
Remember me
From the time that Mayer1 and Ozgur et al.2 described two different minimally invasive lumbar interbody fusions through the retroperitoneal approach, in 1997 and 2006, respectively, various spinal surgery techniques, such as extreme lateral interbody fusion and oblique lumbar interbody fusion, have evolved. Although they have slight differences in surgical methods or approaches, they all operate by the same fusion window, that is, the lateral part of the intervertebral disc. Therefore, they can be uniformly classified as lateral lumbar interbody fusion (LLIF).
The LLIF technique has prevailed due to the advantages of minimal invasion and less bleeding. But the challenge that remains is to reduce the approach-related complications during surgery. In a meta-analysis study of 1874 patients treated via the prepsoas approach and 4607 treated with the transpsoas approach, Walker et al.3 reported similar complications (27.6% transpsoas vs 31.4% prepsoas), which suggests that the complication rate cannot be reduced by only altering the surgical approach. Neural and vascular injuries sustained during the penetration and retraction of the psoas muscle have become well-known complications associated with these surgical approaches4, 5.
Obviously, this is related to the complex distribution of nerves and blood vessels around the psoas major muscle. So a thorough understanding of the anatomical complexity surrounding the psoas muscle is crucial. Bogduk et al.6 described the psoas muscle as a continuous attachment to the vertebral column, consisting of a series of overlapping segmental fascicles and the superficial fascicles seldom arise from the L5 vertebral body. This means that there is a potential cleft beneath the psoas major muscle on the side of L5 vertebra, within which, neurovascular damage often occurs during LLIF. In fact, many anatomical structures, such as great vessels, ascending lumbar vein, iliolumbar vein, obturator nerve and femoral nerve, are distributed in this cleft, and the adjacent relationship of them is complex. These anatomical structures are precisely the main risk factors of LLIF. To our knowledge, there is very little information available regarding the cleft and its contents, in particular, its influence on LLIF surgery.
Previous studies have attempted to calibrate these risk factors by using vertebral bodies and discs as landmarks to identify a safe zone for surgery7-11. Unfortunately, vertebrae discs and neurovascular structures are often concealed by the psoas major and it is impossible to directly identify these beneath the muscle. Therefore, using the psoas major as a reference may have more practical significance.
Based on this premise, we studied the anatomical features in this region, that is, the region between the L5 vertebra and the psoas major, and tried to achieve the following purposes: (i) to confirm the cleft, which is between the L4 vertebra and the psoas muscle, exists, and clarify the relationship between the psoas muscle, neurovascular structures and vertebrae (intervertebral discs) in detail; (ii) to further propose the methods to avoid damage to the neurovascular structures in the CPM during the LLIF procedure; and (iii) to develop a novel grid system, which can be used to divide the psoas major in order to analyze the neurovascular distribution, and therefore has practical value in LLIF surgery.
Materials and Methods Cadaveric Anatomical DissectionSix fresh-frozen cadavers were studied, of which four were male and two female, with mean age of 69.1 ± 7.4 years (from 58 to 77 years) and height of 166.2 ± 8.9 cm (from 152 to 177 cm) (Table 1). The cadavers were placed in a right lateral decubitus position and a skin incision was made from the pubic symphysis, along the iliac margin to the posterior axillary line, then up to the costal arch and cut off at the T11 and T12 ribs. The abdominal muscles were cut and the abdominal contents ventrally reflected. The retroperitoneal space was identified and defined.
TABLE 1. General data of cadaver specimens Variables Emergence Total Data (occurrence rate) Number of specimens 6 Sex Male 4 Female 2 Age 69.1 ± 7.4 years Height 166.2 ± 8.9 cm Easily variable anatomical structures GFN 6 6 100% Psoas minor muscle 4 6 66.7% ALV 5 6 83.3% Iliolumbar vessels 6 6 100% ALV, ascending lumbar vein; GFN, genitofemoral nerve.The psoas major was located in the center of the visual field. The position and course of the genitofemoral nerve (GFN) and psoas minor, running on the surface of the psoas major, were observed and recorded. The psoas muscle was transected at the lower edge of the L4 vertebrae, and reflected to the distal end. The distribution of anatomical structures and their relationship with psoas major were observed and recorded.
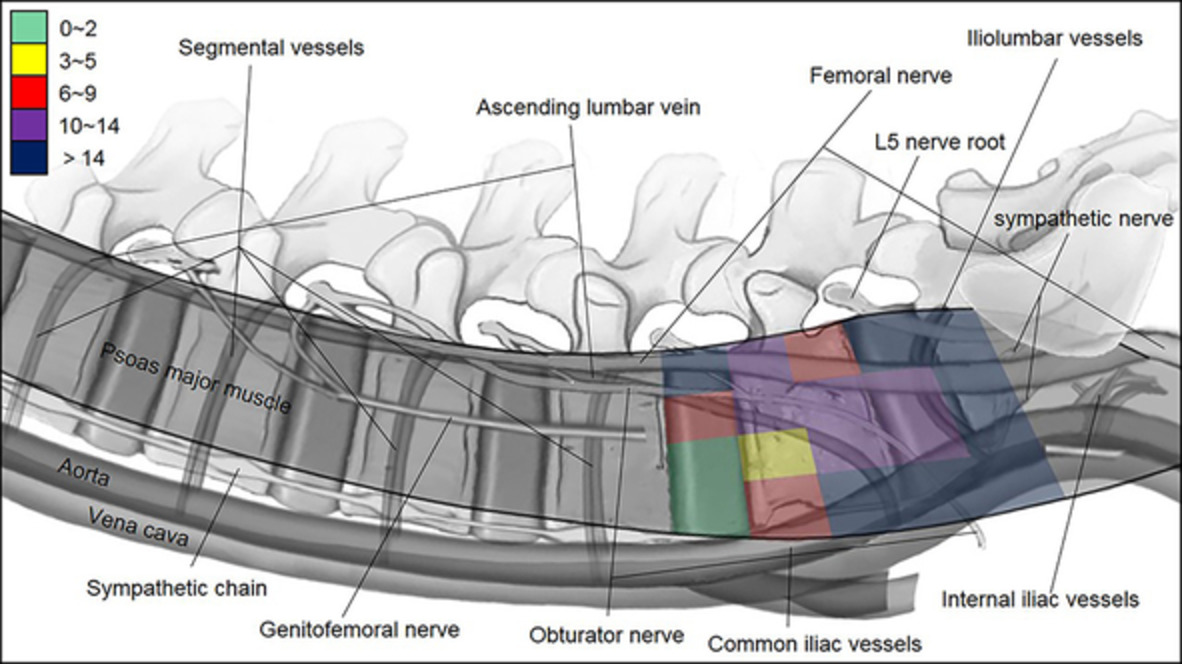
Grid StudyThe psoas major surface was divided homogeneously into four parts, from the anterior border of the psoas major to the transverse process. The cranial-to-caudal division was from the lower edge of the psoas muscle attachment on the L4 vertebrae to the upper part of the S1 vertebrae, and was divided into five segments: segment L45 (L4/5 disc), segment L5-upper (upper half of the L5 vertebrae), segment L5-lower (lower half of the L5 vertebrae), segment L5/S1 (L5/S1 disc), and segment S1-upper (upper part of the S1 vertebrae). Accordingly, a total of 20 grids were generated on the psoas major surface, and the neurovascular structures in each grid were identified, as shown in Fig. 1.

Grid system of the CPM. The psoas major surface was divided into four parts in anterior-to-posterior and five segments in cranial-to-caudal, so that 20 grids were generated. Obviously, there were hidden anatomical structures beneath the muscle in each grid area, which was difficult to detect in the actual operation.
Results MorphologyIn all six cadavers, the GFN was found to emerge from the surface of the psoas major, and descend along the anterior surface; it did not bifurcate. The psoas minor muscle emerged in four of six cases (66.7%), and descended anteriorly along the GFN.
On the lateral vertebrae surface, at L4 and above, the psoas major was firmly attached to the proximal and distal ends of each vertebra, but on the L5 vertebrae surface, there was no adhesion. A cleft filled with loose connective tissue and neurovascular structures was observed beneath the psoas major at mid-L4 and below, in all six specimens; we termed it the cleft of psoas major (CPM) (Figs 2 and 3). When the psoas muscle was transected and reflected in the lateral decubitus position, we observed that the proximal boundary of the CPM was composed of the lower edge of the psoas major and fascicle from the L4 vertebrae, but no clear boundary could be determined at the caudal end, which gradually extended to the pelvis. Therefore the sacral alar can be regarded as the distal end of the CPM. The posterior wall of the CPM is composed of the transverse process and inter-transverse ligament. The anterior side is open, therefore the anterior margin of psoas major can be defined as the anterior boundary of the CPM (Fig. 4). Beneath psoas major, a thin layer of fascia lies on the surface of the CPM.

Pattern of the CPM. The forming reason of the cleft is psoas major muscle is not attached to lumbar 5 vertebrae. The small image at the top right shows its details with viewing direction of blue arrow. And many important structures are inside, such as ascending lumbar vein, obturator nerve and so on.

Ventral view of the CPM. (1) Psoas major muscle, (2) attachment of psoas major on L4, (3) sympathetic chain, (4) iliolumbar vessels, (5) external iliac vein, (6) common iliac artery, (7) acsending lumbar vein, and (8) folded peritoneum.

Transversal pattern of the CPM. The psoas major is its ceiling, the lateral wall of lumbar its bottom, the transverse process and inter-transverse ligament the posterior wall. But the anterior side is open. The cleft fills with loose connective tissue and many neurovascular structures.
Significant variations were observed in the occurrence and location of neurovascular structures within the CPM. As shown in Fig. 5, the sympathetic trunk was usually located in front of the CPM. The great vessels, mainly the iliac vessels, migrated gradually from the front of the CPM at the L4/5 disc level to the anterior at mid-L5 level, in the course of their descent. However, in one of the six specimens, the vessels were situated at the front of the CPM, at the L4/5 disc level. Lumbar plexus nerves were situated in the posterior part of the CPM with a general trend of migration observed from dorsal to ventral, which was mainly composed of two branches: the obturator and femoral nerves. The obturator nerve passed obliquely through the CPM, from the posterior border of the L4 vertebrae to the anterior border of the L5/S1 disc. The femoral nerve was always located dorso-caudal inferior to the obturator nerve, and migrated gradually forwards and away from the obturator nerve at the rear of the CPM. The ascending lumbar vein (ALV) was observed in five cases (83.3%), and in four of them it passed from the L4/5 intervertebral foramen, through the CPM, forwards and downwards at the level of the proximal half of L5, and converged with the common iliac vein. In one case, however, it was seen to descend almost vertically and converged with the iliolumbar vessels, which were observed in all specimens and traversed the CPM almost horizontally at the level between the lower edge of the L5 vertebrae and the proximal part of S1.

Anatomical layout in the CPM. (1) Psoas major muscle, (2) ascending lumbar vein, (3) sympathetic chain, (4) femoral nerve, (5) obturator nerve, (6) iliolumbar vessels, (7) external iliac vein, (8) external iliac artery, and (9) segmental vessels.
Grid SystemThis study showed that the 20 grids created on the psoas major surface, to a large extent, coincided with the area of the CPM. The neurovascular structures identified within each grid were recorded, and the results are shown in Table 2. Compared with observations of vertebrae and discs from previous studies, several characteristics and tendencies were observed: (i) although there was significant anatomical variation, there was a considerably lower frequency of occurrence of neurovascular structures in the grids at the L4/5 level than at the L5/S1 level; (ii) the anterior grids at the L4/5 disc level corresponded with the “safe zone” identified in previous studies, which used bony markers for reference. The locations of neurovascular structures observed in this study were similar to those reported in division systems, except that the great vessels were occasionally situated in the front of the CPM; (iii) different from the zone identified in previous studies, at the level of the distal half of L5 and below, the great vessels were generally distributed in grids I and II, and the ALV and obturator nerve in grid II, where the anterior edge of the psoas major exceeded that of the L5 and S1 vertebrae; and (iv) it is noteworthy that the ALV and obturator nerve could occasionally be identified in the zone of grids I and II, at the L4/5 level and proximal to L5, although the neurovascular structures within were sparse. The risk of different grid was shown in Fig. 6 and different color blocks represented corresponding risks.
TABLE 2. The occurrence and distribution of neurovascular structures within the cleft of psoas major (CPM) Grid of CPM I II III IV L45 discGV (1)
ALV (1)
ON (2)
ALV (5)
FN (6)
ON (6)
ALV (2)
Upper of L5 vertebraGV (3)
ALV (2)
SC (2)
ON (2)
ALV (3)
FN (1)
ON (6)
ALV (4)
FN (6)
ON (4)
Lower of L5 vertebraGV (6)
ON (4)
ALV (2)
SC (6)
GV (4)
ON (6)
ALV (3)
FN (5)
ALV (2)
ON (4)
FN (6)
L5S1 discGV (6)
ILV (1)
ON (2)
SC (6)
GV (6)
ALV (1)
ILV (4)
ON (2)
FN (6)
ILV (4)
FN (6)
L5N (6)
ILV (3)
Upper of S1 vertebraGV (6)
ILV (5)
SC (6)
GV (6)
ILV (5)
SC (6)
FN (6)
ILV (3)
SC (6)
FN (6)
ILV (6)
L5N (6)
ALV, ascending lumbar vein; FN, femoral nerve; GV, great vessel; ILV, iliolumbar vein; L5N, lumbar 5 nerve root; ON, obturator nerve; SC, sympathetic chain.
The risk distribution in the CPM. Using grid system of the CPM, the risk degree of operation in the grid is marked by recording the total number of different structures appearing in each grid area, and expressed by different color blocks. Green represents safety, yellow warning, red danger, and purple and dark blue prohibition.
Discussion Formation and Clinical Significance of CPMThe lateral aspects of the lumbar vertebrae are covered by the psoas muscle, which is a homogeneous muscle with a continuous attachment to the vertebral column at one end from T12 to L4, tapering to a single, round tendon at the other end. The fascicle of psoas is rarely attached to the L5 vertebral body6. A previous study showed the lumbar plexus nerves located posteriorly, beneath the psoas muscle and arranged from dorsal at L2, to ventral at L512. The ALV and iliolumbar vein (ILV) also run beneath the psoas muscle with their own regular pattern13. Sivakumar et al. found that if the length of the ALV or the distance between the ILV and common iliac vein was less than 3 cm, venous avulsion would likely occur. Mayer also warned of ligating veins during surgery1. Damage of these structures would cause major complications. Our results show that the psoas muscle does not attach to the lateral aspects of L5, and that the anterior border of the psoas muscle was adrift in all six specimens. This indicated that a cleft existed between the psoas muscle and the lateral aspect of the lumbar vertebrae, from the level of the caudal quarter end of L4 to that of the cranial end of S1. We have called this cleft the CPM (Fig. 3). Our results showed that the ALV, ILV and obturator and femoral nerves are all contained within the CPM, but that the sympathetic trunk is not. Taking into consideration the complex structures within the CPM, stepwise exposure of the cleft by gentle psoas splitting, followed by dissection of the nerves and vessels within the CPM, and finally accessing the target disc and vertebral surface, would help to reduce the risk of damage to the neurovascular structures covered by the psoas major muscle during surgery.
The Main Risk Factors of LLIF in CPM Great VesselsThe overlap of great vessels and psoas major muscle poses a significant risk for LLIF. Davis et al. measured the distance between the lateral border of the great vessels and the anterior medial border of the psoas to identify the safe access corridor for LLIF14. The results showed that the distances, both in the static state and with mild psoas retraction, gradually narrowed from the L2/3 to the L4/5 level. In this study, we focused on the distribution of vessels within the CPM, with the anterior border of psoas major in the lateral decubitus position. It is worth noting that in all investigated specimens, the great vessels were located anteriorly in the CPM, at the level of mid-L5 and below. It was situated anterior to the CPM at L4/5 disc space in five specimens, but was partially overlapped by psoas major in one. These differences could be explained by the different cadaveric positions used. It is important to note that there may also be differences concerning reference and measurement methods between cadaveric specimens and patients. Taken together, we can assume that there are remarkable variations in the distance between the great vessel and the anterior border of the psoas muscle in the CPM, and a narrow space or structural overlap is often found, especially at the L4/5 level in the lateral decubitus position. Based on these facts, retaining a small piece of the psoas muscle in the ventral part would be a better alternative to avoid injury of the great vessel.
ALVThe ALV represents a communication vessel between the common iliac, iliolumbar and lumbar veins. The ILV drains the iliac fossa, and the iliacus and psoas muscles. Recent studies have proposed that the ALV and ILV, even when interconnected, should be considered as separate veins, as the first is a longitudinal structure ascending to connect to the azygos system, and the second is more horizontal in orientation15. Davis et al. demonstrated that it is critical to consider the ILV during spinal surgeries near the lumbosacral region16, however, Lolis et al. found that the ILV is absent in the majority of cases (51/100, 51%)17. In contrast, we identified the ILV in all six specimens investigated in this study, and in five of the six (83.3%) the ALV was observed in the CPM. The ALV straddles the psoas muscle obliquely, over the upper part of the L5 vertebrae, upwards from ventral to dorsal. Compared with the ILV, the ALV is located closer to the L4/5 discs. These results indicate the risk of ALV injury during dissection. As the ALV is a valve-less vein, damage during surgery could result in significant bleeding from the iliac venous system.
Obturator NerveAccording to the literature, there is a 6.0%–33.6% incidence of sensory or motor deficits after lateral fusion procedures18. These iatrogenic nerve injuries may be secondary to direct mechanical compression, laceration, stretch/traction, or indirect ischemia caused by the insertion and deployment of the tubular dilators and surgical retractors. Benglis et al. found that much of the lumbar plexus lies on the dorsal surface of the psoas muscle, within a compartment created by the transverse process–vertebral body junction, with a general trend of dorsal to ventral migration from L2 to L512. This is consistent with our findings that the femoral nerve, the main trunk of the lumbar plexus, was mainly located in front of the fascicles arising from the transverse process, above the L4/5 level. Interestingly, in this study, the lumbar plexus was mainly located in the posterior part of the CPM, at L4/5 and below, but no nerve branches were observed in the L4/5 disc space. Further results have shown that the obturator nerve, as one branch of the lumbar plexus, travels obliquely from posterior superior to antero-inferior in CPM, which is frequently interdigitated with the ALV, especially at the L5 vertebral levels. The nerve is positioned closer to the L4/5 disc than the femoral nerve, therefore, direct injury of the obturator nerve may be more prominent during establishment and maintenance of the surgical corridor than the femoral nerve.
GFNAlthough GFN is not distributed in CPM, it is still an important risk factor for LLIF. Injury of the GFN is the main complication when the dilator or retractor nerves pass through psoas major. Geh found, after piercing the psoas at around level L3/4, that the GFN exited from the middle third of the psoas muscle's anterior surface in 70% of cases, the dorsal third in 20%, the ventral third in 10%19. We observed similar results. Therefore, it is thought that the GFN may be damaged if the psoas major muscle is split. Based on anatomical studies, several authors believe that this nerve should be easily distinguished during exposure of the psoas muscle under direct visualization7. The possibility of damaging the GFN was not considered. Moro et al. proposed that GFN palsy rarely becomes a serious problem as long as the patient is informed of the possibility of sensory disturbance and comprehension before surgery8.
Significance of Novel Grid System in Improving the Safety of LLIFPrevious studies have indicated the position of neurovascular structures in relation to the intervertebral discs and vertebral bodies7-11. Based on these results, the vertebral bodies and discs are usually used as landmarks to identify the “safe zone”8-10, which unfortunately still has several disadvantages in clinical practice as the landmark bony structures and discs are frequently concealed by the psoas major. Therefore, it is not possible to directly locate the great vessels, lumbar plexus and their branches with this safe zone delineation, and the intervertebral disc guiding can only be carried out by fluoroscopy rather than by full visualization. Another problem limiting the use of vertebral or disc landmarks is that there is no absolute safe zone because of anatomical variants20. Finally, the anatomical relationship of the psoas muscle with the neurovascular arrangement differs from that of vertebrae or discs, which could mislead positioning of the retractor system during surgery. To overcome these limitations, we developed a novel grid system of the psoas muscle to identify the locations of the lumbar plexus and blood vessels in the CPM, and counted the sum of anatomic structures in each grid to alert the corresponding risk. Different from the previous researches on “safe zone”, we found no safe area in CPM except the zone of grids I/II, especially operating at the level of L5S1 disc would face great risks. In the grid study, the significant variation in distribution of neurovascular structures was observed in the CPM, confirming that there is no absolute safe zone for LLIF.
Insights of the Novel Grid System for LLIFThe novel grid system virtually projects the anatomical structures hidden under the psoas major muscle onto its surface. The denseness of anatomical structures in each grid can indicate the risk of surgery there. Therefore, we get the following insights. (i) Our results show that the denseness of the anatomical structures of grids I and II of L4/5 segment is the lowest, so they are considered to be the safe surgical areas, but compared with the possible existence of great vessels in grid I, operation in grid II is safer. (ii) Anatomically, the anterior part of the lower edge of L4 vertebral body is the attachment area of the psoas major muscle, in which there is no important anatomical structures distribution. Therefore, it is more appropriate to separate the psoas major muscle from cranial to caudal during operation. (iii) For another LLIF operation window in CPM, L5/S1 segment, from Table 2, we know that anatomical structures are densely distributed in all grids of this segment. In particular, great vessels are distributed in grids I and II, while femoral nerve is distributed in grids III and IV. The risk of surgery is huge there. Therefore, we recommend not to perform LLIF in the L5/S1 segment. (iv) Compared with the longitudinal great vessels and femoral nerve, the transversal ALV and ILV are more intractable troubles. (v) The grids III and IV of CPM have dense anatomical structures distribution in all segments. Therefore, we suggest that operation in the posterior part of the psoas muscle of CPM should be avoided in any circumstance. In fact, the LLIF of L5S1 segment was not performed through the gap between the psoas major muscle and great vessels, but from the front of the internal iliac vessels21, 22.
Limitations and ProspectsThe main limitation of this study is the small sample size, and it is possible that there are some variations in the arrangement of neurovascular structures within the CPM. Some nerve and vessel branches may exist with greater frequency than was shown in this study. Cadaveric study can not truly reflect the characteristics and variation of anatomical structures in physiological state. In addition, the surgical position may cause the shift of important anatomical structures and the change of anatomical adjacent relationship, especially psoas major muscle, great vessels and femoral nerve23.
In our follow-up study, the method of image overlap was adopted to avoid the limitation of sample size, observe the anatomical distribution and variation in CPM under physiological state, and evaluate the impact of body position change on LLIF surgical risk by simulating the actual operation position. This study is the basis of related follow-up research.
Nevertheless, our findings provide spinal surgeons with an awareness of the existence of the CPM over the surface of the L4/5, L5 vertebrae and L5/S1, which is important when performing spinal fusion surgery using the transpsoas or prepsoas approaches.
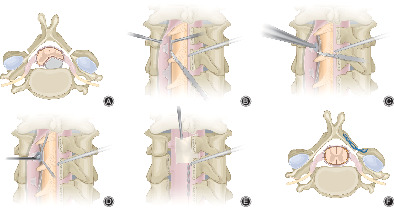
To our knowledge, this is the first study to identify the CPM, its contents and boundary. The neurovascular structures most vulnerable to damage during LLIF are mostly situated within the CPM, which otherwise could provide a potential cavity for direct visualization during LLIF. Consequently, we recommend the following modifications to avoid damage to the neurovascular structures in the CPM during the LLIF procedure: (i) Identification of the CPM is recommended, to determine the optimal dilator or retractor insertion method. We propose a three step process, first identification of the CPM, followed by dissection of the neurovascular structures, and finally docking of the retractor on the vertebrae or discs, rather than a dilator or retractor being blindly placed on the lateral vertebral or disc surface through the psoas major24. The surgeon is thereby able to visually identify and protect both the nerves and vessels located within the CPM. (ii) Instead of circumferential dilation of the psoas, a longitudinal split technique is recommended using a separated plate as the psoas retractor with sequential and gentle muscle splitting to ensure visibility throughout.
AcknowledgmentsNational Natural Science Foundation of China (Grant No.81572177) was received in support of this work. Major Scientific and Technological Plan for Medicine and Health of Zhejiang Province (WKJ⁃ZJ⁃1903).
Ethical StatementThe procedures in the study were undertaken in accordance with the ethical standards of the Helsinki Declaration and had been approved by the local ethical committee. The manuscript submitted does not contain information about medical device(s)/drug(s). No relevant financial activities outside the submitted work.
Comments (0)