-splenectomized patients [11]. To date, for RBC-PET/CT, we have not detected a sink effect in patients with a native spleen, which may have limited the detectability of other small structures containing functioning splenic tissue.The availability of PET/CT alternatives to evaluate various clinical issues is becoming increasingly important because the supply of molybdenum-99 (99Mo) and, thus, technetium-99m has been repeatedly disrupted in the past [12]. Currently, supply shortages of 99Mo are anticipated for Europe in November and December 2022, and these situations may become more frequent because the number of facilities producing 99Mo is decreasing [13].RBC-PET/CT should be kept in mind as a problem solver in difficult cases of splenic disease, including splenosis and asplenia. It represents a feasible alternative to 99mTc-based scintigraphic methods.
Author ContributionsConceptualization, A.W., M.F. and R.D.; methodology, M.F. and R.D.; validation, M.F., R.D. and A.W.; investigation, A.W.; writing—original draft preparation, A.W.; writing—review and editing, A.W., M.F. and R.D.; visualization, R.D.; supervision, M.F. All authors have read and agreed to the published version of the manuscript.
FundingThis research received no external funding.
Institutional Review Board StatementThe examinations were part of the clinical workup of the patient. Ethical review and approval were not necessary. The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent StatementInformed consent was obtained from the patient.
Conflicts of InterestThe authors declare no conflict of interest.
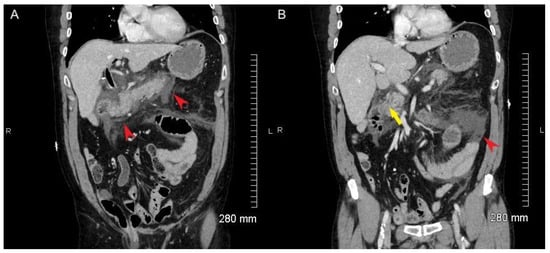
ReferencesCaroli, J. Ist observation of a primary tumor of the spleen (reticulosarcoma) diagnosed by the splenic scintillogram using radiogold. Rev. Medico-Chirurgicale Mal. Foie 1961, 36, 1–8. [Google Scholar]Kuba, J.; Charamza, O.; Kuchar, O.; Husak, V.; Krc, I. Spleen scintigraphy with radiopertechnate (99mTc). Ceskoslovenska Gastroenterol. A Vyziv. 1968, 22, 281–288. [Google Scholar]Wong, A.; Fung, K.; Wong, W.; Ng, K.; Kung, B.; Kan, Y. Multimodality imaging of developmental splenic anomalies: Tips and pitfalls. Clin. Radiol. 2022, 77, 319–325. [Google Scholar] [CrossRef] [PubMed]Drescher, R.; Gröber, S.; Seifert, P.; Freesmeyer, M. Differentiation of residual splenic tissue from neuroendocrine tumor metastasis on PET/CT with heat-damaged, Ga-68-oxine-labeled red blood cells. Jpn. J. Clin. Oncol. 2020, 51, 160–161. [Google Scholar] [CrossRef] [PubMed]Freesmeyer, M.; Gröber, S.; Greiser, J.; Seifert, P.; Gühne, F.; Drescher, R. PET/CT with [68Ga]gallium-oxine-labeled heat-denatured red blood cells for detection of dystopic splenic tissue. Eur. J. Pediatr. 2020, 48, 644–646. [Google Scholar] [CrossRef] [PubMed]Socan, A.; Petrik, M.; Peitl, P.K.; Krošelj, M.; Rangger, C.; Novy, Z.; Svajger, U.; Gmeiner, T.; Decristoforo, C. On-cartridge preparation and evaluation of 68Ga-, 89Zr- and 64Cu-precursors for cell radiolabelling. Nucl. Med. Biol. 2019, 71, 23–31. [Google Scholar] [CrossRef] [PubMed]Thompson, S.; Rodnick, M.E.; Stauff, J.; Arteaga, J.; Desmond, T.J.; Scott, P.J.H.; Viglianti, B.L. Automated synthesis of [68Ga]oxine, improved preparation of68Ga-labeled erythrocytes for blood-pool imaging, and preclinical evaluation in rodents. MedChemComm 2018, 9, 454–459. [Google Scholar] [CrossRef] [PubMed]Ates, I.; Yazici, O.; Yazilitas, D.; Ozdemir, N.; Zengin, N. Accessory spleen hypertrophy mimicking colon cancer metastasis. Exp. Oncol. 2016, 38, 202–203. [Google Scholar] [CrossRef] [PubMed]Rosar, F.; Ries, M.; Khreish, F.; Ezziddin, S. Remember the Pitfall. Clin. Nucl. Med. 2019, 45, 250–251. [Google Scholar] [CrossRef] [PubMed]Ryoo, H.G.; Choi, H.; Cheon, G.J. Spleen Scan for 68Ga-DOTATOC PET-Positive Pancreatic Tail Lesion: Differential Diagnosis of Neuroendocrine Tumor from Accessory Spleen. Nucl. Med. Mol. Imaging 2019, 54, 43–47. [Google Scholar] [CrossRef] [PubMed]Ekmekçi, Ş.; Diz-Küçükkaya, R.; Türkmen, C.; Adalet, I. Selective Spleen Scintigraphy in the Evaluation of Accessory Spleen/Splenosis in Splenectomized/Nonsplenectomized Patients and the Contribution of SPECT Imaging. Mol. Imaging Radionucl. Ther. 2015, 24, 1–7. [Google Scholar] [CrossRef] [PubMed]Ruth, T.J. The Shortage of Technetium-99m and Possible Solutions. Annu. Rev. Nucl. Part. Sci. 2020, 70, 77–94. [Google Scholar] [CrossRef]Nuclear Medicine Europe (NMEU). Communication from NMEU to EU Observatory for the Supply of Medical Radioisotopes: Global Mo-99 and I-131 Production Impacted by Delay of BR2 Reactor Restarting from Scheduled Maintenance. Available online: https://s3.amazonaws.com/rdcms-snmmi/files/production/public/images/HPRA/Communication%20Mo-99%20and%20I-131%20-%2028%20October%202022.pdf (accessed on 14 November 2022).Figure 1. MR imaging showed well-defined masses (arrow: index lesion in the upper abdomen), moderately hyperintense on T2-weighted spectral presaturation with inversion recovery (SPIR) images (a) and with nearly homogeneous contrast enhancement on T1-weighted multiecho 2-point Dixon (mDIXON) sequences (b).
Figure 1. MR imaging showed well-defined masses (arrow: index lesion in the upper abdomen), moderately hyperintense on T2-weighted spectral presaturation with inversion recovery (SPIR) images (a) and with nearly homogeneous contrast enhancement on T1-weighted multiecho 2-point Dixon (mDIXON) sequences (b).
Figure 2. Multiple masses with high tracer uptake seen on RBC-PET/CT (a): non-contrast CT, (b): PET/CT fusion, (c): PET maximum intensity projection (MIP) image acquired 25 min after tracer injection).
Figure 2. Multiple masses with high tracer uptake seen on RBC-PET/CT (a): non-contrast CT, (b): PET/CT fusion, (c): PET maximum intensity projection (MIP) image acquired 25 min after tracer injection).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Comments (0)