
Remember me
Sepsis and septic shock are major health care problems around the world.1 Some reports state that 0.5%–0.9% of Indonesians get acute kidney injury (AKI), 0.7% is hospitalized patients and up to 20% of the patients are treated in intensive care unit (ICU). Kidney is one of the most affected organ during sepsis which contribute to mortality and morbidity of sepsis.2 The incidence in developing countries, especially in community-acquired, is difficult to explain because not all AKI patients come to the hospital.3 AKI mortality rates reported from around the world is ranging from 25% to 80%.4 It is estimated that the apparent incidence in communities exceeds much higher from the recorded numbers. The increased incidence of AKI is associated, among others, with an increase in the sensitivity of diagnostic criteria causing milder cases to be diagnose.5
Sepsis may be identified with Quick Sepsis-Related Organ Failure Assessment (qSOFA) criteria on patients with suspected infections that are likely to have poor outcome.1 qSOFA applies three criteria, assigning one point for low blood pressure (SBP ≤ 100 mmHg), high respiratory rate (≥22 breaths per min), or altered mentation (Glasgow coma scale < 15). The presence of two or more qSOFA points is likely to be septic.
Serum creatinine (SCr) that are being used are not sensitive nor specific for detecting AKI, limiting treatment and potentially reducing outcomes.6 New biomarkers are being studied in order to diagnose previous and more specific AKIs.7 Up to this moment, AKI was defined as serum creatinine increase based on Risk, Injury, Failure, Loss, End-stage Kidney Disease (RIFLE) criteria. RIFLE criteria describe three stages of severity of acute renal failure (Risk, Injury, and Failure) and two output variables (Loss and End Stage Kidney Disease). The risk category is defined when the SCr level increases ≥1.5 × baseline; while, injury category is defined when the SCr increases ≥2.0 × baseline; and failure category is defined when the SCr increases ≥3.0 × baseline. The loss stage is defined as complete loss of kidney function >4 weeks, and ESRD is the end stage of renal disease >3 months. Liver-Fatty Acid Binding Protein (L-FABP) is one of the biomarker candidates which is a 14-kDa protein expressed in proximal tubular epithelial cells. Urine levels of uL-FABP may predict adverse outcome and severity of sepsis induced renal impairment. It has also been reported that the levels of uL-FABP in septic shock patients with AKI were higher than those of healthy people, in patients with AKI without sepsis, and in septic patients without septic shock.8–12 Normal urine level for uL-FABP was 16 ng/mL.9
The aims of this study are to determine the correlation between uL-FABP and SCr and to assess whether uL-FABP can predict AKI earlier in septic patients. This survey is expected to obtain the description of uL-FABP in patients suffering from this sepsis, provide input for further research which will be useful for early detection and manage AKI in septic patients. In Healthcare, this study can support the diagnosis and improve AKI management in septic patients. In addition, it is useful for the medical staff to explain to the patient's family about the possibility of septic induced AKI. Finally, it might become a reference for physicians to refer their patients to hospitals with facilities equipped for dialysis especially in remote area hospitals in Indonesia.
2 Subjects and methodsThis prospective study was conducted from January 2017 to May 2017 in ICU of Dr. Wahidin Sudirohusodo Makassar General hospital in South Celebes, Indonesia and its satellite hospitals. The main design of this study applied a diagnostic test and cross sectional and consecutive samplings. Patient which suspected for sepsis in ward or emergency department was included. Any patients diagnosed with renal insufficiency, chronic kidney disease, and genitourinary tract infection previously were excluded. At the time sepsis was suspected, the qSOFA, combining these two or more criteria, that is, changes of consciousness level, systolic blood pressure of 100 mmHg or less, and respiratory rate of 22/minute or greater, was used to determine severity of patient's illness. Mid-stream urine and blood was collected to measure uL-FABP and SCr, respectively. This criterion AKI was defined as an increase in SCr based on RIFLE criteria (Risk stage). uL-FABP levels were measured by enzyme linked immunoassay. This study was approved by ethics committee of Faculty of Medicine, Hasanuddin University. All the patients or their guardians had provided written informed consent to be included in this study. The subjects enrolled in this study were 54 patients admitted to ICU aged from 18 years with sepsis.
The Third International Consensus Definitions for Sepsis recommend qSOFA as a simple prompt to identify infected patients who are likely to be septic outside the ICU. qSOFA criteria can be conducted simply by identifying adult patients with suspected infections that are likely to have poor outcomes.1 qSOFA applies three criteria, assigning one point for low blood pressure (SBP ≤ 100 mmHg), high respiratory rate (≥22 breaths/min), or altered mentation (Glasgow coma scale < 15). The presence of two or more qSOFA points is likely to be septic. Sepsis is defined as an increase in the Sequential Organ Failure Assessment (SOFA) score of two or more points. Septic shock can be identified by a vasopressor requirement to maintain a mean arterial pressure of 65 mmHg or greater and serum lactate level >2 mmol/L in the absence of hypovolemia.1
Statistical analysis applied independent t test, Chi-Square, Fisher's Exact test, ANOVA, receiver operating characteristic (ROC) curve and validity with P < .05 was considered significant.
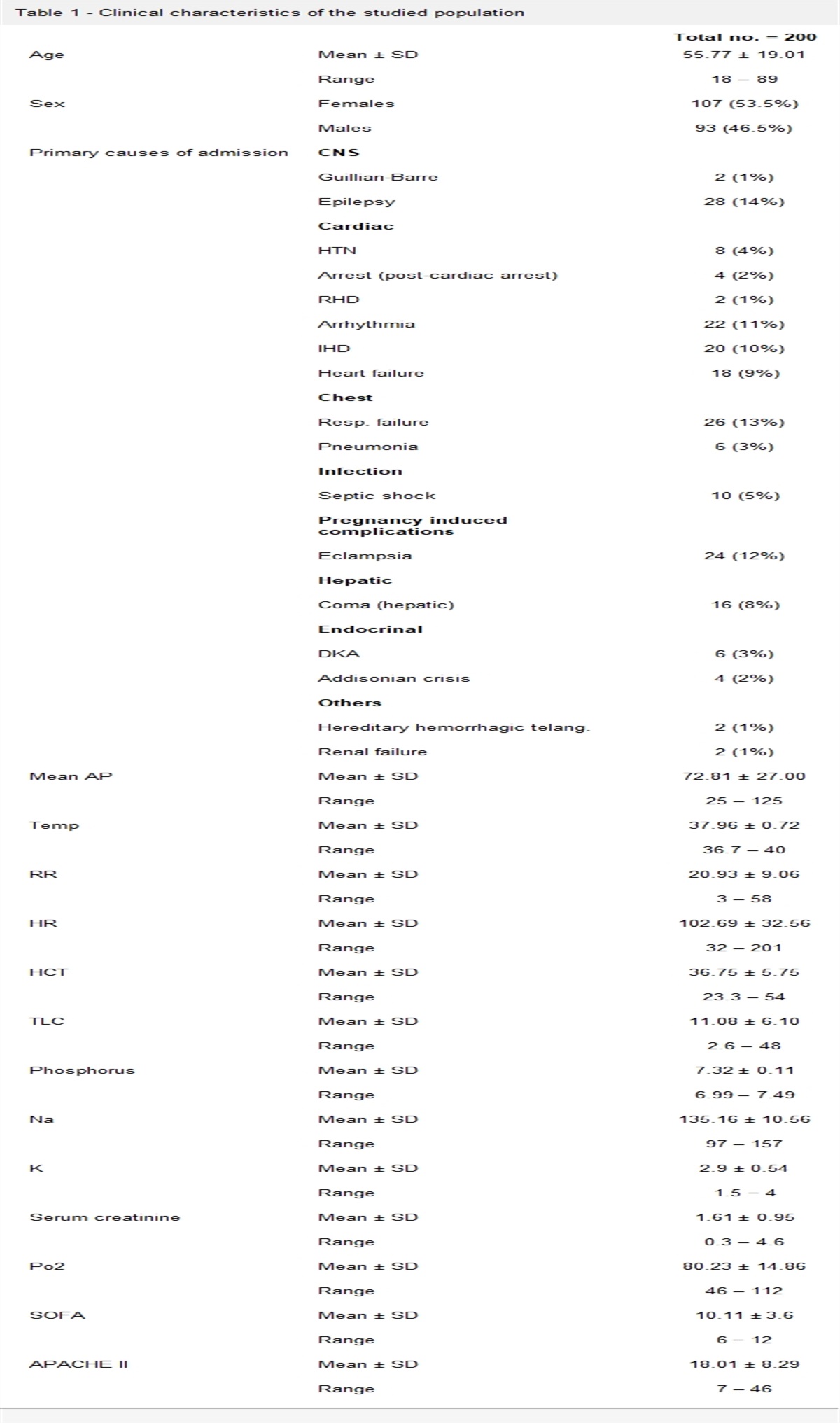
3 ResultsAll patients consisting of 28 patients with sepsis and 26 patients with septic shock were enrolled in this study. The characteristics of subjects are depicted in Table 1. The number of male (57.41%) more than female (42.59%). The largest source of infection was lungs (50%), then abdominal organs (48.14%) and the least was skin and soft tissue infection (1.90%). The number of sepsis patients (51.85%) were higher than septic shock patients (48.15%).
Table 1 - Sample characteristic based on gender and source infection Sepsis (n = 28) Shock sepsis (n = 26) Characteristic Frequency (n) Percentage (%) Frequency (n) Percentage (%) P Gender .610∗ Male 17 31.50 14 25.90 Female 11 20.4 12 22.20 Source infection .889† Pulmonary 13 24.10 14 25.90 Abdomen 14 25.90 12 22.20 Limb 1 1.90 0 0Data showed are in frequency and percentage.
∗Analyzed by Chi-square test.
†Analyzed with Fisher's Exact test.
Table 1 shows that there is no statistically significant differences in gender and the sources of infection between both groups (patients with sepsis and patients with septic shock) with P (.610 and .889), respectively.
Table 2 shows that there is no significant difference for age between both groups (patients with sepsis and patients with septic shock) with P .358.
Table 2 - Sample characteristics based on age Sepsis (n = 28) Shock sepsis (n = 26) Variable Mean SD Min Max Mean SD Min Max P Age (years) 46.93 18.49 18 76 51.27 15.67 18 82 .358Data showed are in mean, SD, min (minimal) and max (maximum), analyzed by independent t test.SD, standard deviation.
Table 3 depicts that there are statistically significant differences between the values of uL-FABP in patients with sepsis and septic shock with P .029.
Table 3 - Levels of uL-FABP (ng/mL) based on sepsis severity Variable n Mean SD P Sepsis 28 61.21 58.14 .029∗ Septic shock 26 109.68 96.90Data showed are in mean and SD.SD, standard deviation; uL-FABP, urine liver-fatty acid binding protein.
∗P < .05, analyzed by independent t test.
Among 54 septic patients participated in the study, it was found that 33 patients were non-AKI patients, 13 patients with AKI (Risk), and 8 patients with AKI (Injury). The difference in mean values of uL-FABP based on AKI criteria can be seen in Table 4.
Table 4 - Levels of uL-FABP (ng/mL) based on RIFLE Variable n Mean SD P Non-AKI 33 39.13 38.86 .000∗ AKI (risk) 13 153.98 74.88 AKI (injury) 8 159.05 97.77Data showed are in mean and SD.AKI, acute kidney injury; SD, standard deviation; uL-FABP, urine liver-fatty acid binding protein.
∗P < .001 analyzed by ANOVA.
Table 5 shows that there is a statistically significant difference between the value of serum creatinine levels in patients with sepsis and septic shock.
Table 5 - Levels of SCr (mg/dL) based on sepsis severity Variable n Mean SD P Sepsis 28 1.36 0.864 .025∗ Septic shock 26 1.92 0.919Data showed are in mean and SD.Scr, serum creatinine; SD, standard deviation; uL-FABP, urine liver-fatty acid binding protein.
∗P < .05, analyzed by independent t test.
Table 6 indicates that there are statistically significant differences between SCr levels in septic patients with non AKI, AKI (Risk) criteria, and AKI (Injury) criteria.
Table 6 - Levels of SCr (mg/dL) based on RIFLE Variable n Mean SD P Non-AKI 33 1.07 0.45 .000∗ AKI (risk) 13 2.09 0.129 AKI (injury) 8 3.21 0.917Data showed are in mean and SD.AKI, acute kidney injury; SCr, serum creatinine; SD, standard deviation; uL-FABP, urine liver-fatty acid binding protein.
∗P < .001, analyzed with ANOVA.
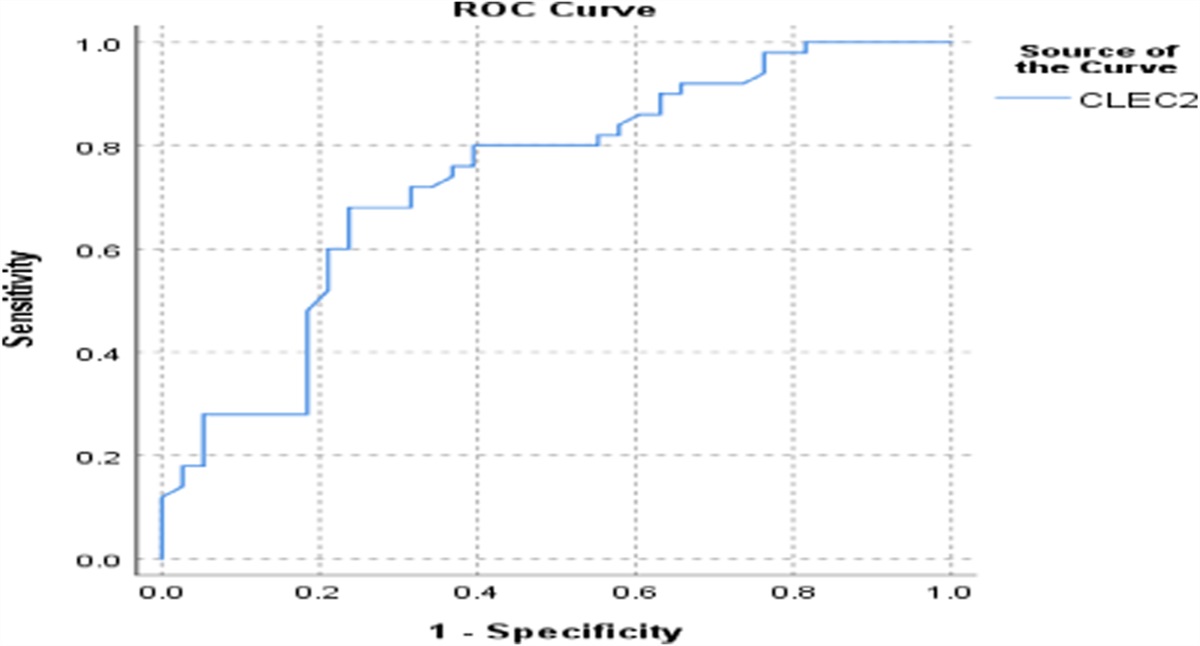
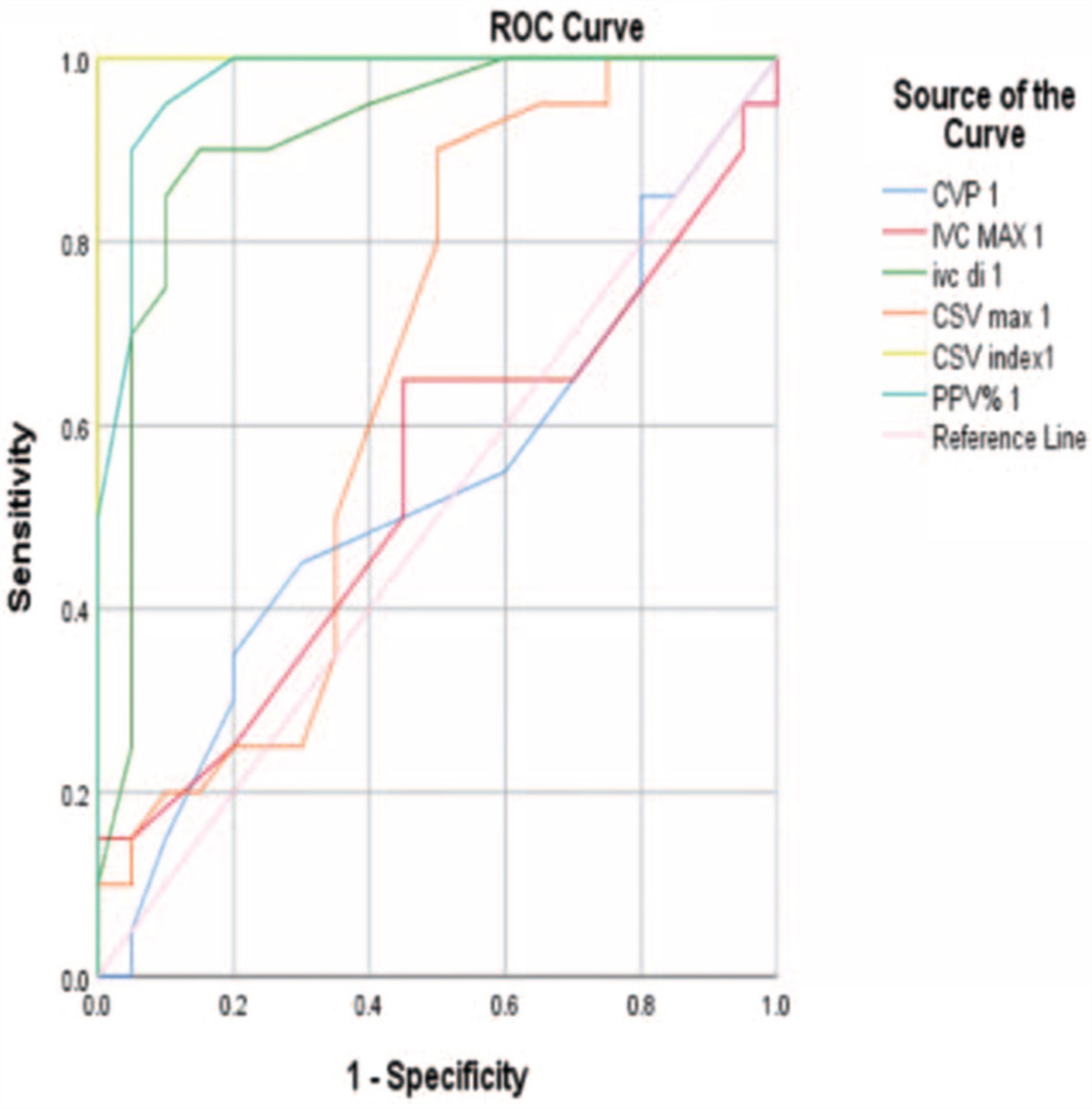
ROC curve analysis in Figure 1 indicates that the area under the curve (AUC) of uL-FABP levels is 0.921 with intervals of 0.847–0.995 (95% significance). Diagnostic examination with AUC value is 0.921 or 92.1. Cut-off value was obtained, which was 29.9 ng/dL. Based on these results, the following sensitivity and specificity were obtained. There was a positive correlation between SCr and uL-FABP (Table 7).
 Figure 1:
Figure 1: ROC curve for uL-FABP. AUC, area under the curve; ROC, receiver operating characteristic; uL-FABP, urine liver-fatty acid binding protein.
Table 7 - Sensitivity and specificity of uL-FABP Variable Cut off point (ng/mL) Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%) uL-FABP 29.9 95.2 54.5 57.1 94.7 70.4NPV, negative predictive value; PPV, positive predictive value; uL-FABP, urine liver-fatty acid binding protein.
Significant differences were shown in the levels of uL-FABP and SCr based on the severity of sepsis (P < .05), with mean values of 61.21 ng/mL for sepsis and 109.68 ng/mL for septic shock. Eunjong cho's in his study was using 28.45 ng/mL uL as normal limits, found that higher uL-FABP was seen as more advance sepsis stage.13
Significant differences was found in creatinine levels based on the severity of sepsis with a value of P < .05. However, their value (measured in sepsis patients (mean 1.36 mg/dL) and sepsis shock patients (mean 1.92 mg/dL) were still within normal limits and the increase of creatinine and slightly increased in septic shock. The mean serum creatinine value in all septic patients was 1.6 ± 0.9 mg/dL. This value was lower compared from Pereira et al. with a result of 2.3 ± 5.5 mg/dL. This might be due to that the subjects of Pereira's research were patients with sepsis who had suffered from AKI, whereas in this study, not all the subjects were AKI sepsis.14,15
There was a significant difference between the severity of AKI and the severity of sepsis according to the RIFLE criteria (P < .05). From the analysis above, it can be concluded that there is a correlation between uL-FABP and RIFLE criteria with P < .05. Although AKI is not established yet by the RIFLE criteria, the uL-FABP may already high (mean 39.13 ng/mL). uL-FABP develop earlier than Scr (RIFLE). The higher uL-FABP levels, the worse AKI will be. According to Eunjung Cho et al.'s, sepsis is one of the factors that increased of uL-FABP. uL-FABP can be used as a predictor of mortality in 90 days of treatment.13
References [1]. Zarjou A, Agarwal A. Sepsis and acute kidney injury. J Am Soc Nephrol 2011;22:999–1006. [2]. Basile D, Anderson M, ànd Sutton T. Pathophysiology of Acute Kidney Injury. Comprehensive Physiology. 5th ed. Vol. 2). Elsevier Inc.; 2012. http://doi.org/10.1002/cphy.c110041. Pathophysiology. Accessed January 5, 2017. [3]. Sinto R, Nainggolan G. Acute kidney injury: Pendekatan Klinis dan Tata Laksana. Maj Kedokt Indones 2010;60(2):81–88. [4]. Davis EN. Acute kidney injury. Phys Assis Clin 2016;1(1):149–159. doi:10.1016/j.cpha.2015.09.006. [5]. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016;315(8):801–810. doi:10.1001/jama.2016.0287. [6]. Susantitaphong P, Siribamrungwong M, Doi K, Noiri E, Terrin N, Jaber BL. Performance of urinary liver-type fatty acid-binding protein in acute kidney injury: a meta-analysis. Am J Kidney Dis 2013;61(3):430–439. doi:10.1053/j.ajkd.2012.10.016. [7]. Seijas M, Baccino C, Nin N, Lorente JA. Definition and biomarkers of acute renal damage: new perspectives. Med Intensiva 2014;38(6):376–385. doi:10.1016/j.medin.2013.09.001. [8]. Sato R, Suzuki Y, Takahashi G, Kojika M, Inoue Y, Endo S. A newly developed kit for the measurement of urinary liver-type fatty acid-binding protein as a biomarker for acute kidney injury in patients with critical care. J Infect Chemother 2015;21(3):165–169. doi:10.1016/j.jiac.2014.10.017. [9]. Pelsers M, Hermens WT, Glatz JF. Fatty acid-binding proteins as plasma markers of tissue injury. Clin Chim Acta 2005;352(1–2):15–35. [10]. Elnady HG, Abdalmoneam N, Abu MM, Hassanain AI, Ibraheim RAM, Abdel H. Urinary liver-type fatty acid-binding protein for early detection of acute kidney injury in neonatal sepsis. Med Res J 2013;21–26. doi:10.1097/01.MJX.0000446938.48277.e6. [11]. Parikh CR, Thiessen-philbrook H, Garg AX, et al. Article performance of kidney injury molecule-1 and liver fatty acid-binding protein and combined biomarkers of AKI after cardiac surgery. Clin J Am Soc Nephrol 2013;8:1079–1088. doi:10.2215/CJN.10971012. [12]. Portilla D, Dent C, Sugaya T, et al. Liver fatty acid-binding protein as a biomarker of acute kidney injury after cardiac surgery (c). Kidney Int 2008;465–472. doi:10.1038/sj.ki.5002721. [13]. Cho E, Yang HN, Jo SK, Cho WY, Kim HK. The role of urinary liver-type fatty acid-binding protein in critically ill patients. J Korean Med Sci 2013;28(1):100–105. doi:10.3346/jkms.2013.28.1.100. [14]. Pereira M, Rodrigues N, Godinho I, et al. Acute kidney injury in patients with severe sepsis or septic shock: a comparison between the ‘ Risk, Injury, Failure, Loss of kidney function, End-stage kidney disease ’ (RIFLE), Acute Kidney Injury Network (AKIN) and Kidney Disease: Improving Global Outcomes (KDIGO) classifications. Clin Kidney 2017;10(3):332–340. doi:10.1093/ckj/sfw107. [15]. Tanaka T, Doi K, Maeda-Mamiya R, et al. Urinary L-type fatty acid-binding protein can reflect renal tubulointerstitial injury. Am J Pathol 2009;174(4):1203–1211. doi:10.2353/ajpath.2009.080511.
Comments (0)