
Remember me
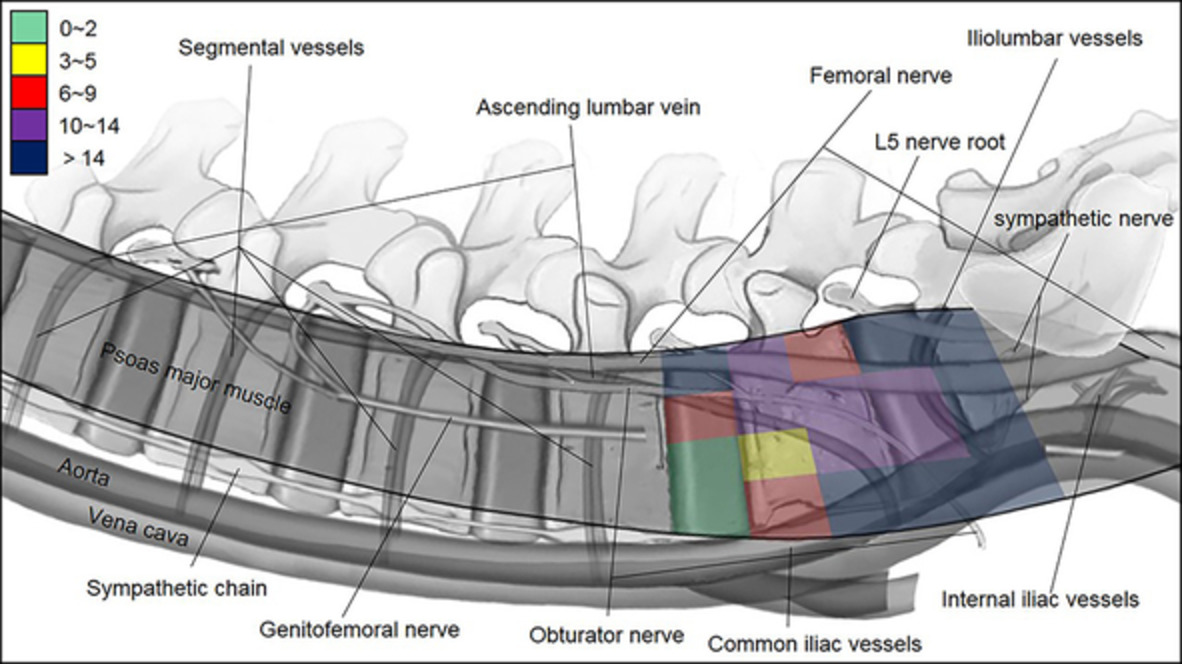
Cortex violation of the ilium would occur when S2AI screws were placed by free hand technique. The cortical breach of an S2AI screw may result not only in decrease fixation strength but also potentially injury of the major vessels, particularly the internal iliac artery with an anterior breach and the superior gluteal artery with a caudal breach7. O'Brien and colleagues reported a 15% rate of posterolateral cortex violation in 10 cadaveric specimens11. Shillingford and colleagues found an overall 7% rate of posterior cortical perforation and a 1% rate of anterior cortex violation12. Posterolateral cortex violation did not endanger any major neurovascular structures. Although anterior pelvic violation and inferior screw violation were rare, they can result in severe complications and devastating consequences. Anterior violations can result in injuries of important visceral or neurovascular structures located anterior to the pelvis13. Moreover, inferior screw violation into the sciatic notch may result in injuries of sciatic nerve, pudendal nerves, or internal pudendal vessels as they pass over and under the piriformis muscle within the notch14. In recent years, several techniques were used for S2AI screw placement, including navigation, freehand technique, and TGT. However, freehand technique obtained popularity because of convenience. Some limitations of navigation and TGT, including expense and complexity, limited them being widely use. In this study, to further enhance the accuracy or S2AI screw placement by freehand technique, the authors adopted ball tip technique for S2AI screw placement. Ball tip technique applied in thoracic pedicle screw insertion for adolescent idiopathic scoliosis patients was initially described by Kota Watanabe9. They found that ball tip technique could enhance the accuracy of pedicle screw placement in clinical and cadaveric study. Whether the ball tip technique could be feasibly used for S2AI screw insertion and increase the accuracy of S2AI screw placement has not been, to our knowledge, studied previously in the available literature. The results of our study demonstrated an overall 5% rate of cortical perforation in ball tip group, which significantly increases the accuracy compared with the result of 17.9% rate of cortical perforation in conventional freehand group. However, neither of the two different techniques gave rise to major neurologic or vascular complications.
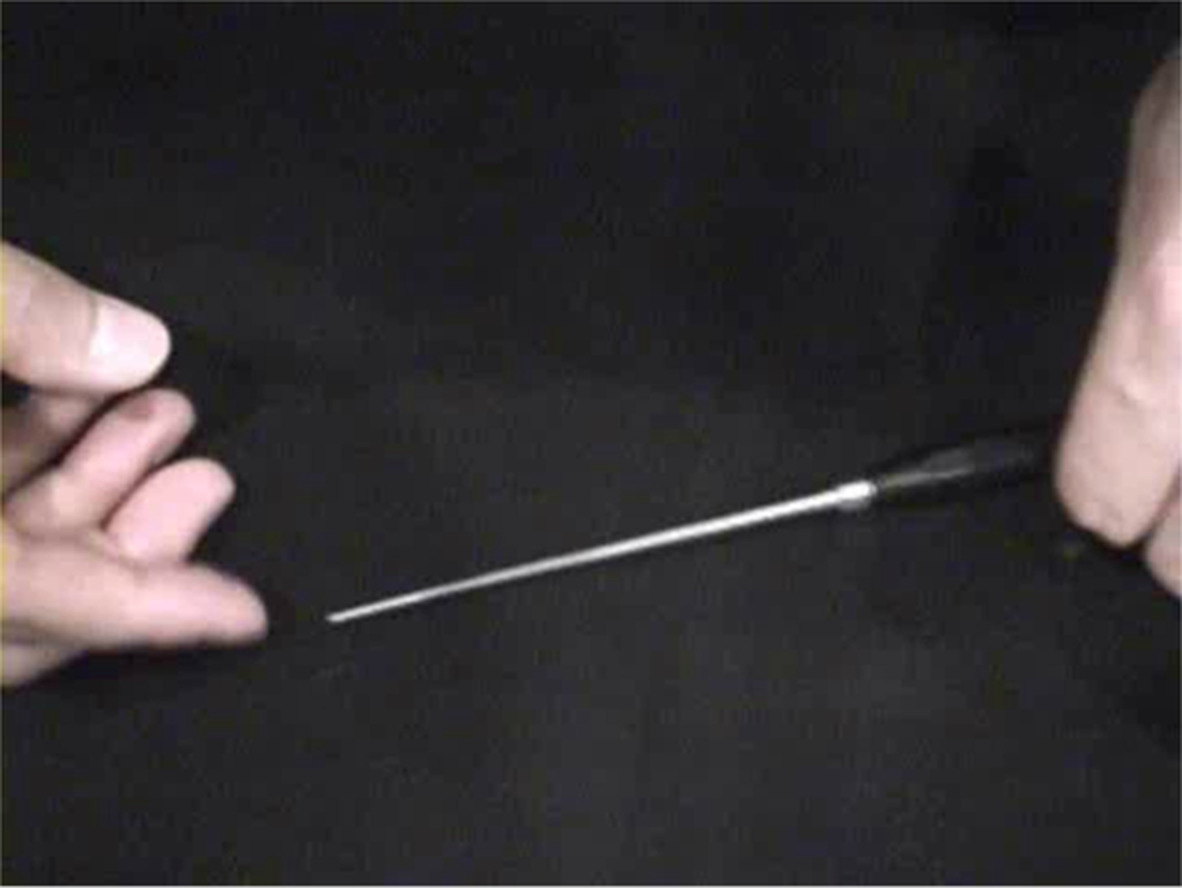
Furthermore, compared with conventional freehand technique, ball tip technique decreased the frequency of using C-arm, which would significantly reduce radiation exposure to the patient and surgeon. In the conventional freehand technique, the surgeon had to find the teardrop and ensured the guided probe and the inserted screw inside the teardrop under repeated intraoperative fluoroscopy. On the contrary, in procedure of ball tip technique, the surgeon took the special probe with characteristics of semi-flexible metal shaft to find the track hole in the cancellous channel automatically, rather than having to continue watching the probe inside the teardrop, which obviously reduces the frequency of using C-arm. Consequently, the efficacy of S2AI screw insertion was significantly improved. Especially for some patients with severe lumbosacral deformity and rotational pelvis, ball tip technique significantly decreased frequency of intraoperative fluoroscopy and simplified surgical procedure (Figs 4-6).

Typical case 1 managed by ball tip technique. A 44-year-old female presented severe congenital thoracolumbar deformity with a morphological abnormality of right sacroiliac joint, in which the hypertrophy is obvious under the overload stress. Also, the pelvis is asymmetrical with the right side being anteriorly rotational (A, B). The anomaly made the S2AI screw insertion by conventional free hand technique to be difficult. Surgeon conducted the ball tip technique to solve this problem perfectly. Postoperative X-rays showed the satisfactory correction and good sagittal and coronal realignments with a sacropelvic fixation (C, D). Postoperative CT scan indicated the perfect positions of S2AI screws bilaterally in the axial and sagittal plates of screws without any cortex breach (E–H).

Typical case 2 managed by ball tip technique. A 60-year-old female presented trunk shift. She underwent an anterior cervical discectomy and fixation (ACDF) at local hospital 3 years ago. Preoperative X-rays showed a coronal imbalance. (A, B) Surgeon adopted the ball tip technique for S2AI screw placement. Postoperative X-rays showed the satisfactory correction and good sagittal and coronal realignments with a sacropelvic fixation (C, D). Postoperative CT scan indicated the perfect positions of S2AI screws bilaterally in the axial and sagittal plates of screws without any cortex breach (E–H).
 Typical case 3 managed by ball tip technique. A 68-year-old male presented severe back pain and weakness of low limbs. Rigid lumbar scoliosis. He underwent an anterior cervical discectomy and fixation (ACDF) at local hospital 5 years ago. Preoperative X-rays showed a rigid lumbar scoliosis and asymmetric pelvis (A–D). Surgeon adopted the ball tip technique for S2AI screw placement. Postoperative X-rays showed the satisfactory correction and good sagittal and coronal realignments with a sacropelvic fixation (Fig. 3C, D). Postoperative CT scan indicated the perfect positions of S2AI screws bilaterally in the axial and sagittal plates of screws without any cortex breach (E–H).
Typical case 3 managed by ball tip technique. A 68-year-old male presented severe back pain and weakness of low limbs. Rigid lumbar scoliosis. He underwent an anterior cervical discectomy and fixation (ACDF) at local hospital 5 years ago. Preoperative X-rays showed a rigid lumbar scoliosis and asymmetric pelvis (A–D). Surgeon adopted the ball tip technique for S2AI screw placement. Postoperative X-rays showed the satisfactory correction and good sagittal and coronal realignments with a sacropelvic fixation (Fig. 3C, D). Postoperative CT scan indicated the perfect positions of S2AI screws bilaterally in the axial and sagittal plates of screws without any cortex breach (E–H).
Some surgeons who used conventional freehand technique reported that only 5% of the S2AI screws demonstrated moderate to severe cortical breaches, all of which perforated the pelvis posteriorly and all only involved the distal part of the screw tip depending on the horizontal and caudal angles12; but in an anther study, the rate of cortex penetration was high, reaching 15%11. In this study, stricter evaluation criteria were adopted in which mild to severe cortex breaches were considered as inaccurate insertion. In ball tip technique group, the total rate of penetration was 5.7% (4/70) but there was no moderate to severe cortex breach. In conventional freehand group, although the total rate of penetration was 17.9%, the rate of moderate to severe cortex breaches was 10.7% (6/56). Our result further demonstrated that ball tip technique enhanced the accuracy of S2AI screw placement, especially avoiding moderate to severe penetration.
Ball Tip Technique Reduces Time Cost for S2AI Screw PlacementIn this study, the time cost between ball tip technique and conventional freehand technique were also compared, our result demonstrated that ball tip technique could statistically decrease the time cost of screw placement from 20.2 ± 8.6 min to 9.8 ± 4.5 min. Less surgical time means less intraoperative blood loss and lower rate of wound infection. Less operation time may also decrease surgeon fatigue, improve concentration, and potentially correlate with positive patient outcomes15.
Limitations of Current StudyThere were limitations to this study. The ball tip technique was not generalized in pediatric patients, whether this technique could be used in pediatric patients needs to be further investigated. This study is a small series in a single center and the patients were not randomized for both techniques in this retrospective study. Limited results were obtained from this study and future studies may benefit from randomizing patients divided into ball tip vs conventional freehand technique. Additionally, although our result demonstrated that the ball technique is useful and reliable for S2AI screw placement in this study, it still needs to be emphasized that it may not be helpful to a surgeon who has no experience in placing S2AI screws, since a mistake in the identification of starting point could lead to missed screw placement even if the ball tip technique is used.
ConclusionBall tip technique for S2AI screw placement is not only a reliable but also a practical technique. This technique significantly enhances the accuracy of S2AI screw placement and improves the efficacy by reducing the time cost for S2AI screw placement in spine surgery involved in sacropelvic unit compared with conventional freehand technique.
Comments (0)