
記住我
Magnesium ranks as the second intracellular cation with a critical blood level of 1.46–2.68 mg/dL, influencing over 300 enzyme systems among Na–K ATPase, Ca–K homeostasis, neural, and muscular activities.1,2 The incidence of hypomagnesemia in critically ill patients reaches 60%, in contrast to only 2% in the general population.3 Symptomatic or asymptomatic hypomagnesemia produces serious complications, such as hypocalcemia, hypokalemia, cardiac arrhythmias, neurotoxicity, and psychiatric manifestations, eventually increasing the rates of morbidity and mortality.4,5 Some groups of patients, particularly the elderly, have a higher risk due to lower intake, decreased absorption, chronic stress, and increased urinary loss with their frequent use of diuretics and digitalis.6
Although many parameters have been investigated to reduce mortality in intensive care units (ICU), hypomagnesemia management has not been well addressed, leading to uncertain conclusions and recommendations.7,8 For instance, a previous cohort study revealed that daily magnesium supplementation in the ICU was associated with lower mortality rates.9 However, this effect was not found to be independent, and the exact cause was unknown.9 Likewise, a meta-analysis concluded that magnesium administration reduces atrial fibrillation, yet, the conclusion was limited to ICU patients after cardiac surgery and within this type of arrhythmia.10
In the present study, we have examined the effect of serum magnesium levels and magnesium administration on clinical outcomes for critically ill patients. The general objectives of the study included the length of ICU stay, the requirement of mechanical ventilation, and the incidence of mortality.
Patients and methodsEthical approval for this study was provided by the Ethical Committee of Critical Care Department, Kasr Al-Ainy University Hospital, Egypt.
Study design and patientsWe planned a retrospective chart review of patients admitted to the intensive care units of Kasr Al-Ainy University Hospital from January 2011 to January 2015. Adult patients were included irrespective of their cause of admission to ICU. We excluded patients with less than 24 hours of ICU stay and patients with history of magnesium treatment prior to ICU admission. Eligible patients were divided into two groups: normomagnesaemic and hypomagnesaemic groups based on their initial measured serum Magnesium level on admission to the ICU.
Data collectionRetrieved data included age at admission, gender, primary cause of admission, hemodynamic measures, routine laboratory findings, level of magnesium, APACHE II score, SOFA score, needs for mechanical ventilation, days on mechanical ventilation, days, days of ICU stays, and mortality. The normal level of magnesium was defined as 1.9–2.2 mg/dL.
Study's outcomesWe primarily relate magnesium levels with patient's outcomes regarding mortality, ICU stay, needs for mechanical ventilation, days on mechanical ventilation, and SOFA score.
Statistical analysisRetrieved data were summarized and processed with IBM SPSS statistical software (version 25). Frequencies were used to describe categorizes and numeric were summarized into mean ± SD. The hypothesize of significant associations between various parameters and magnesium levels was tested by Chi-square test for categorical variables and Mann-Whitney test for continuous variables. P-value < .05 was regarded as statistically significant
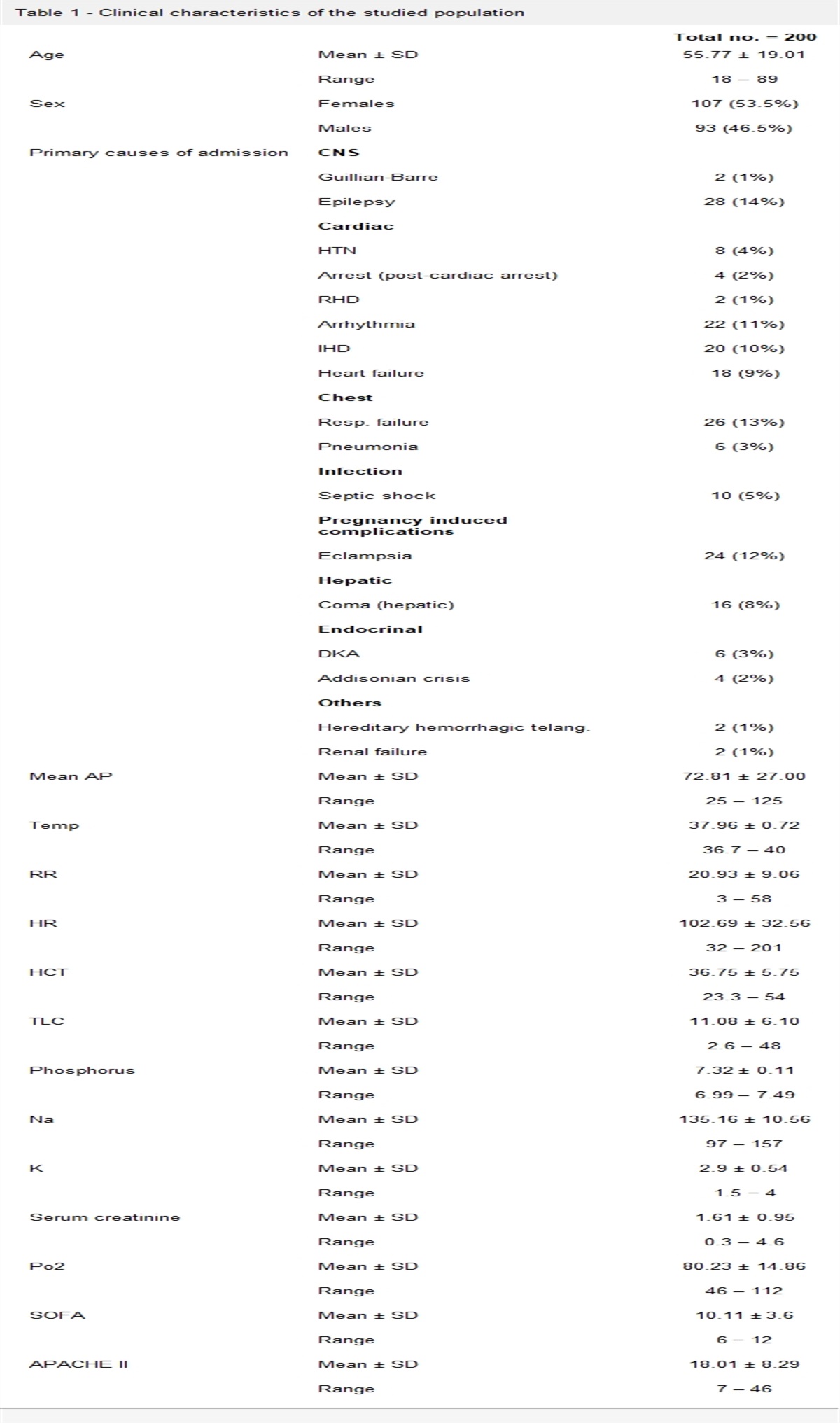
ResultsThe present retrospective study was performed on 200 patients with a mean age of 55.77 ± 19.01 years old. The majority of patients were females (53.5%). The majority of the patients had cardiac causes of admission, followed by respiratory causes. As regard to hemodynamics, the mean arterial blood pressure was 72.81 ± 27 mm Hg, mean temperature was 37.96°C ± 0.72°C, mean respiratory rate was 20.93 ± 9.06 per minutes, and the heart rate ranged was 102.69 ± 32.56 beats per minutes. The mean APACHE II score was 18.01 ± 8.29 and the mean SOFA score was 10.11 ± 3.6 (Table 1).
Table 1 - Clinical characteristics of the studied population Total no. = 200 Age Mean ± SD 55.77 ± 19.01 Range 18 – 89 Sex Females 107 (53.5%) Males 93 (46.5%) Primary causes of admission CNS Guillian-Barre 2 (1%) Epilepsy 28 (14%) Cardiac HTN 8 (4%) Arrest (post-cardiac arrest) 4 (2%) RHD 2 (1%) Arrhythmia 22 (11%) IHD 20 (10%) Heart failure 18 (9%) Chest Resp. failure 26 (13%) Pneumonia 6 (3%) Infection Septic shock 10 (5%) Pregnancy induced complications Eclampsia 24 (12%) Hepatic Coma (hepatic) 16 (8%) Endocrinal DKA 6 (3%) Addisonian crisis 4 (2%) Others Hereditary hemorrhagic telang. 2 (1%) Renal failure 2 (1%) Mean AP Mean ± SD 72.81 ± 27.00 Range 25 – 125 Temp Mean ± SD 37.96 ± 0.72 Range 36.7 – 40 RR Mean ± SD 20.93 ± 9.06 Range 3 – 58 HR Mean ± SD 102.69 ± 32.56 Range 32 – 201 HCT Mean ± SD 36.75 ± 5.75 Range 23.3 – 54 TLC Mean ± SD 11.08 ± 6.10 Range 2.6 – 48 Phosphorus Mean ± SD 7.32 ± 0.11 Range 6.99 – 7.49 Na Mean ± SD 135.16 ± 10.56 Range 97 – 157 K Mean ± SD 2.9 ± 0.54 Range 1.5 − 4 Serum creatinine Mean ± SD 1.61 ± 0.95 Range 0.3 – 4.6 Po2 Mean ± SD 80.23 ± 14.86 Range 46 – 112 SOFA Mean ± SD 10.11 ± 3.6 Range 6 − 12 APACHE II Mean ± SD 18.01 ± 8.29 Range 7 – 46Concerning patients’ outcomes, 88 patients needed mechanical ventilation with duration ranged from 1 to 18 days a mean of 4.7 ± 3.1 days. ICU stay for the patients ranged from 1 to 22 with mean of 6.57 ± 3.52. The mortality rate was 27% (Table 2).
Table 2 - Description of clinical data among studied patients Total no. = 200 Mechanical vent. No 112 (56.0%) Yes 88 (44.0%) M.V days Mean ± SD 4.70 ± 3.10 Range 1 – 18 Days in ICU Mean ± SD 6.57 ± 3.52 Range 1 – 22 Mortality Survived 146 (73.0%) Non survived 54 (27.0%)A total of 114 patients were hypomagnesaemic (57%). There were no significant associations between hypomagnesemia and gender or age (Table 3). Patients with hypomagnesemia were more likely to be associated with eclampsia, seizures, and other diseases (P = .024; Table 1). Besides, patients with hypomagnesemia were more likely to be associated with septic shock and infection (P = .03). As regard hemodynamics, patients with hypomagnesemia had significantly lower mean arterial blood pressure (64.42 ± 22.19 vs 79.14 ± 28.63 mm Hg, P < .001). There were no significant associations between hypomagnesemia and HCT values (P = .618), TLC (P = .179), serum phosphorus (P = .721), PO2 (P = .79), and other laboratory parameters (P > .05). The mean APACHE II was 18.19 ± 8.04 in normomagnesaemic patient and 17.88 ± 8.51 in hypomagnesaemic patients, with P-value of .795. The mean SOFA score was 9.84 ± 3.41 in normomagnesaemic patients and 10.78 ± 4.04 in hypomagnesaemic patients, with P-value of .523 (Table 3).
Table 3 - Shows incidence of hypomagnesaemia according to age and sex and association with hypocalcaemia and hypokalemia Normomagnesaemia Hypomagnesaemia Independent t test N = 86 N = 114 t P Sex Females 40 (46.5%) 67 (58.8%) 2.962 .085 Males 46 (53.5%) 47 (41.2%) Age Mean ± SD 57.51 ± 16.62 54.46 ± 20.60 1.126 .261 Range 22 – 80 17 – 89 Hct Mean ± SD 36.98 ± 5.50 36.57 ± 5.96 0.500 .618 Range 23.6 – 51 23.3 – 54 Tlc Mean ± SD 11.75 ± 5.45 10.58 ± 6.52 1.349 .179 Range 2.6 – 28.9 3.7 – 48 Ph Mean ± SD 7.32 ± 0.11 7.32 ± 0.10 0.357 .721 Range 6.99 – 7.49 7.01 – 7.44 Po2 Mean ± SD 79.91 ± 15.46 80.47 ± 14.45 −0.266 .790 Range 46 – 112 46 – 96 serum cr Mean ± SD 1.69 ± 0.94 1.55 ± 0.96 0.991 .323 Range 0.5 – 4.1 0.3 – 4.6 Na Mean ± SD 135.63 ± 8.69 134.81 ± 11.80 0.543 .587 Range 112 – 153 97 – 157 Mean AP Mean ± SD 64.42 ± 22.19 79.14 ± 28.63 −3.955 .000 Range 28 – 114 25 – 125 temp Mean ± SD 37.99 ± 0.80 37.94 ± 0.65 0.491 .624 Range 36.7 – 40 36.9 – 39.7 RR Mean ± SD 21.09 ± 9.42 20.81 ± 8.83 0.220 .826 Range 3 – 58 4 – 42 HR Mean ± SD 99.67 ± 37.19 104.96 ± 28.54 −1.138 .256 Range 32 – 201 41 – 198 SOFA Mean ± SD 9.84 ± 3.41 10.78 ± 4.04 0.305 .523 Range 6 – 21 6 – 19 APACHE II Mean ± SD 18.19 ± 8.04 17.88 ± 8.51 0.260 .795 Range 7 – 46 7 – 42Among hypomagnasaemic patients, there were 60 patients (52.6%) needed to be mechanically ventilated with mean period of 4.75 ± 3.29days, while in normomagnesaemic patients, there were 28 patients (32.56%) needed to be mechanically ventilated with a mean period of 4.63 ± 2.8 days (P = .005). In hypomaganesaemic patients, the mean days of ICU stay was 7.27 ± 3.15 days, compared to 6.17 ± 3.52 for normomagnesaemic patients (P = .021). Among hypomagnesaemic patients, the mortality rate was 24.6%, compared to 30.2% in normomagnesaemic patient (P = .37; Table 4).
Table 4 - Relation of measured magnesium levels on outcomes of our study population Normomagnesaemic Hypomagnesaemia Independent t test No. = 86 No. = 114 t P Mechanical vent. No 58 (67.44%) 54 (47.4%) 8.016 .005 Yes 28 (32.56%) 60 (52.6%) M.V days Mean ± SD 4.63 ± 2.80 4.75 ± 3.29 −0.181 .857 Range 2 – 11 1 – 18 Days in ICU Mean ± SD 6.17 ± 3.52 7.27 ± 3.15 2.322 .021 Range 1 – 18 2 – 22 Mortality No 60 (69.8%) 86 (75.4%) 0.800 .371 Yes 26 (30.2%) 28 (24.6%)Although many parameters have been investigated to reduce mortality in ICU, hypomagnesemia management has not been well addressed, leading to uncertain conclusions and recommendations.7,8 Our present study aimed to evaluate the prevalence of hypomagnesaemia in critically ill and to assess the effect of magnesium on patient outcomes in terms of ICU stay, hospital stay, ventilator days, and mortality.
A cumulative body of evidence suggests that hypomagnesaemia is usually missed in critically ill patients, despite its potential impact on patients’ outcomes.11 Abnormal magnesium levels in the ICU is attributed to several factors including impaired gastrointestinal absorption, malnutrition, therapeutics, and associated electrolytes abnormalities.12 Abnormal magnesium levels can lead to critical disturbance in the normal functions of several organs, leading to a wide range of complications such as secondary hypokalemia or hypocalcemia, ventricular arrhythmia, neuromuscular abnormalities, prolonged stay, and mortality.13 Previous studies showed that hypomagnesaemia is common in the ICU setting, with wide variations in the reported prevalence.14–16 Our study assessment of magnesium level in ICU showed that 57% of the patients had hypomagnesaemia. In concordance with our findings, Limaye et al.,17 conducted a prospective observational study on 100 ICU patients and found that 52% of the patients had hypomagnesaemia at admission. Nonetheless, such prevalence was notably higher than observations from other registries. For example, Sunil Kumar et al.,8 recruited 105 patients to assess the prevalence of hypomagnesaemia in a follow-up period of 1 year; they found that 25% of patients had hypomagnesaemia. Another report by Zafar et al.,11 reported a prevalence of 24.3%. We assume that the wide variations in the reported prevalence of hypomagnesaemia in the ICU setting are attributed to utilization of different cut-off values for normal magnesium levels across the published studies, methodological differences, and wide differences in the characteristics of the patients.
Hypokalemia and hypocalcemia are common in patients with hypomagnesaemia due to secondary increase in the renal loss of potassium and decrease in the parathyroid hormone, respectively.13 In our study, the incidence of hypocalcaemia was significant in patients with hypomagnesaemia compared to patient who had normal Mg levels. In concordance with our study, Limaye et al.17 found a significant association between hypocalcemia and hypomagnesemia. In a registry made by Safavi and Honarmand,18 the incidence of total hypocalcaemia was 52.1% in hypomagnesemic patients. They showed an association of hypocalcaemia with hypomagnesaemia. In a case series published by Baskaran et al.,19 the author found an association between hypomagnesaemia and hypocalcaemia in T.B. patients. The association between hypomagnesemia and hypokalaemia was further confirmed by Gupta et al.; in a prospective observational study over 200 patients; they showed that hypokalemia was higher in hypomagnesaemic patients than normomagnesaemic patients.
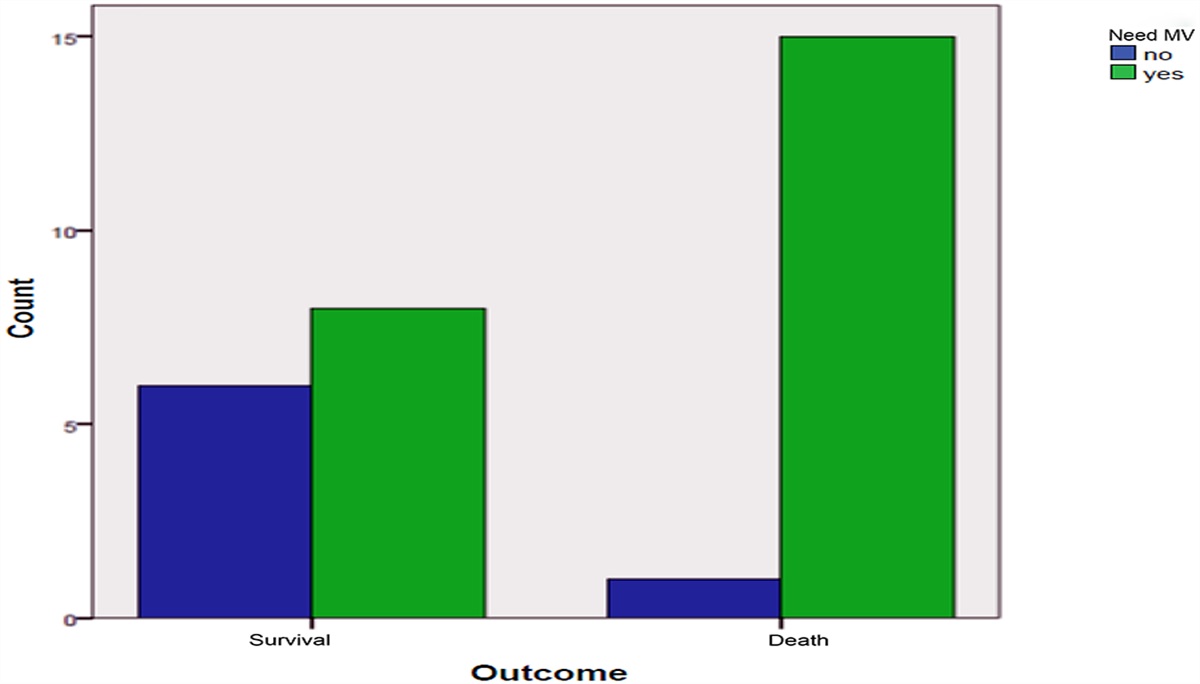
Low magnesium level is significant contributor to respiratory muscle weakness and failure. Thus, hypomagnesaemic patients are expected to have more difficult weaning from the ventilator and prolonged hospitalization.20 In our study, we found that patients with hypomagnesemia required ventilator support more frequently and for a longer duration; 60 (52.6%) patients of total 114 hypomagnesaemic patients required ventilator support with a mean period of 4.75 ± 3.29, compared to 54 (47.4%) patients did not require ventilator support. There was a statistical significance (P = .005). Our findings were in line with the findings of Sunil Kumar et al.,8 Limaye et al.,17 and Demircan et al.21 In contrast with our study, Soliman et al.,22 found that there was no significant association between hypomagnesaemia and mechanical ventilation need, duration, or ICU. This contrast is probably due to early correction of the serum magnesium levels.
On the other hand, we observed that mortality rate was not associated with hypomagnesaemia. There were 28 (24.6%) patients were not survived in hypomagnesaemic patients, compared to 26 (30.2%) non-survivors in the normomagnesaemic patients. In contrast to our study, Sunil Kumar et al.8 showed higher mortality in hypomagnesaemic patients, compared to normomagnesaemic patients. Likewise, Limaye et al.,17 in observational study included 144 patients found that mortality rate was 57.7% fatalities in hypomagnesaemic group, compared to 36.3% in the normomagnesaemic group with P < .05. Similarly, Upala et al.,23 collected data from six studies involving 1550 participants. There was a statistically significant higher risk of mortality in critically ill patients who had hypomagnesemia. We hypothesized that this contrast is due to inclusion of many comorbid patients with multiple risk factors.
In conclusion, hypomagnesemia is prevalent in ICU setting. We found that hypomagnesaemia significantly affected patients’ outcome as regard need of mechanical ventilation and ICU stay. Thus, routine monitoring of serum magnesium level is recommended in the ICU setting and prompt correction of its level is warranted.
ConclusionsHypomagnesemia is associated with significant increase in the risk of mechanical ventilation and prolonged ICU stay.
Recommendations:
1. The pivotal role of Magnesium levels in critically ill patients makes it essential to measured and treated to improve intensive care outcome. 2. More studies are required to validate the essential role and impact of Magnesium levels in critically ill patients.Study limitations:
1. Small sample size, which reduces the statistical validity of some of the differences between the groups. 2. The present study was not a randomized controlled trial, and a selection bias may have existed. 3. Long follow-up durations are needed to capture enough events to reveal more meaningful patterns in the data. References [1]. Dubé L, Granry J-C. The therapeutic use of magnesium in anesthesiology, intensive care and emergency medicine: a review. Can J Anaesth 2003;50(7):732–746. [2]. Gröber U, Schmidt J, Kisters K. Magnesium in prevention and therapy. Nutrients 2015;7(9):8199–8226. [3]. Guerrera MP, Volpe SL, Mao JJ. Therapeutic uses of magnesium. Am Fam Physician 2009;80(2):157–162. [4]. Gragossian A, Bashir K, Friede R. Hypomagnesemia. Book From StatPearls Publishing, Treasure Island (FL), 2018, PMID: 29763179 [5]. Xiong J, He T, Wang M, Nie L, Zhang Y, Wang Y, et al. Serum magnesium, mortality, and cardiovascular disease in chronic kidney disease and end-stage renal disease patients: a systematic review and meta-analysis. J Nephrol 2019;32(5):791–802. [6]. Lo Piano F, Corsonello A, Corica F. Magnesium and elderly patient: the explored paths and the ones to be explored: a review. Magnes Res 2019;32(1):1–15. [7]. Fairley J, Glassford NJ, Zhang L, Bellomo R. Magnesium status and magnesium therapy in critically ill patients: a systematic review. J Crit Care 2015;30(6):1349–1358. [8]. Kumar S, Honmode A, Jain S, Bhagat V. Does magnesium matter in patients of Medical Intensive Care Unit: a study in rural Central India. Indian J Crit care Med 2015;19(7):379–383. [9]. Dabbagh OC, Aldawood AS, Arabi YM, Lone NA, Brits R, Pillay M. Magnesium supplementation and the potential association with mortality rates among critically ill non-cardiac patients. Saudi Med J 2006;27(6):821–825. [10]. Fairley JL, Zhang L, Glassford NJ, Bellomo R. Magnesium status and magnesium therapy in cardiac surgery: a systematic review and meta-analysis focusing on arrhythmia prevention. J Crit Care 2017;42:69–77. [11]. Zafar MS, Wani J, Karim R, Mir M, Koul P. Significance of serum magnesium levels in critically ill-patients. Int J Appl Basic Med Res 2014;4(1):34. [cited 2021 Jan 9]. Available from: /pmc/articles/PMC3931212/?report=Abstract. [12]. Huijgen HJ, Soesan M, Sanders R, Mairuhu WM, Kesecioglu J, Sanders GT. Magnesium levels in critically ill patients: what should we measure? Am J Clin Pathol 2000;114(5):688–695. [13]. Hansen BA, Bruserud Ø. Hypomagnesemia in critically ill patients [Internet]. J Intensive Care BioMed 2018;6:1–11. [cited 2021 Jan 9]. Available from: https://doi.org/10.1186/s40560-018-0291-y. [14]. Whang R, Oei TO, Aikawa JK, Watanabe A, Vannatta J, Fryer A, et al. Predictors of clinical hypomagnesemia: hypokalemia, hypophosphatemia, hyponatremia, and hypocalcemia. Arch Intern Med 1984;144(9):1794–1796. [15]. Wong ET, Rude RK, Singer FR, Shaw ST. A high prevalence of hypomagnesemia and hypermagnesemia in hospitalized patients. Am J Clin Pathol 1983;79(3):348–352. [16]. Hayes JP, Ryan MF, Brazil N, Riordan TO, Walsh JB, Coakley D. Serum hypomagnesaemia in an elderly day-hospital population. Ir Med J 1989;82(3):117–119. [17]. Limaye CS, Londhey VA, Nadkar MY, Borges NE. Hypomagnesemia in critically ill medical patients. J Assoc Physicians India 2011;59(1):19–22. [18]. Safavi M, Honarmand A. Admission hypomagnesemia—impact on mortality or morbidity in critically ill patients. Middle East J Anesthesiol 2007;19(3):645–660. [19]. International Journal of Current Research and Review (IJCRR) [Internet]. [cited 2021 Jan 9]. http://ijcrr.com/article_html.php?did=937 [20]. Islam MM, Faruq MO, Asaduzzaman M, Sultana A, Mollick UK. Hypomagnesemia is associated with increase in mortality and morbidity in ICU: Can serum magnesium level be used as prognostic marker in critically ill ICU admitted patients? Bangladesh Crit Care J 2017;5(2):77–82. [21]. Demircan F, Altun Y, Kilinc F. Hypomagnesemia in Internal Care Unit. Int J Basic Clin Stud 2013;1(1):180–189. [22]. Soliman HM, Mercan D, Lobo SSM, Mélot C, Vincent JL. Development of ionized hypomagnesemia is associated with higher mortality rates. Crit Care Med 2003;31(4):1082–1087. [23]. Upala S, Jaruvongvanich V, Wijarnpreecha K, Sanguankeo A. Hypomagnesemia and mortality in patients admitted to intensive care unit: a systematic review and meta-analysis. QJM [Internet] 2016;109(7):453–459. [cited 2021 Jan 9]. Available from: https://academic.oup.com/qjmed/article-lookup/doi/10.1093/qjmed/hcw048.
留言 (0)