
Remember me


CERVICAL OSTEOPHYTES: A RARE CAUSE OF ACUTE DYSPNEA.
Report of 2 cases with different evolution and literature review.
O. Marotta*- N. Maione°- V. Marotta^
*Casa di Cura S. Patrizia – Napoli
° Ospedale S. Paolo – Napoli
^Universita’ A.Moro – Bari
Introduction
Osteophytes are ‘‘fibrocartilage-capped bony outgrowths’’, which can be caused by an excessive cellular overgrowth in response to a chronic irritating stimulus (1), such as:
traction at the insertion of tendons and ligaments
inflammatory processes as in ankylosing spondylitis
repeated fiction at the junction between cartilage and bone (genuine osteophyte or chondro-osteophyte).
Osteophytosis of the anterior face of cervical spinal tract occur in 20% to 30% of the general population. It more frequently affects the elderly population linked to senile degenerative skeletal alterations (2), (3),(4). Anterior cervical osteophytes can be isolated or diffuse. Usually they are idiopathic and part of a form called Forestier disease (diffuse idiopathic skeletal hyperostosis – DISH), firstly described in 1950 (5), but they could also be caused by traumatic, infectious, iatrogenic (eg. spinal surgery) factors (2).
In case of involvement of the anterior face of the cervical vertebrae, chronic inflammation phenomena can also involve the mucosa of the upper airways-digestive tract in correspondence of bone neoformations (intrinsic reactive inflammatory hyperplasia of the hypopharynx and esophagus) (6).
Generally, cervical osteophytes are asymptomatic and so the diagnosis is often occasional. Nevertheless, rarely they can have a significant clinical impact: in case of anterior cervical hyperostosis, mechanical obstruction of the pharyngo-esophageal segment may cause dysphagia, which is the most frequent symptom complained, but also foreign body sensation, cough, dysphonia and dyspnea (7) (8). In addition, very rarely, osteophytes of the spine can cause acute respiratory distress, even resulting in life-threatening situations (9).
Here we report two cases of symptomatic anterior cervical osteophytes, one successfully treated by medical therapy, the other complicated by severe respiratory deficit and requiring a prompt tracheotomy.
case report
Case 1
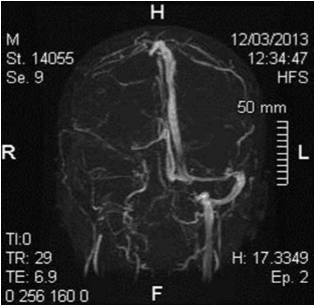
A 71- year-old man presented with dyspnea and progressive solids dysphagia resulting in a moderate loss of weight. Pharyngeal and laryngeal examination showed a bulging of the posterior wall of hypopharynx covered by healty mucosa and pooling of saliva in the left piriform sinus, while glottis was not sufficiently viewable. Neck motion was not decreased. CT and NMR imaging showed osteophytes of the bodies of C5 to C7 [Fig-1]. No other bony spurs were identified on radiographs of the thoracic and lumbar spine. In addition, there was evidence of asymmetry of the laryngeal vestibule and dislocation of the cricoid and esophagus to the right side. Since the high anesthesiology risk, surgical excision of osteophytes was not executed. Only 4 months later, patient returned to the Emergency complaining with severe difficulty in breathing, quickly deteriorate in respiratory insufficiency. Emergency tracheotomy and percutaneous endoscopic gastrostomy were needed in order to restore the correct pulmonary ventilation and the correct feeding respectively.
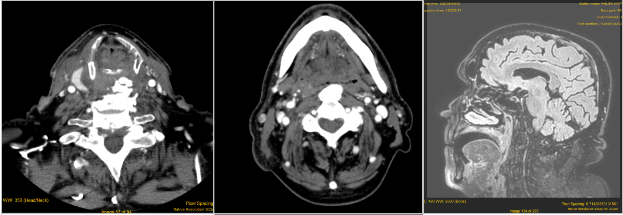
Fig 1: a) e b): TC images of osteophytosis of cervical spine. c) NMR imgage showing occlusion of the upper airway tract due to osteophyte.
Case 2
A 67-year-old male presented with progressive dysphagia since about 6 months. Patient didn’t complained with pain neither with difficulty in breathing nor with change in voice. Laryngoscopy revealed a bulging of the posterior-left pharyngeal wall, partially obstructing the pharynx and limiting the complete view of larynx which appeared normal. CT scan showed many osteophytes of the anterior face of cervical vertebrae with mild signs of inflammation regarding pero-popharyngeal-laryngeal tissues, with no evidence of occlusion of upper aero-digestive tract [Fig-2]. Orthopedic and neurosurgery consultants were asked for further management, but patient refused surgical treatment. He started exclusive medical treatment with anti-inflammatory and anti-reflux therapy getting a little improvement on symptoms initially referred. At one-year follow-up, the patient still refers occasional acute symptomatic episodes successfully treated by medical drugs.
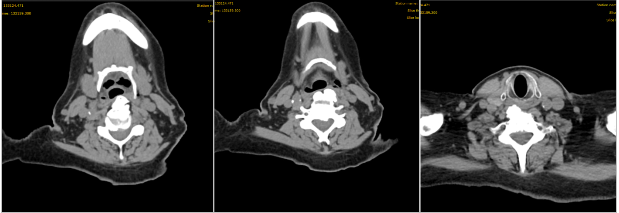
Fig.2: case 2, ostephitosys of cervical spine.
discussion
Dyspnea and dysphagia due to skeletal causes are rare entities. According to Grandville et al.(10), about 10% of people presenting with progressive dysphagia has cervical osteophytes. Specialists should always be aware of this entity in order to be able to recognize it promptly, treat it and follow it adequately over time.
Anterior cervical osteophytes are benign lesions, usually asymptomatic, which can be commonly found in elderly population, probably linked to degenerative process of osteoarthritis of the cervical spine, with estimated incidence up to 30% of the population (2), (3)(4). Many different terms are used to describe this condition, such as ankylosing hyperostosis, diffuse idiopathic skeletal hyperostosis (DISH), Forestier’s disease, cervical ankylosing, or simply cervical osteophytosis. Even if these lesions are often asymptomatic, sometimes cervical osteophytes can cause annoying troubles not to underestimate.
According to data actually available, dysphagia for solid is recorded in 6—28% of these cases and, together with foreign body sensation in throat, it is the most frequent described symptom (3). Since C5 – C6 are the most common vertebrae involved (40%), followed by C4 – C5 (23%) (11), lesions of these tracts can result in mechanical compression of pharynx and esophagus and/or in inflammation of para-esophageal tissues, explaining why swallowing difficulty is the most common and initial symptom. Over time, dysphagia for liquid and cough can appear too.
Laryngeal and respiratory symptoms due to anterior cervical osteophytes are even more rarely described. As suggested by Matan et al. (6), respiratory symptoms may result from pressure on the posterior laryngeal tract and/or from inflammatory processes involving posterior crico-arytenoid muscle caused by the constant movement of the cricoid lamina over a projecting osteophytic mass. A recent review on Forster’s disease found out that mild and moderate airway obstruction was present in 6% and in 12% of the population studied respectively (12), while only few Authors reported about cases requiring emergency tracheotomy for acute airway obstruction (4) (11), (6) (13), (14), (15).
Radiological examinations are essential to exclude other causes of dysphagia and dyspnea (expansive processes, injury, neurological impairment, diverticula, pharyngeal or esophageal stenosis) should always be investigated.
Therapeutic planning is based on symptoms, health general condition and pathogenic mechanisms of each patient. For symptomatic patients, surgical excision of osteophytes should be the golden choice of treatment in order to avoid severe complications such as deficit in feeding and respiratory distress. It may be performed by anterior approach and meticulous blunt dissection is needed in order to avoid any mucosal injuries. Moreover, given that large osteophytes can irritate the pharynx and esophagus causing inflammatory hyperplasia, Matan et al. suggest to carefully evaluate intrinsic esophageal or pharyngeal reactive inflammatory mass so to treat both external and internal obstruction causes (6).
When surgical excision of bone lesions is not possible, tracheostomy may be required to avoid acute respiratory distress and/or even death, as well as a percutaneous gastrostomy (PEG) may be useful to ensure adequate nutritional intake.
The two different cases of cervical osteophytosis that we reported exemplify the two pathogenic mechanisms previously described. In fact, although none of them was treated by surgical osteophytectomy, they showed different evolution of the symptoms, thus requiring different management.
Emergency tracheotomy was required for first patient affected by a giant osteophyte of cervical vertebrae largely projecting into hypopharynx and causing severe dysphagia and respiratory difficulties since it almost completely closed upper aero-digestive tract threatening the life of patient.
On the other hand, milder symptoms were complained by second patient, who was able to gain sufficient relief just with medical drugs. In this case, dysphagia could be caused by inflammatory processes affecting the hypopharyngeal-laryngeal mucosa rather than to the “space-occupying lesion” as in previous case.
The different pathogenesis of osteophytes may explain the different response to medical treatment. In any case, surgical excision of symptomatic osteophytes should always be the gold standard; if it cannot be performed or in presence of an important reduction of respiratory space, it’s advisable to program tracheotomy to perform in election and not in emergency.
To this day, clear guidelines still don’t exist for this disease. From our point of view, studies with longer follow-up would be very useful in order to evaluate the probability of sudden worsening of a well-drug-managed osteophytosis. In this regard, Mauri et al. reported about a case of long time dysphagia (2 years) suddenly deteriorated in respiratory distress (16)
CONCLUSIONS
Anterior cervical osteophytes are common but rarely symptomatic finding in the elderly population, still today often underestimated in the clinical practice. Dysphagia is the most common symptom complained while dyspnea is only in few case reported. Since airway obstruction due to cervical osteophytes is very uncommon, clinicians should be aware of this entity and should be able to recognized it promptly because an emergent tracheotomy could be required.
Nevertheless, surgical multidisciplinar treatment with collaboration between ENT and spine specialists is the best choice of treatment in order to avoid the arise of sudden complications life threatening.
BIBLIOGRAFIA
1. Menkes CJ, Lane NE. Are osteophytes good or bad? Osteoarthritis Cartilage. 2004, 12(Suppl A):S53-4.
2. Yasin Kür?ad Varsak, Mehmet Akif Eryilmaz, Hamdi Arba?. Dysphagia and Airway Obstruction Due to Large Cervical. The Journal of Craniofacial Surgery. 2014, p. 25(4):1402-1403.
3. Lecerf P, O. Malard. How to diagnose and treat symptomatic anterior? European Annals of Otorhinolaryngology, Head and Neck diseases. 2010, p. 127, 111—116.
4. Nelson RS, Urquhart AC, Faciszewski T. Diffuse idiopathic skeletal hyperostosis: a rare cause of Dysphagia, airway obstruction, and dysphonia. J Am Coll Surg. 2006 , p. 202(6):938-42.
5. Forestier J, Rotes-Querol J. Senile ankylosing hyperostosi of the spine. . Ann Rheum Dis. 1950, 9:32130.
6. Matan AJ, Hsu J, Fredrickson BA. Management of respiratory compromise caused by cervical osteophytes: a case report and review of the literature. Spine J. 2002, p. 2:456—9.
7. Aronowitz P, Cobarrubias F. Images in clinical medicine. Anterior cervical osteophytes causing airway compromise. N Engl J Med . 2003, p. 25;349(26):2540.
8. Aydin K, Ulug T, Simsek T. Case report: bilateral vocal cord paralysis caused by cervical spinal osteophytes. . Br J Radiol . 2002, p. 75(900):990-1033.
9. Caminos CB, Cenoz IZ, Louis CJ, Otano TB, Esáin BF, Pérez de Ciriza MT. Forestier disease: an unusual cause of upper airway obstruction. American Journal of Emergency Medicine. 2008, p. 26:1072-1–1072-3.
10. Grandville LJ, Musson N, Altman R, et al. Anterior cervical osteophytes as a cause of pharyngeal stage dysphagia. . J Am Geriatr Soc . 1998, p. 46:1003—7.
11. Walid I. Dagher, Viviane G. Nasr, Anju K. Patel, Daniel W. Flis, Richard O. Wein. AN UNUSUAL AND RARE CAUSE OF ACUTE AIRWAY OBSTRUCTION. The Journal of Emergency Medicine. 2014, p. 46(5). 617–619, .
12. Jorrit-Jan Verlaan, Petronella F.E. Boswijk, BS, Jacob A. de Ru, Wouter J.A. Dhert, F. Cumhur One. Diffuse idiopathic skeletal hyperostosis of the cervical spine:an underestimated cause of dysphagia and airway obstruction. The Spine Journal. 2011, p. 11:1058–1067.
13. AD., Hassard. Cervical ankylosing hyperostosis and airway obstruction. Laryngoscope. 1984, 94(7):966-8.
14. Demuynck K, Van Calenbergh F, Goffin J, et al. Upper airway obstruction caused by a cervical osteophyte. Chest . 1995, p. 108:283–4.
15. Solomons NB, Linton DM, Potgeiter PD. Cervical osteophytes and respiratory failure. S Afr Med J . 1987, p. 71:259–60.
16. JC, Giroux. Vertebral artery compression by cervical osteophytes. . Adv Otorhinolaryngol . 1982;, p. 28:111-7.
17. Maiuri F, Stella L, Sardo L, Buonamassa S. Dysphagia and dyspnea due to an anterior cervical osteophyte. Arch Orthop Trauma Surg. 2002 , 122(4):245-7.
18. D., Stuart. Dyspliagia due to cervical osteophyres. A description of five patients and a review of tlie literature. Int Ortho. 1989, 13:95-99.
Comments (0)