
Remember me
Acute myocardial infarction (MI) is a highly prevalent non-communicable disease with a significant burden worldwide.1 Previous studies have shown that inflammation and immune cells share a significant portion of the onset, development, and prognosis of the patients with ST-elevated myocardial infarction (STEMI).2 Changes of white blood cells have been used as an independent risk factor for predicting cardiovascular events. It has been demonstrated that preoperative neutrophil-to-lymphocyte ratio (NLR) has a good predictive value of mortality and recanalization of impaired coronary blood flow in patients with STEMI after percutaneous coronary intervention (PCI).3,4 The relation of the monocyte, neutrophil, and lymphocyte with the mortality of MI has been demonstrated lately.5,6 Neutrophils, the most abundant leukocytes in the circulation, are actively involved in atherogenesis and plaque destabilization.7,8
Several mechanisms could probably explain the role of neutrophils in atherosclerosis either through infiltrating coronary atherosclerotic plaques and the infarcted myocardium and mediating tissue damage or through aggravating endothelial dysfunction or promoting endothelial erosion with resultant weak fibrous caps and neo-intima formation which might contribute to plaque destabilization.9,7
Lymphocytes are also an integral part of the immune system, which participate in every phase of atherosclerosis. Lymphocytopenia, resulting from increased lymphocyte apoptosis, contributes to atherosclerotic plaque growth, lipid core development, plaque destabilization, post-infarct cardiac remodeling, and progression.10,11
Some studies have suggested that, at least in a subset of patients, eosinophils and basophils also may play a pathogenetic role.12,13 These cells, indeed, are rich in small granules, which contain many chemical mediators, released by a process called degranulation following activation of the cell. This process can favor thrombus formation and enhance vasoconstriction at coronary level.14,15
2 Aim of the workTo evaluate the association between basophilic counts and in-hospital major adverse cardiac events in patients with STEMI.
3 Materials and methodsA retrospective observational study was conducted on 607 patients, admitted to the critical care department at Cairo university hospitals with ST-elevation myocardial infarction and were candidates for primary PCI from 2013 to 2017. These patients were managed according to published ESC guidelines at the time being.16 The study was approved by our institutional ethical committee.
Our study recruited patients who were diagnosed with acute STEMI. Acute myocardial infarction was diagnosed upon detection of a rise and/or fall of cardiac biomarkers (preferably troponin) with at least one value above 99th percentile of the upper reference limit., together with evidence of myocardial ischemia with at least one of the following: symptoms of ischemia, ECG changes, development of pathological Q waves in ECG, or imaging evidence of new loss of viable myocardium or new regional wall motion abnormality.17
ECG criteria were based on changes of electrical currents of the heart (measured in millivolts). Typically, ST-segment elevation in acute myocardial infarction, measured at the J point, in two contiguous leads in the absence of left ventricular (LV) hypertrophy or left bundle branch block.14 In patients with inferior myocardial infarction, we recorded right precordial leads (V3R and V4R) seeking ST elevation, to identify concomitant right ventricular infarction. Likewise, ST-segment depression in leads V1–V3 suggested myocardial ischemia, especially when the terminal T-wave was positive (ST-elevation equivalent) and was confirmed by concomitant ST elevation ≥0.1 mV recorded in leads V7–V9.16
Exclusion criteria included patients with evidence of an acute or chronic infection, hematological diseases, history of trauma or surgical operation within preceding 2 weeks, or patients diagnosed with immune system deficiencies, malignancies, autoimmune disorders or on immunosuppressive regimens including steroids.
All patients admitted to critical care department with acute ST elevation myocardial infarction were referred for primary percutaneous coronary intervention, if indicated, within a timely protocol. Those patients were subjected to thorough clinical history and physical examination to document cardiac status, clinical compensation and to exclude possible complications. Written informed consent from the patient was obtained to allow for data collection.
Routine laboratory tests including complete blood picture on admission and 24 hours (hrs) later to record absolute and relative basophil counts. Lactate and high sensitivity C-reactive protein (hsCRP) were measured on admission. The SYNTAX score was employed for the risk stratification of patients undergoing revascularization.18
Patients were followed up for Major adverse cardiac and cerebrovascular events (MACCEs) during the hospital stay. MACCEs included death, stroke, target vessel revascularization, and myocardial re-infarction.
Procedure complications included the No-reflow phenomenon (defined as resultant TIMI flow less than III), side branch occlusion (diameter ≥1.5 mm), and vascular access bleeding that necessitated blood products transfusion and/or vascular intervention. Another recorded complication is contrast-induced nephropathy (CIN) defined as either a 25% increase in serum creatinine from baseline or a 0.5 mg/dL (44 μmol/L) increase in absolute serum creatinine value within 48–72 hours after intravenous contrast administration.
Complicated in-hospital course was defined as those patients who experienced medical complications that necessitated supportive specific ICU measures, including patients who needed respiratory support (invasive and non-invasive), hemodynamic support, or renal replacement therapy.
Blood sampling and the blood parameters; absolute and relative basophil counts was done, using SYSMEX and CELLTEC devices System. The SYSMEX and CELLTEC devices used flow cytometric techniques to analyze red blood cells, platelets, and white blood cells.19,20
3.1 Statistical analysisData were summarized by descriptive statistics using mean and standard deviation or frequency and percentage as appropriate. Mean values and standard deviation were compared using a simple t test (for two variables) or ANOVA test (for more than two variables). Mann-Whitney test was used for non-parametric data. Percentages were compared using the chi-square (x2) test. Pearson correlation was used for the analysis of correlation. Logistic regression was carried out to identify potential predictors for in-hospital MACCE and in-hospital mortality. Receiver operating curve (ROC) was plotted for optimal cutoffs for MACCE prediction. Kaplan Meier curve was plotted for survival analysis with Log-rank test reported. The software used in the analysis was the statistical package SPSS version 23. P-value ≤.05 was considered statistically significant.21
4 ResultsThis was a retrospective observational cohort study involving 607 patients who presented with STEMI. The mean age of our study population was 57.7 ± 11.3 years old. Male patients represented 80.0% of total patients (488 male patients). The length of hospital stay was 6.5 ± 5.0 days. Demographics, laboratory, and angiographic data were presented in Table 1. A total number of 688 stents were deployed. Patients who developed MACCEs were 79 (13%). Death (11%), target vessel revascularization (TVR) was 0.8%, myocardial infarction was 0.8%, and stroke was 1%. Organ support measures were recorded as well: hemodynamic support (15.7%), respiratory support (7.4%), and renal replacement therapy (0.3%).
Table 1 - Demographics, laboratory and angiographic data All (N. 607) No MACCE (N. 527) MACCE (N. 79) P Age 57.7 ± 11.3 57.2 ± 11.0 61.4 ± 12.4 .002 LOS∗ 6.5 ± 5.3 6.5 ± 4.8 6.8 ± 7.7 .765 Pain duration 5.1 ± 2.6 5.0 ± 2.5 5.5 ± 3.1 .178 hsCRP† 57.1 ± 81.9 49.4 ± 71.7 108.7 ± 119.5 <.001 Lactate 2.5 ± 1.6 2.3 ± 1.5 3.4 ± 2.1 <.001 Smoking 395 (65.1%) 349 (66.1%) 46 (58.2%) .108 Hypertension 296 (48.8%) 249 (47.2%) 47 (59.5%) .027 Diabetes 222 (36.6%) 184 (34.8%) 38 (48.1%) .016 Dyslipidemia 213 (35.1%) 185 (35.0%) 28 (35.4%) .519 TLC1‡ 11.6 ± 4.9 11.1 ± 4.3 15.1 ± 6.8 <.001 TLC2§ 10.8 ± 4.6 10.2 ± 4.0 15.1 ± 5.9 <.001 ABC1|| 542.3 ± 732.1 466.0 ± 587.3 1052.3 ± 1237.4 <.001 ABC2¶ 441.4 ± 540.7 371.9 ± 419.9 906.1 ± 910.3 <.001 RBC1# 3.8 ± 2.8 3.5 ± 2.5 5.5 ± 3.9 <.001 RBC2∗∗ 3.5 ± 2.4 3.2 ± 2.1 5.3 ± 3.6 <.001 SYNTAX score 17.5 ± 7.5 16.7 ± 7.1 20.5 ± 8.3 <.001 Lesion length 24.4 ± 6.2 24.6 ± 6.3 23.9 ± 5.7 .276 Lesion diameter 3.2 ± 0.4 3.1 ± 0.4 3.2 ± 0.4 .179 Stent no.†† 1.2 ± 0.5 1.3 ± 0.5 1.2 ± 0.4 .376 ST resolution‡‡ 296 (48.8%) 269 (50.9%) 27 (34.2%) .004 Procedure comp§§ 38 (6.3%) 19 (3.6%) 19 (24.1%) <.001 No-reflow 70 (11.5%) 43 (8.1%) 27 (34.2%) <.001 CIN|||| 64 (10.5%) 35 (6.6%) 29 (36.7%) <.001MACCE, major adverse cardiac cerebrovascular events.
∗LOS, length of stay.
†hsCRP, high sensitivity C reactive protein.
‡TLC1, total leukocytic count on admission.
§TLC2, total leukocytic count within 1st 24 h.
||ABC1, absolute basophil count on admission.
¶ABC2, absolute basophil count within 1st 24 h.
#RBC1, relative basophil count on admission.
∗∗RBC2, relative basophil count within 1st 24 h.
††Stent no., stent number.
‡‡ST resolution, ST segment resolution ≥70%.
§§Procedure comp, periprocedural complications.
||||CIN, contrast induced nephropathy.
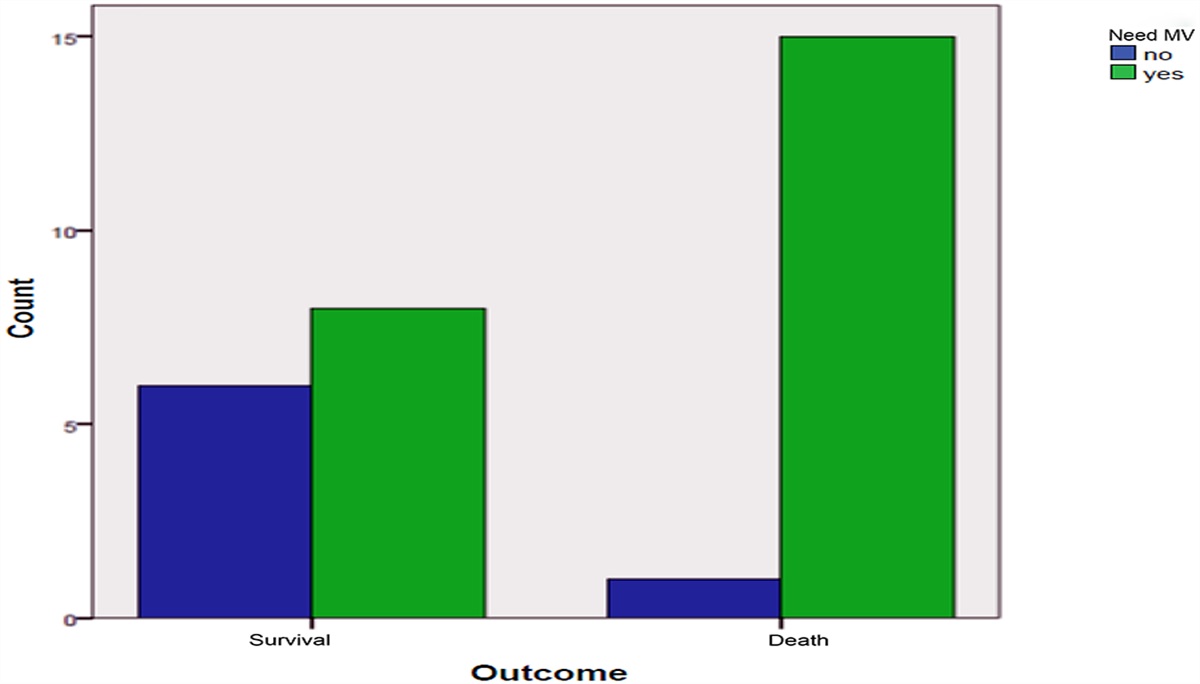
For patients who needed organ support measures, they showed higher absolute basophilic counts on admission (786.6 ± 979.6 versus 494.6 ± 664.2, P .005) and 24 hours later (686.4 ± 732.3 versus 393.7 ± 481.4, P < .001). Similarly, patients who died showed higher counts on admission (1112.5 ± 1290.8 versus 470.3 ± 591.5, P < .0001) and 24 hours later (943.1 ± 940.5 versus 378.1 ± 428.1, P < .0001). Also, absolute basophilic counts on admission were higher in the CIN group on admission (987.9 ± 1216.1 versus 489.7 ± 633.3, P .002) and 24 hours later (765.2 ± 815.4 versus 403.2 ± 485.5, P .001).
Multivariate regression showed ST-segment resolution <70%, total leucocytic count within 1st 24 hours, basophilic counts on admission and within 1st 24 hours, contrast-induced nephropathy, and need for organ support measures were potential significant predictors for in-hospital MACCE (Nagelkerke R2 0.745 and fitness of goodness 0.776). Another multivariate regression showed hypertension, ST-segment resolution <70%, baseline creatinine, total leucocytic count within 1st 24 hours, basophilic counts on admission and within 1st 24 hours, SYNTAX, myocardial blush grading, and need for organ support measures were potential significant predictors for in-hospital mortality (Nagelkerke R2 0.759 and fitness of goodness 0.395). These regression models were represented in Tables 2 and 3.
Table 2 - Multivariate regression analysis to predict MACCE 95% Confidence interval for Hazards risk B P Hazards risk Lower Upper Age .029 .135 1.029 .991 1.069 Gender (male) −.303 .568 .738 .261 2.088 ST resolution 2.167 .001 8.728 2.551 29.869 SYNTAX .069 .680 1.071 .772 1.488 Post SYNTAX −.012 .947 .989 .702 1.393 Procedure comp .222 .796 1.248 .233 6.681 Organ support 1.626 .001 5.082 2.002 12.900 TLC1 .001 .994 1.001 .867 1.154 TLC2 .213 <.001 1.237 1.104 1.386 MBG −2.865 <.001 .057 .026 .123 ABC1 −.623 .010 .536 .335 .859 ABC2 .670 .007 1.955 1.202 3.179 CIN 1.456 .010 4.289 1.418 12.968 No-reflow −.666 .313 .514 .141 1.873 Constant −4.541 .006 .011ABC, absolute basophil count; CIN, contrast induced nephropathy; MACCE, major adverse cardiac cerebrovascular events; MBG, myocardial blush grading; TLC, total leukocytic count.
ABC, absolute basophil count; MBG, myocardial blush grading; TLC, total leukocytic count.
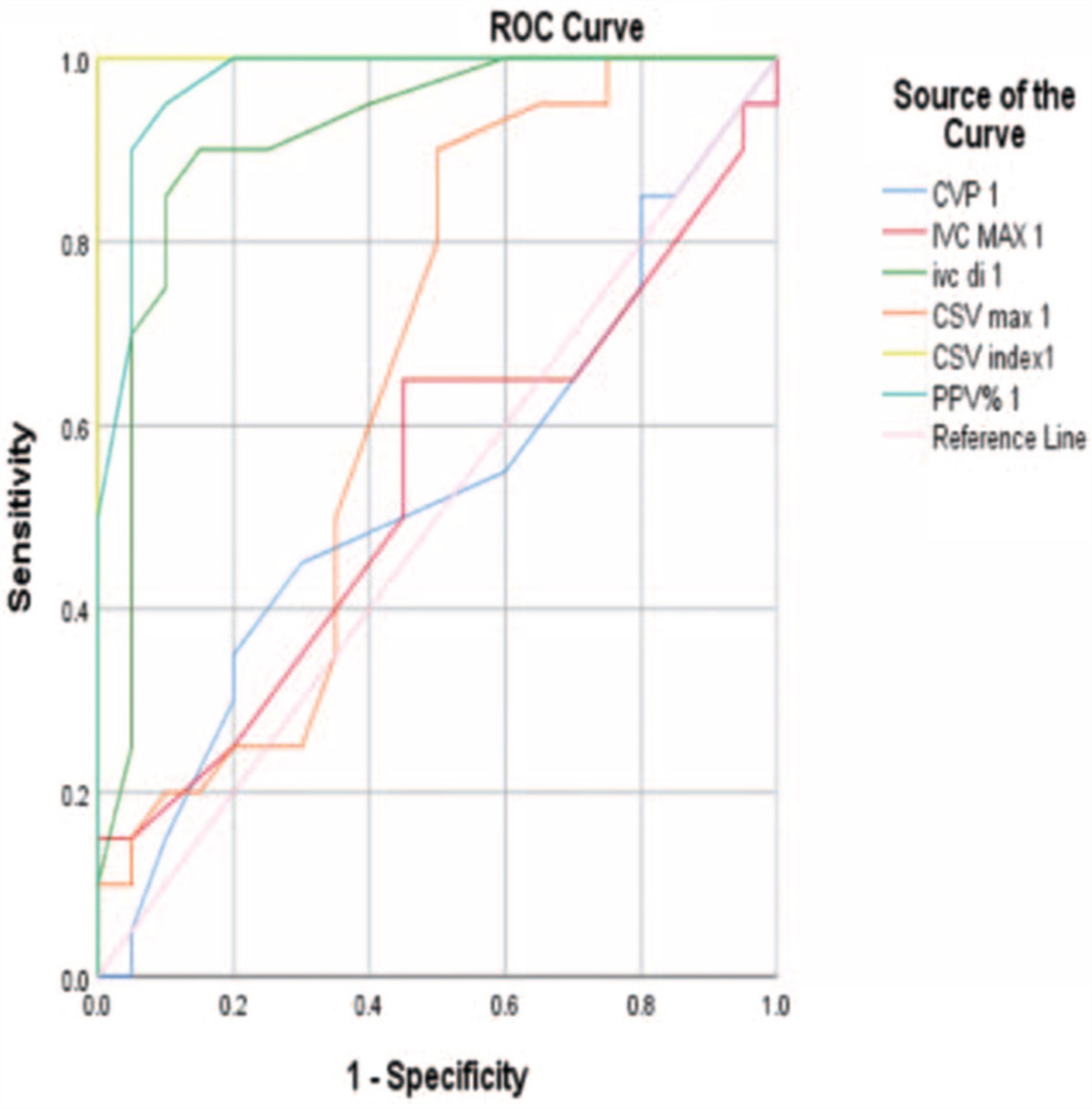
ROC was plotted for basophilic and total leucocytic counts on admission and 24 hours later to predict MACCE in STEMI patients in Table 4 and Figure 1. ROC was plotted for basophilic and total leucocytic counts on admission and 24 hours later to predict in-hospital mortality in STEMI patients in Table 5 and Figure 2. Kaplan Meier curve was plotted for patients whose absolute basophilic count on admission ≤370/mm3 versus those >370/mm3 in Figure 3 and plotted for patients whose absolute basophilic count within 1st 24 hours ≤350/mm3 versus those >350/mm3 in Figure 4. Survival analysis was statistically significant between both groups.
Table 4 - ROC to predict MACCE in STEMI patients Area under curve P Cut-off Sensitivity (%) Specificity (%) ABC1 0.710 <.001 370.0/mm3 68.4 63.6 ABC2 0.763 <.001 350.0/mm3 73.4 68.7 RBC1 0.694 <.001 3.3% 68.4 63.9 RBC2 0.698 <.001 3.2% 67.1 63.6 TLC1 0.696 <.001 11 × 103/mm3 70.9 59.2 TLC2 0.769 <.001 11 × 103/mm3 70.9 65.7ABC, absolute basophil count; MACCE, major adverse cardiac cerebrovascular events; RBC, relative basophil count; ROC, receiver operating curve; STEMI, ST elevation myocardial infarction; TLC, total leukocytic count.
 Figure 1:
Figure 1: ROC was plotted for basophilic and total leucocytic counts to predict MACCE in STEMI patients. Blue line represents basophilic count on admission. Purple line represents basophilic count in 1st 24 h. Green line represents total leucocytic count on admission. Red line represents total leucocytic count in 1st 24 h. ROC, receiver operating curve.
Table 5 - ROC to predict in-hospital mortality in STEMI patients Area under curve P Cut-off Sensitivity (%) Specificity (%) ABC1 0.726 <.001 380.0/mm3 70.6 64.7 ABC2 0.772 <.001 375.0/mm3 70.6 71.2 RBC1 0.712 <.001 3.3% 72.1 63.9 RBC2 0.717 <.001 3.2% 72.1 63.6 TLC1 0.706 <.001 11 × 103/mm3 70.6 58.6 TLC2 0.761 <.001 11 × 103/mm3 70.6 64.9ABC, absolute basophil count; RBC, relative basophil count; ROC, receiver operating curve; STEMI, ST elevation myocardial infarction; TLC, total leukocytic count.
 Figure 2:
Figure 2: ROC was plotted for basophilic and total leucocytic counts to predict in-hospital mortality in STEMI patients. Blue line represents basophilic count on admission. Purple line represents basophilic count in 1st 24 h. Green line represents total leucocytic count on admission. Red line represents total leucocytic count in 1st 24 h. ROC, receiver operating curve.
 Figure 3:
Figure 3: Kaplan Meier curve to reveal survival of those with absolute basophilic count on admission <370/mm3 vs those ≥370/mm3. Solid line represents those with basophilic count <370/mm3 while dotted line represent those with count ≥370/mm3. Log rank test reported.
 Figure 4:
Figure 4: Kaplan Meier curve to reveal survival of those with absolute basophilic count within 1st 24 h <350/mm3 vs those ≥350/mm3. Solid line represents those with basophilic count <350/mm3 while dotted line represent those with count ≥350/mm3. Log rank test reported.
5 DiscussionOur findings explored associations between basophilic counts on admission and 24 hours later with major adverse events in STEMI patients. Patients who developed MACCE showed higher relative and absolute basophil counts. Our regression model showed that absolute basophilic counts were significant predictors of in-hospital MACCE, namely in-hospital mortality. Our study could provide potential cutoffs for absolute and relative basophilic counts to predict in-hospital MACCE and mortality.
The role of basophils in thrombosis is still investigational. Basophils are known members of the granulocytes and constitute less than 1% of the circulating leukocytes. Controversial studies could not verify a common bone marrow-derived hematopoietic precursor cell for both basophils and mast cells. However, basophils have granules, containing histamine, proteolytic enzymes, and other inflammatory mediators.22
Previous studies have shown that inflammation and immune cells could underlie the pathogenesis of acute coronary syndromes.23 Moreover, changes of white blood cells have been shown to provide prognostic information for predicting cardiovascular events.24,25 It has been demonstrated that preoperative NLR had a good predictive value of MACCE.24,25 Besides, the lymphocyte-to-monocyte ratio was suggested as a marker of inflammation related to coronary artery disease.26 Other studies have postulated that eosinophils and basophils may play a pathogenetic role, through releasing chemical mediators that might favour thrombus formation and enhance vasoconstriction at the coronary level.12–15 Kounis syndrome is caused by inflammatory mediators such as histamine; arachidonic acid products; platelet-activating factor; and a variety of cytokines and chemokines released during the mast-cell activation. This might have a role in the activation cascade. The same mediators released from similar inflammatory cells are involved in acute coronary events of non-allergic etiology.15
Flow cytometry studies in acute coronary syndrome showed evidence of basophilic activation in acute coronary syndrome settings. A study by Niccoli in 2015 was the first to demonstrate the possible role of allergic inflammation, accompanied by eosinophilic and basophilic activation in acute coronary syndrome. Niccoli demonstrated a greater expression of CD69 and CD203, markers of eosinophil degranulation and of basophil activation, respectively, in patients with acute coronary syndromes, compared to patients with stable angina.27
This was confirmed by Anita study on STEMI and NSTEMI patients.28 He also stated that there was a significant relationship between basophil and high mortality (P < .05). As it is known that in the inflammatory process, basophil histamine as a mediator issues a major and rapid response of vascular inflammation leading to local capillary vasodilation and might trigger neutrophils and monocytes to induce inflammation.
However, a study published by Naser supported the notion that basophils secrete endogenous heparin that might reduce the incidence of deep venous thrombosis.29 These conflicting studies warrant further research to explore the potential role of allergic inflammatory cells in acute coronary syndromes.
Mast cells were believed to share a common origin with basophils. Studies presented conflicting results about its potential role in thrombosis. An interesting hypothesis about the role of mast cells in venous thrombosis was presented by Ponomaryov in mice models. He stated that mast cells could exacerbate DVT likely through endothelial activation and release of Weibel-Palade body (WPB; storage granules present in endothelial cells), which is, at least in part, mediated by histamine.30 On the other side, some authors claimed that mast cells contain both inhibitors of coagulation, such as heparin and tPA, which could be expected to inhibit thrombosis, and proinflammatory mediators, such as histamine and tumor necrosis factor-α, which could exert a prothrombotic effect.31
The role of basophils in acute MI is still under study. Our findings supported the notion that allergic inflammatory cells could play a role in prognostication in this subset. Further studies are warranted to confirm our findings and examine potential therapies that could hamper basophilic activation and explore their therapeutic benefits.
6 ConclusionAbsolute and relative basophilic counts were higher in the MACCE group on admission and 24 hours later. They could provide acceptable cutoffs for predicting MACCE in STEMI patients. Targeting allergic inflammatory cells might
Comments (0)