
Remember me


THE EFFICACY OF EVAN® IN POST-OPERATIVE TREATMENT OF BENIGN CORDAL INJURIES: AN OBSERVATIONAL PILOT STUDY.
PATRIZIA ZAMBITO, MD1 e ETTORE BENNICI, MD1
U.O. Otorinolaringoiatria – Ospedale San Giovanni di Dio (Agrigento)
Corresponding author:
Patrizia Zambito,
U.O. Otorinolaringoiatria – Ospedale San Giovanni di Dio, Contrada Consolida, 92100 Agrigento
E-mail: zambito.patrizia@outlook.it
ABSTRACT
Post-surgical treatment of patients with benign pathology of the vocal cords is a useful support to the logopedic rehabilitation. Commonly, it employs anti-inflammatory drugs and corticosteroids by inhalation. This study aims to evaluate the reliability of EVAN® (Ananas comosus titrated in bromelain and Boswellia Serrata titrated at 65% in boswellic acids) as an alternative supplement to the pharmacological treatment in patients undergoing surgical intervention. To this purpose, 56 patients undergoing phonosurgery were divided into two groups and treated postoperatively with EVAN® (2 tablets or sachets/day) for one week or with inhaled corticosteroid for 7 days. Stroboscopic parameters and perceptive analysis of the voice were assessed during early postoperative follow-up and three months after surgery. Patients treated with EVAN® showed a faster recovery of the qualitative parameters of the vocal function and a significant reduction of the postoperative GRBAS score, compared to the control group treated with inhaled corticosteroid. The results of this study suggest that the combination of bromelain and Boswellic acids is safe and effective in the treatment of acute and chronic inflammation of the vocal cords.
INTRODUCTION
Voice production depends on complex mechanisms, such as the coordinated participation of muscle groups that perform an antagonistic action, the bellows action of the lungs and the undulation of the mucosa that covers the vocal cords (body-cover theory) (Zhang, 2016; Hirano, 1974).
The presence of nodules, cysts or polyps on the vocal cords impairs and segments the transmission of the mucosal wave that normally originates from under the glottis and reaches the superior arcuate line (Altman 2007). A diffuse alteration of the muco-undulatory action also occurs in Reinke’s edema due to the change in the space that constitutes the transition area between “body” and “cover” (Tavaluc 2019). These are benign pathologies of the vocal cords, responsible for organic dysphonia, the main etiopathological factor of which is an acute or chronic vocal abuse/misuse disorder.
Vocal cord nodules are acquired lesions that underlie a chronic vocal disorder. Frequency is higher in women and in certain professional categories that require high vocal performance (singers, teachers, etc.). They develop in an almost symmetrical manner (kissing nodules) between the middle and anterior thirds of the edge of the vocal cord, a critical area of higher contact and pressure during speech. They may appear as an initial thickening in that area due to an edematous reaction of the lamina propria and, subsequently, undergo a fibrous involution due to the infiltration of fibroblasts: if the condition is diagnosed early, they can be treated conservatively. In the latter case, the therapeutic gold standard is surgery (Altman 2007).
Vocal cord polyps more frequently appear as a unilateral sessile or pedunculated neoformation, although possible association with reactive or congenital contralateral lesions is reported (cysts, sulci, vergetures). They are also related to vocal abuse, most often an acute trauma, which results in an inflammatory edema and hemorrhage with segmentary herniation of the superficial layer of the lamina propria (Altman 2007).
Vocal cord cysts may be acquired, in the case of mucous retention cysts, or, more frequently, congenital. In the latter case, the cyst has a white/mother of pearl aspect and is defined as epidermoid, as it is thought to be the result of an inclusion in the lamina propria of epidermis residues during embryogenesis. The cyst is located in the middle third of the cord, uni- or bilaterally, it may be associated to “sentinel” varices and results in a lack of mucosal vibration when viewed with a stroboscope. Treatment typically consists in surgery and may be difficult, due to the frequent instances of adhesion to the vocal ligament (Altman 2007). It should be pointed out that opening an intracordal cyst in early childhood can result, following the progressive growth in length of the glottis, in the appearance of secondary lesions, such as sulci (invagination of the cord mucosa), vergetures (atrophic depression on the free margin of the cords) and mucosal bridges (due to the creation of a double channel of communication between the cysts), which are also characterized by a close connection to the ligament layer and susceptible to resolution by surgery (Giovanni 2007).
Similar ultra-structural alterations of the Superficial Layer of the Lamina Propria (SLLP) are found in Reinke’s edema, also defined as smokers’ hyperplastic chronic laryngitis. In this case, the damage caused to the micro-vessels by inflammation may be correlated to smoking and affects the so-called Reinke’s space as a whole. The condition affects both vocal cords, albeit differently, and results in the characteristic laryngostroboscopic aspect, with increased amplitude of the vocal cycle associated to lowering of the fundamental frequency (Sakae 2008).
In all cases of benign pathologies described above, phono-surgical treatment plays a major role and aims to preserve the anatomic integrity of the structures of the glottis and restore appropriate speech function. Surgical treatment alone, however, may not guarantee immediate results: in many cases, supporting medical treatment and logopedic rehabilitation may be useful (Isshiki 2000; Kacker 1997). The rationale for the use of anti-inflammatory drugs in the early post-operative stages depends not just on their edema-preventing action but also on their possible role in regulating the tissue reparation processes, in order to avoid possible anomalous scarring. The sub-continuous administration of NSAIDs, however, is not recommended following any surgical operation, due to its possible effect on the coagulation cascade. The use of systemic corticosteroids is not recommended either. To address this, it is common for phono-surgery to be followed by a post-operative protocol that entails the use of steroids by inhalation, so as to obtain a direct action of the drug on the site of the operation. This type of treatment is not unanimously accepted and may not be devoid of contraindications. Adverse effects on the mucosa of the larynx and on vocal performance following the use of corticosteroids by inhalation have been amply proven in the literature for groups of patients suffering from bronchial asthma who underwent long-term treatment (Williams 1983).
It is precisely for this reason that the introduction of food supplements, whose effect as remedies has been recognized since antiquity, may be a possible alternative to corticosteroids. Natural products with anti-inflammatory properties, in fact, have long been used for inflammatory conditions, such as fever, pain, migraines and arthritis (Yuan 2006). Among these products, extracts of Boswellia serrata and bromelain have been used to counter various types of inflammation, with proven effectiveness (Italiano 2019, Fusini 2016, Ghensi 2017, Mataro 2017, Ammon 2016).
Bromelain is a proteolytic enzyme, a natural active ingredient found in pineapple, particularly effective in the treatment of soft tissue inflammation and traumas, of localized inflammation, in particular in the presence of edema and also in the case of post-operative tissue reactions (Bromelain review 2010). In vitro studies have proven that bromelain may selectively inhibit the thromboxane-synthase enzyme, limiting the conversion of prostaglandin H2 (a product of the catabolism of arachidonic acid) in prostaglandins and thromboxanes. The edema-suppressing action, in particular, is due to the increase of anti-inflammatory cytokines compared to their pro-inflammatory counterparts, pulling phlogogen cells and fluids from the extracellular space towards the vascular compartment (Maurer 2001).
Boswellia is a tree that grows in India, from which a resin is extracted that contains more than 12 different types of boswellic acids. Boswellic acids can significantly reduce the production of leukotrienes by 5-lipoxygenase. They act as an allosteric regulator of the enzyme, inhibiting it. The action is dose-dependent and takes place through a direct, non-redox and non-competitive mechanism that inhibits the synthesis of the 5-HETE catabolite (a metabolite of the arachidonic acid synthesis) and of leukotriene B4 that act on chemotaxis towards the phlogogen site and on capillary permeability (Ammon 2016).
The anti-inflammatory, fibrinolytic and anti-edematous action of the bromelain + boswellic acids complex means the drug is now routinely used in various inflammation conditions.
Their use, therefore, nowadays widely accepted in the treatment of osteoarticular and upper airways pathologies, could also be useful as post-operative adjuvant treatment of benign lesions of the vocal cords. The analysis of current scientific literature shows a clear lack of clinical data regarding the effectiveness of bromelain and/or boswellic acid in the adjuvant post-operative treatment of benign lesions of the vocal cords.
In this study, therefore, we studied the use of EVAN® (Ananas comosus titrated in bromelain and Boswellia serrata titrated at 65% in boswellic acids) on a group of patients who underwent phono-surgery for the treatment of benign lesions of the vocal cords. The results, in terms of tissue repair and recovery of adequate vocal performance, were compared to those obtained in a similar cohort of patients who received the standard treatment which entailed the use of corticosteroids by inhalation.
MATERIALS AND METHODS
Patients
This study examines 56 patients with benign conditions of the vocal cords, whom we observed in the period from February to June 2018. The sample assessed included 30 men (53.6%) and 26 women (46.4%) with a M/F ratio of 1.15% and whose ages ranged from 34 to 58. Of these, 23 patients mentioned, when their medical history was taken, that smoking formed part of their lifestyle, while 5 cases had a known background of gastroesophageal reflux.
This study excluded patients who, on undergoing pre-operative clinical observation with optic fiber laryngoscopy, presented with objective suspicions of pre-cancerous lesions or neoplasms. Other exclusion criteria related to evidence, while the medical history was being taken, of previous operations on the vocal cords (phono-surgery and/or cordectomy) or a history of prolonged orotracheal intubation, due to the possible scarring effects on the glottis.
Similarly, the study did not include patients who had undergone radiotherapy for tumors in the head-neck area, due to the possible presence of radiation-induced fibrosis sequelae.
The patients provided informed consent for their participation in the study.
Surgery and parameters analyzed
All patients underwent transoral phono-surgery with MLDS (Microdirect Laryngoscopy Suspension), an endoscopic procedure under general anesthesia.
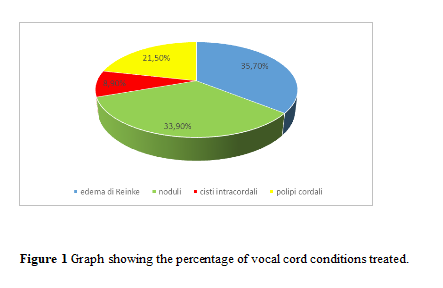
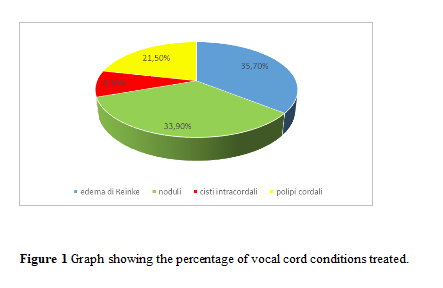
The following conditions affecting the vocal cords were found, shown in Figure 1:
19 cases of kissing nodules of the vocal cords, where excision with the Microflap technique was performed;
5 cases of intracordal cysts, treated with a similar technique;
12 cases of vocal cord polyps.
Pre-operative assessment entailed the performance of preliminary fibro-laryngoscopic investigation and stroboscopy; this not only made it possible to assess the morphology of the larynx and to identify the macroscopic characteristics of the lesions to the cords, but also to study the fundamental frequency and the transmission dynamics of the mucosal wave.
The main stroboscopy parameters assessed are as follows:
Amplitude: distance between the median line and the free edge of the vocal cords during opening and closure.
Regularity of the vibration cycles.
Symmetry of the progression of the mucosal wave on the two sides.
Glottic closure: conformation of the glottal plane on closure and any insufficiency.
In addition, perceptive analysis of the voice was performed during prolonged vocal emission and conversational voice and a pre-operative score was calculated for each patient by using the GRBAS scale (Yamaguchi 2003), a widely used method for perceptive assessment of the quality of the voice that is based on the following parameters:
Grade = total dysphonia score.
Roughness = irregular fluctuation of the fundamental frequency F°.
Breathiness = noise produced by the outflow of air.
Asthenia = grade of vocal weakness.
Strain = tension, excessive vocal effort.
A score from 0 to 3 was assigned to each parameter of the scale:
0 = normal
1 = slight alteration
2 = moderate alteration
3 = severe alteration
Treatment
The patients who underwent surgery were divided into two groups, as consistent as possible, by number of cases, age, pathology and consequent surgical technique. The 28 patients of Group A (cases) were treated, post-operatively, with EVAN® (BIOHEALTH ITALIA srl, Turin): Ananas comosus titrated in bromelain (80 mg) + boswellic acids titrated at 65% (750 mg) with a dose of 2 tablets or sachets/day for a week. For Group B (control), which included the remaining 28 cases, instead, a standard treatment with corticosteroids by inhalation for 7 days was recommended.
The stroboscopy parameters and the perceptive analysis of the voice were assessed during the early post-operative follow-up and at three months from surgery, so as to compare the morpho-functional results in the two groups treated.
Statistical Analyses
The statistical method used to study the possible correlation between improvement of the GRBAS score post-operatively and group was linear regression with Dummy variable.
RESULTS
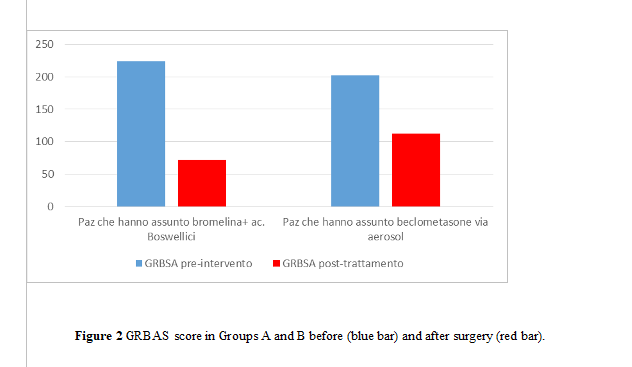
A pre-operative GRBAS score was calculated for each patient candidate for phono-surgery with direct microlaryngoscopy. The phoniatric reassessment of the patients in both groups took place approximately two weeks after surgery. Aside from assessment with optic fiber laryngoscopy with stroboscopy, the aforementioned score was recalculated. In Group A patients, who used EVAN®, it was found, already during the early post-operative period, a faster disappearance of the dysphonia symptoms and of asthenia. Stroboscopy showed gradual improvement of the main parameters examined (amplitude, regularity, symmetry, closure). The improvement of the GRBAS score following the procedure was calculated, in terms of difference in percentages, compared to that obtained before surgery. As a whole, in Group A the combined treatment with phono-surgery and administration of bromelain/boswellic acids resulted in a 67.86% reduction of the GRBAS score against 44.55% in Group B, who underwent phono-surgery and standard aerosol treatment (Figure 2).
Starting with the assumption that both groups of patients had undergone preliminary phono-surgery, we decided to perform the study of linear regression with Dummy variable in order to assess the correlation between intake of the drug tested and improvement of the GRBAS score by individual patient. In patient Group A, who took EVAN® after surgery, a higher improvement of the score was observed compared to the pre-operative values than in the control Group B. The results obtained showed that this difference in the GRBAS indicator in the early post-operative stages was, therefore, correlated in a statistically significant manner (p-value = 0.000000108) with post-operative adjuvant treatment with EVAN®. Conversely, the data of the two groups on reassessment 3 months following surgery were comparable.
DISCUSSION
The purpose of this research was to perform a preliminary study of the clinical effectiveness of a food supplement made with Ananas comosus titrated in bromelain and Boswellia serrata titrated at 65% in boswellic acids (EVAN®) in patients with benign pathologies of the vocal cords (Reinke’s edema, kissing vocal cord nodules, intracordal cysts, vocal cord polyps). In patients who were assigned the post-operative therapeutic protocol with bromelain and boswellic acids, a faster recovery of the qualitative parameters of vocal functionality and a significant reduction of the post-operative GRBAS score were observed, compared to the control group who were treated with corticosteroids by inhalation. These results, although preliminary, are of fundamental importance since there are no clinical data on the effectiveness and safety of bromelain and/or boswellic acids in the post-operative treatment of benign pathologies of the vocal cords. The standard protocol for this type of operations currently entails the administration of oral steroids, a treatment that has critical side effects. Lavy et al (2000), in fact, describe voice alterations in 50% of cases of asthma patients in treatment with steroids by inhalation, with 22 patients showing the simultaneous presence of stroboscopic larynx alterations: irregularity of the vocal cycle, supraglottic hyperfunction, reduction of the maximum phonation time. Further, mucosal damage with reduction of the barrier functions (Salturk 2018) was found, higher susceptibility to fungal infections (Saha 2016), and, lastly, a peculiar case of steroid-induced myasthenia of the adductor muscles of the larynx. Similarly, Mirza et al (2004) showed that 8 out of 10 patients with persistent dysphonia presented with mucosal alterations and alterations of the stroboscopic parameters (reduction of vibration amplitude and of the propagation of the mucosal wave) following treatment with steroids and bronchodilators by inhalation. Furthermore, there have been reports of cases of infective laryngitis caused by atypical microorganisms (mycobacteria) in immunocompetent subjects under local treatment with steroids, as further confirmation of their harmful effect on the mucosal barrier (Wang 2008). Although the post-operative treatment with local steroids was shorter than in the cases reported in the literature, such treatment can increase the feeling of dryness, altering the normal hydrolipidic film of the mucosa of the larynx at the level of the glottis, slow down the reparative processes and be poorly tolerated by patients who suffer from laryngopharyngeal reflux. However, treatment with bromelain + boswellic acids may avert, as shown in this study, such rather severe undesired effects. The two substances act through different action mechanisms, acting on different cascades of the inflammation mechanism, most likely by creating a synergetic effect which reduces inflammation and has an anti-edematous action. The action mechanism of the boswellic acids unfolds by inhibiting the pro-inflammatory process through its effect on 5-lipoxygenase, cyclooxygenase and the complement system (Prabhavathi 2014). Bromelain, consisting of a combination of cysteine proteases, acts through various mechanisms: it increases the action of the fibrinolytic system, it reduces the levels of fibrinogens in the plasma, and reduces the levels of bradykinin, which, in turn, reduces vascular permeability and edema. In addition, it is able to reduce Prostaglandin 2 and Thromboxane A2 (Brien 2004).
To date, the combination of bromelain and boswellic acids used in this study has only been employed in a study by Italiano et al (2019) on 49 patients who suffered from various forms of arthrosis (knee, hip, generalized arthrosis) with the aim of improving their quality of life. The authors show that the patients had marked improvements in performing daily activities that were impaired before the treatment, proving that EVAN® is an effective alternative tool available to patients with arthrosis.
The results of our study and of the Italiano study prove that the combination of bromelain + boswellic acids is safe and effective in the treatment of acute and chronic inflammation.
CONCLUSION
The treatment of benign conditions of the vocal cords with bromelain + boswellic acids has been found to be effective in terms of tissue repair and recovery of adequate vocal performance in patients who underwent phono-surgery.
These phyto-therapeutic active ingredients, therefore, may be indicated in the post-operative stage for patients who underwent surgery for a benign laryngeal condition, due to their action preventing the formation of edemas, inhibiting chemotaxis, and modulating fibroblast activation without potential mucosal damage, also in the case of prolonged treatment.
BIBLIOGRAPHY
Altman KW. Vocal fold masses. Otolaryngol Clin North Am. 2007 Oct;40(5):1091-108, viii.
Ammon HP. Boswellic Acids and Their Role in Chronic Inflammatory Diseases. Adv Exp Med Biol. 2016;928:291-327.
Brien S, LewithG, Walker A, Hicks SM, Middleton D. Bromelain as a Treatment for Osteoarthritis: a Review of Clinical Studies. Evid Based Complement Alternat Med. 2004;1(3):251–257.
Bromelain. Monograph. Altern Med Rev. 2010 Dec;15(4):361-8.
Franic DM, Bramlett RE, Bothe AC. Psychometric evaluation of disease specific quality of life instruments in voice disorders. J Voice. 2005 Jun;19(2):300-15.
Fusini F, Bisicchia S, et al. Nutraceutical supplement in the management of tendinopathies: a systematic review. Muscles Ligaments Tendons J. 2016 May 19;6(1):48-57.
Ghensi P, Cucchi A, Creminelli L, Tomasi C, Zavan B, Maiorana C. Effect of Oral Administration of Bromelain on Postoperative Discomfort After Third Molar Surgery. J Craniofac Surg. 2017 Mar;28(2):e191-e197. doi: 10.1097/SCS.0000000000003154.
Giovanni A, Chanteret C, Lagier A. Sulcus vocalis: a review. Eur Arch Otorhinolaryngol. 2007 Apr;264(4):337-44. Epub 2007 Jan 13.
Hirano M. Morphological structure of the vocal cord as a vibrator and its variations. Folia Phoniatr (Basel). 1974;26(2):89-94.
Isshiki N. Mechanical and dynamic aspects of voice production as related to voice therapy and phonosurgery. Otolaryngol Head Neck Surg. 2000 Jun;122(6):782-93.
Italiano G, Raimondo M, Giannetti G, Gargiulo A. Benefits of a Food Supplement Containing Boswellia serrata and Bromelain for Improving the Quality of Life in Patients with Osteoarthritis: A Pilot Study. J Altern Complement Med. 2019 Nov 1. doi: 10.1089/acm.2019.0258. [Epub ahead of print]
Kacker SK. Phonosurgery and other voice improvement techniques .Med J Armed Forces India. 1997 Apr; 53(2): 127–130.
Lavy JA, Wood G, Rubin JS, Harries M Dysphonia associated with inhaled steroids. J Voice. 2000 Dec;14(4):581-8.
Mataro I, Delli Santi G, Palombo P, D’Alessio R, Vestita M. Spontaneous healing and scar control following enzymatic debridement of deep second-degree burns. Ann Burns Fire Disasters. 2017 Dec 31;30(4):313-316.
Maurer HR. Bromelain: biochemistry, pharmacology and medical use. Cell Mol Life Sci. 2001 Aug;58(9):1234-45.
Mirza N, Kasper Schwartz S, Antin-Ozerkis D. Laryngeal findings in users of combination corticosteroid and bronchodilator therapy. Laryngoscope. 2004 Sep;114(9):1566-9.
Mohamed Tap F, Abd Majid FA et al. In Silico and In Vitro Study of the Bromelain-Phytochemical Complex Inhibition of Phospholipase A2 (Pla2). Molecules. 2018 Jan 19;23(1).
Prabhavathi K, Chandra US, Soanker R, Rani PU. A randomized, double blind, placebo controlled, cross over study to evaluate the analgesic activity of Boswellia serrata in healthy volunteers using mechanical pain model. Indian J Pharmacol. 2014 Sep-Oct;46(5):475-9. doi: 10.4103/0253-7613.140570.
Saha A, Saha K, Chatterjee U. Primary aspergillosis of vocal cord: Long-term inhalational steroid use can be the miscreant. Biomed J. 2015 Dec; 38(6):550-553. doi: 10.1016/j.bj.2015.09.001. Epub 2016 Mar 15.
Sakae FA, Imamura R, Sennes LU, Mauad T, Saldiva PH, Tsuji DH. Disarrangement of collagen fibers in Reinke’s edema. Laryngoscope. 2008 Aug;118(8):1500-3.
Salturk Z, Kumral T L, Uyar Y. Histopathological Analysis of the Effects of Corticosteroids on Vocal Cords: Experimental Study. Indian J Otolaryngol Head Neck Surg (Jan–Mar 2018) 70(1):111–114.
Tavaluc R, Tan-Geller M. Reinke’s Edema. Otolaryngol Clin North Am. 2019 Aug;52(4):627-635. doi: 10.1016/j.otc.2019.03.006. Epub 2019 May 14.
Wang BY, Amolat MJ, Woo P, Brandwein-Gensler M. Atypical mycobacteriosis of the larynx: an unusual clinical presentation secondary to steroids inhalation. Ann Diagn Pathol. 2008 Dec;12(6):426-9.
Williams AJ, Baghat MS, Stableforth DE, Cayton RM, Shenoi PM, Skinner C. Dysphonia caused by inhaled steroids: recognition of a characteristic laryngeal abnormality. Thorax 1983 Nov;38(11):813-821
Yamaguchi H, Shrivastav R, Andrews ML, Niimi S. A comparison of voice quality ratings made by Japanese and American listeners using the GRBAS scale. Folia Phoniatr Logop. 2003 May-Jun;55(3):147–157.
Yuan G, Wahlqvist ML, He G, Yang M, Li D. Natural products and anti-inflammatory activity. Asia Pac J Clin Nutr. 2006;15(2):143-52.
Zhang Z. Mechanics of human voice production and control. J Acoust Soc Am. 2016 Oct;140(4):2614.
Comments (0)