
Remember me
Traumatic brain injury (TBI) is one of the most common causes of longevity disability and about 30% of worldwide death is related to injury. It is defined as an injury due to any external force resulting in disrupting the brain normal function. It is associated with high economic burden and disturbance of the quality of life.1 The brain trauma foundation guidelines for the management of TBI highlighted the significance of hypoxemia and hypoperfusion prevention that may occur secondary to the injury.2 Also, prevention of the damage triggered by free radicals, calcium-mediated injury, neurotransmitters, and inflammatory cascade is essential after head injury as they are associated with increasing the morbidity and mortality rates among head trauma patients.3
Administration of adrenergic receptor blockers could blunt the inflammatory and immune changes related to traumatic brain injury resulting in reducing the mortality rate.4
Early propranolol administration may possibly compensate the catecholamines elevation impacting the sympathetic hyperactivity during the first week post trauma.5,6 Also, it can penetrate the blood-brain barrier and might improve the post TBI outcomes.7,8
Several studies hypothesized that the survival rates were improved in TBI patients who were administrated β-blockers, but the β-blockers impact on functional outcome is poorly observed. This prospective randomized-study aimed at investigating whether empiric early administration of propranolol in patients with moderate-to-severe TBI impacts outcomes define it.
2 Methods 2.1 Study designThis is a prospective study that was conducted at General ICU Alexandria Main University Hospital among 100 patients who were diagnosed with isolated traumatic brain injury GCS< 10 and head [AIS] score, 3–5. The patients were divided into two equal groups according to either received B-blockade or not. Patients not receiving β-blockers constituted the control group in this study. The B-blockade group received propranolol 1 mg every 8 hours intravenously for 1 week. The patients suffering from polytrauma patient, previous CVA-dementia-Alzheimer, brain tumor and BB hypersensitivity or contraindications were excluded from the study.
2.2 Data collectionPatients’ data and full history were reviewed charts to determine demographics data such as patient's age, gender, and history of medications. All the patients were subjected to complete physical examination, basal neurological examination, radiological investigation and laboratory investigation to determine the CBC, renal function, liver function, ABG, and coagulation profile. TBI was evaluated using Abbreviated Injury Scale (AIS)9 and patients with a head AIS score of 3 or greater attributed to their intracranial injury were included. Also, the post-rescuscitation Glasgow Coma Scale (GCS) was used to determine the severity of TBI as patients are classified as having mild if the score between 13 and 15, moderate if the score between 9 and 12 and severe if the score is less than 9.10 Finally, all the patients were followed up for 3 weeks to assess the complications and outcomes of BB administration including its impact on ICU mortality, length of ICU stay, and the GCS increase.
2.3 Ethical approvalThe study was approved by the ethical committee of Faculty of Medicine, Cairo University and the Alexandria Main University Hospital. An informed consent was given by the included patients or their families. All the included patients were treated according to the ethical standards of the responsible committee on human experimentation.
2.4 Statistical analysisThe data were processed using the Statistical Package for Social Sciences (SPSS, version 20.0). The variables were shown as number and percentages while quantitative data were distributed as mean and standard deviation. Chi-square test was used to compare between different variables of the two groups. Significance of the obtained results was judged at the 5% level.
3 Results 3.1 Demographics of included subjectsTable 1 shows the demographics of the studied groups, the mean age in patients received beta blocker was 36.12, while in patients without beta blocker was 36.88, on comparing the two groups regarding age, it was found that there was no significant difference between the two groups. The majority of the subjects of both groups were males with no significant difference between the two groups regarding gender.
Table 1 - Comparison between the two studied groups regarding demographic data Group I Beta blocker (+) Group II Beta blocker (−) P Age .719 Mean 36.12 36.88 S.D. 10.42 10.65 Gender No % No % 1.0 Male 46 92.0 46 92.0 Female 4 8.0 4 8.0 Total 50 100.0 50 100.0The mean of ICU stay in group I was 10.06, while in group II was 10.02 days. The mechanical ventilation in days in group I was 5.28, while in group II was 5.30 days, there was no significant difference between the two groups regarding the ICU stay and duration mechanical ventilation (P> .05 write it) (Table 2).
Table 2 - Comparison between the two studied groups regarding ICU stay and mechanical ventilation stay (days) Group I Beta blocker (+) Group II Beta blocker (−) P ICU stay (days) 10.06 ± 3.92 10.02 ± 3.56 .958 Mean ± S.D. Mechanical ventilation (days) 0.00–21.00 2.00–17.00 .980 Range 5.28 ± 4.57 5.30 ± 3.37 Mean ± S.D.There was no significant difference between the two groups regarding GCS after administration of β-blockers (Table 3).
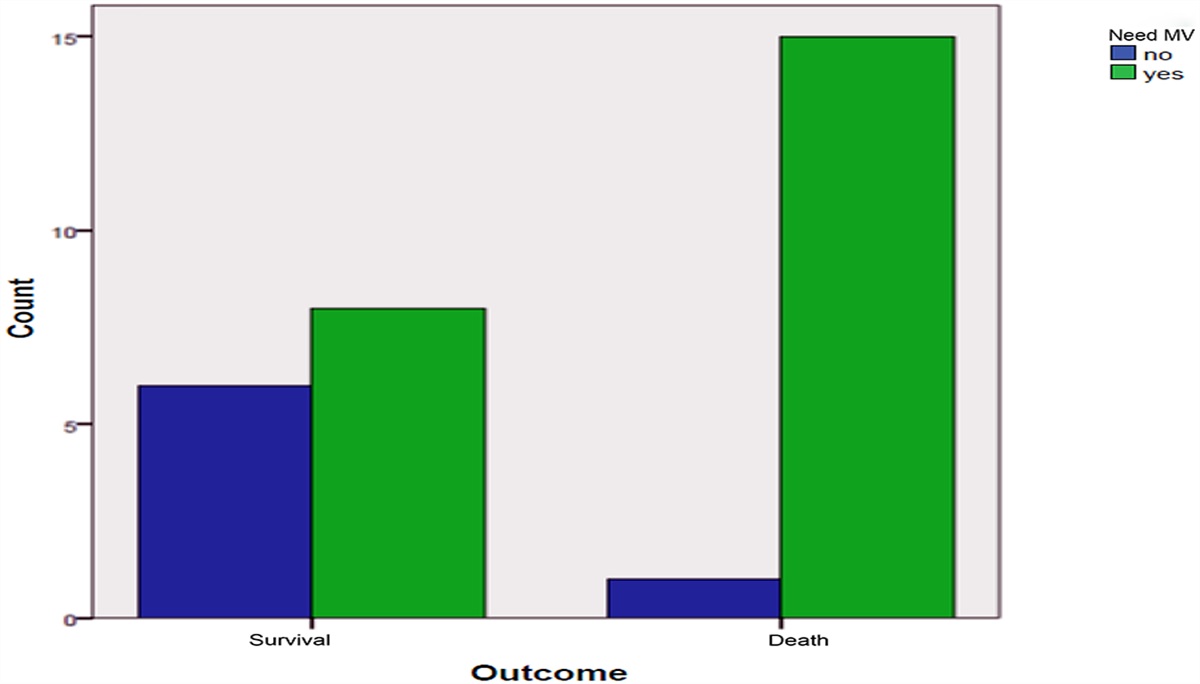
Table 3 - Comparison between the two studied groups regarding GCS Group I Beta blocker (+) Group II Beta blocker (−) GCS Range 7.00–15.00 6.00–15.00 Mean ± S.D. 9.84 ± 2.11 10.06 ± 2.37 P 0.626Table 4 shows that the mortality was significantly lower in BB group than the non BB group.
Table 4 - Comparison between the two studied groups regarding mortality Group I Beta blocker (+) Group II Beta blocker Mortality Number % Number % No 48 96.0 41 82.0 Yes 2 4.0 9 18.0 X2 5.005 P 0.026∗∗P < 0.05 to be significant.
The mean systolic blood pressure among BB group was 135.28 and the non BB group was 133.96 mmHg. The heart rate was 114.54 beats in BB group and 116.28 in non BB group (Table 5).
Table 5 - Comparison between the two studied groups regarding Systolic BP and Heart rate Group I Beta blocker (+) Group II Beta blocker (-) P Systolic BP Range 107.00–152.00 122.00–155.00 .426 Mean ± S.D. 135.28 ± 9.31 133.96 ± 7.04 Heart rate Range 87.00–128.00 95.00 135.00 .376 Mean ± S.D. 114.54 ± 8.79 116.28 ± 10.65There was no significant difference between the studied groups regarding BP and heart rate.
3.5 Beta-blocker complicationsAs presented in Table 6, only 3 cases in group I had hypotension, and no one of the two groups had other complication. There was no significant difference between the studied groups regarding beta-blocker complications.
Table 6 - Comparison between the two studied groups regarding hypotension, Bradycardia, bronchospasm, heart failure and other BB complication Group I Beta blocker (+) Group II Beta blocker (−) Number % Number % P Hypotension No 47 94.0 50 100 .121 Yes 3 6.0 0 0 Bradycardia No 50 100 50 100 – Yes 0 0 0 0 Bronchospasm No 50 100 50 100 – Yes 0 0 0 0 Heart failure No 50 100 50 100 – Yes 0 0 0 0 Other BB complication No 50 100 50 100 – Yes 0 0 0 0Table 7 presented the show the comparison between the two studied groups regarding type of hemorrhage.
Table 7 - Comparison between the two studied groups regarding type of hemorrhage Group I Beta blocker (+) Group II Beta blocker (−) Number % Number % P Extradural hemorrhage 4 8.0 3 6.0 .695 Subdural hemorrhage 13 26.0 12 24.0 .817 Subarachinoid hemorrhage 6 12.0 7 14.0 .766 Brain contusion 4 8.0 3 6.0 .695 Intraparenchymal hemorrhage 2 4.0 4 8.0 .399 combined hemorrhage 19 38.0 18 36.0 .835 DIA 2 4.0 3 6.0 .646Four patients (8.0%) in group I and 3 patients (6.0%) in group II suffered from Extradural hematoma. About 13 patients (26.0%) in group I and 12 patients (24.0%) in group II suffered from subdural heamatoma. Subarachinoid hemorrhage was presented in 6 patients (12.0%) in group I and 7 patients (14.0%) in group II. Also, 4 patients (8.0%) in group I and 3 patients (6.0%) in group II suffered from Brain contusion. Intraparenchymal hemorrhage was found in 2 patients (4.0%) in group I and 4 patients (8.0%) in group II. Among BB group, 19 patients (38.0%) suffered from combined hemorrhage while 18 patients (36.0%) in group II suffered from combined hemorrhage. Also, DIA was diagnosed among only 2 patients (4.0%) in group I and 3 patients (6.0%) in group II, there was no significant difference between the two groups regarding the type of hemorrhage.
3.7 Incidence of craniectomyAbout 15 patients (30.0%) undergone Craniectomy in group I and 24 patients (48.0%) undergone Craniectomy in group II. which was significantly higher in group II than group I (P< .05) (Table 8).
Table 8 - Comparison between the two studied groups regarding craniectomy Group I Beta blocker (+) Group II Beta blocker (−) Number % Number % P Craniectomy Yes 15 30.0 24 48.0 .065 No 35 70.0 26 52.0Table 9 shows that 7 patients in group II needed vasopressor which was significantly higher than group I receiving BB.
Table 9 - Comparison between the two studied groups regarding need for vasopressor Group I Beta blocker (+) Group II Beta blocker (−) Need for vasopressor Number % Number % P Yes 1 2.0 7 14.0 0.026∗ No 49 98.0 43 86.0 Total 50 50∗P < 0.05 to be significant.
Table 10 shows that the mean GOSE in the two studied groups after one month of TBI was 2.85 in group I and 2.35 in group II with no significant difference between the two studied groups.
Table 10 - Comparison between the two studied groups regarding GOSE Group I Beta blocker (+) Group II Beta blocker (−) P GOSE score Range 1–8 1–8 .325 Mean ± S.D. 2.85 ± 2.4 2.35 ± 2.11Table 11 shows the regression analysis to determine the risk factors of mortality, it was found that the most significant factors which affect the mortality was type of treatment (Beta blocker), the male gender and lower GCS score (Table 12).
Table 11 - Regression analysis to determine the risk factors of mortality Anova∗ Model Sum of squares Df Mean square F Sig. 1 Regression 3.939 6 0.656 10.434 0.000† Residual 5.851 93 0.063 Total 9.790 99∗Dependent variable: mortality.
†Predictors: (Constant), ED heart rate, gender, groups, age, GCS, ED systolic BP.
aDependent variable: mortality.
∗P < 0.05 to be significant.
The current study showed that the usage of B-blockade in the early phases of isolated traumatic brain injury is associated with blocking the hyperactivity of sympathetic adrenoceptors thus decreasing the mortality rates and better functional outcomes in comparison with the control group who were not administrated BB.
We noted that the demographics’ of the studied groups showed no significant difference. Also, there was no significant difference between the studied groups regarding the ICU stay and mechanical ventilation stay days. However, Chen et al.,11 stated that the usage of β-blocker therapy was related to increasing the ICU stay, longer ventilation periods and high infection rates.
The study indicated that there was no significant difference between the studied groups regarding the BB complications including hypotension, heart failure, and bradycardia. Correspondingly, other studies showed that blood pressure and heart rate showed no significant difference between the two studied groups either administrated BB or not.12–15
This study revealed that on the comparison between the two studied groups, the mortality rates were significantly lower among patients who administrated BB. Consistently, the survival rates among beta-blockade traumatic brain injury patients were significantly improved.16 On the same respect Mohseni et al.,17 showed that in-hospital mortality was significantly increased by 5-fold among TBI patients who did not administrate early β -blockers during their admission. Also, two meta-analysis demonstrated that beyond the complications of β-blockers, they are effective in reducing the in-hospital mortality rates among TBI patients.11,16
B-blockade mechanism of action during injury is still a debate but it can block the hyperactive sympathetic adrenoceptors. After traumatic brain injury, the sympathetic storm could worsen the neurological outcome thus increasing the in-hospital mortality3,5,18–20 as the sympathetic hyperactivity is could enhance the cerebral vasoconstriction resulting in increasing the intracranial pressure and the incidence of edema that reduce the brain perfusion and oxygenation thus increase the overall disability and mortality rates.21,22
Also, the blockade could lessen the vasospasm induced by intracerebral posttraumatic catecholamine induced vasospasm, thus decreasing the occurrence of local ischemia.23 The BB could stimulate the adrenoreceptors in the brain which reduce the oxygen consumption and metabolism of the brain.6,24
Systemically, it could also protect the susceptible end organs as heart from damage with its cardioprotective effects thus decrease the incidence of rhythm disturbances and myocardial necrosis after brain trauma.25 Furthermore, beta blockade could decrease the occurrence of myocardial oxygen demand, tachycardia26 and improved oxygen utilization.27
However, other large studies associate preinjury beta blockade with higher mortality in patients without head injury.28 Likewise, a large study of trauma patients with preexisting cardiac disease showed that beta blocker usage is associated with increasing the relative risk by 2 fold when compared to non BB administrated patients and could also be associated with failure of a patient to respond to normal resuscitation.29 It has been proposed that beta blockade may render trauma victims not sufficient to increase the cardiac output properly to preserve the tissue perfusion.28
Interestingly, the incidence of undergoing craniectomy was significantly higher among group II than those who administrated BB but there was no significant difference between the studied groups regarding the incidence of hemorrhage and other clinical outcomes. On the other hand, a recent study showed that the risk of poor long-term functional outcome was more than doubled in non-β-blocked controls.12
As for the logistic regression studies, it was found that the most significant factors which effect on mortality was type of treatment (Beta blocker), the male gender and GCS score. Accordingly, diminished Glasgow Coma Scale (GCS) score on admission was associated with increasing the rates of in-hospital mortality.30,31 On the same respect, BB was identified as protective among head injury patients lowering the mortality rates by 65% in comparison with non B-blocked patients.32 Inaba et al.16 declared the protective effect of BB among elderly TBI patients which decreased the mortality rates by 60%.
On contrast, factors associated with increased mortality among in hospital traumatized patients were age and severity of brain trauma but showed no significant difference among patients who either received BB or not.13
The present study has some strengths as it examined the factors related to BB complications and its effects on other neurological functions.
Nevertheless, there are several limitations to the study. First, we chose to perform a case-control study, and the size of the study population was limited by a relatively small number of in-hospital deaths. Also, time limitation as the follow up was done for only 1 month were not sufficient for following up patient's GCS.
5 ConclusionThis early administration of B-blockade among isolated traumatic brain injury patients could reduce the in hospital mortality rate and decrease the rate of craniectomy suggesting that BB are essential for survival and functional recovery among TBI patients. Further research is encouraged to examine the mechanisms underlying this effect.
References [1]. Ma VY, Chan L, Carruthers KJ. Incidence, prevalence, costs, and impact on disability of common conditions requiring rehabilitation in the United States: stroke, spinal cord injury, traumatic brain injury, multiple sclerosis, osteoarthritis, rheumatoid arthritis, limb loss, and back pain. Arch Phys Med Rehabilit 2014;95(5):986–995. e1. [2]. BTF. Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons: Guidelines for the management of severe traumatic brain injury. J Neurotrauma 2017;24(Suppl 1):S1–106. [3]. Heffernan DS, Inaba K, Arbabi S, Cotton BA. Sympathetic hyperactivity after traumatic brain injury and the role of beta-blocker therapy. J Trauma 2010;69(6):1602–1609. [4]. Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic brain injury-related emergency department visits, hospitalizations, and deaths: United States, 2007 and 2013. MMWR Surveill Summ 66: 2017(9):1–16. [5]. Cotton BA, Snodgrass KB, Fleming SB, et al. Beta-blocker exposure is associated with improved survival after severe traumatic brain injury. J Trauma 2007;62(1):26–33. discussion-5. [6]. Ferry B, Parrot S, Marien M, Lazarus C, Cassel JC, McGaugh JL. Noradrenergic influences in the basolateral amygdala on inhibitory avoidance memory are mediated by an action on alpha2-adrenoceptors. Psychoneuroendocrinology 2015;51:68–79. [7]. Murry JS, Hoang DM, Barmparas G, et al. Prospective evaluation of early propranolol after traumatic brain injury. J Surg Res 2016;200(1):221–226. [8]. Bible LE, Pasupuleti LV, Alzate WD, et al. Early propranolol administration to severely injured patients can improve bone marrow dysfunction. J Trauma Acute Care Surg 2014;77(1):54–60. discussion 59–60. [9]. Lesko MM, Woodford M, White L, O’Brien SJ, Childs C, Lecky FE. Using Abbreviated Injury Scale (AIS) codes to classify Computed Tomography (CT) features in the Marshall System. BMC Med Res Methodol 2010;10:72. [10]. Gradisek P, Osredkar J, Korsic M, Kremzar B. Multiple
Comments (0)