nan12781-sup-0001-Supplementary Information.docxWord 2007 document
, 7.7 MB
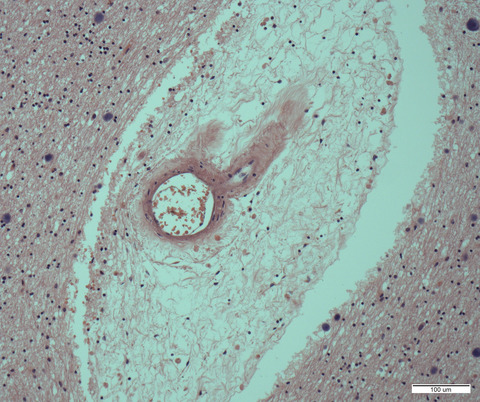
Figure S1. Representative gross and histological images of AD-related neuropathology. a1-a7: frontal cortex, b1-b7 hippocampus, and c1-c7: occipitomedial region. A1: Moderate frontal and more prominent superior and middle temporal atrophy is observed at gross examination. A2, A3: Moderate neuronal loss and mild superficial spongiosis is observed in frontal cortex. A4, A5: A high density of diffuse and primitive ßA4-deposits is observed, dense or core-plaques are less frequent. There is no amyloid angiopathy. A6, A7: There is a high load of tau-positive neurofibrillary pathology with abundant neuropil threads throughout the whole cortical laminae and frequent neurofibrillary tangles (AT8 antibody). B1: The hippocampal formation shows no obvious gross (B1) or microscopic atrophy (B2, B3). B4, B5: ß-Amyloid-deposits are also only moderate in frequency with typical fleecy or lake-like deposits in the entorhinal region. B6, B7: In contrast, tau positive neurofibrillary pathology is extensive and involves mostly the CA1 sector of the hippocampus, the subiculum, the ento- and transentorhinal regions as well as the temporo-occipital cortex (AT8 antibody). C1-C3: No prominent atrophy of the area striata and parastriata is observed. C4, C5: In contrast, there is relative prominent ßA4-plaque pathology with more diffuse and primitive deposits in the area parastriata and more cored plaques in the area striata. C6-C7: Tau-immunoreactive neurofibrillary pathology is extensive and involves prominently the area parastriata and somewhat less the area striata (lower part of the image in C6 and C7; AT8 antibody). Scale bars: 3mm in A2, A4, A6, B2, B4, B6 and C2, C4, C6; 300μm in A3, A5, A7, and B5, B7, and 1mm in B3, C3, C5 and C7.
Figure S2. Figure 2: Neuropathological details of AD neuropathological changes. A-C: Tau immunoreactive neurofibrillary pathology consisting of a high density of fine neuropil threads and intraneuronal neurofibrillary tangles (A). Dystrophic neurites around amyloid cores were only rarely observed, particularly in the amygdala (B, C). D-F: Varying morphology of ßA4-deposits from diffuse, patchy, perineuronal and more compact or primitive deposits (D, E) to classical cored plaques (F). G-I: On conventional haematoxylin-eosin stained sections superficial spongiosis was observed (G), extracellular amyloid plaques appear as some clustered amorphous deposits (H) and some typical core-plaques surrounded by reactive astrocytes and some microglial nuclei (I, arrow). Scale bars: 20μm in A and G, 10μm in B-F and in H-I
Figure S3. IHC negative controls. Tissue sections were incubated with blocking solution without primary antibodies, followed by incubation with secondary HRP antibodies and DAB detection reagents. No signal was detected in any case ensuring that staining of all proteins included in the study is specific. Scale bar=20μm
Figure S4. Experimental validation of the modified AT protocol. Representative images of the same case using the standard AT protocol for fresh brain samples (A-D) and the modified protocol for PFA-fixed brain samples (E-H). Amyloid plaques were stained with NAB61 antibody (red) and presynaptic terminals with an anti-SYPH antibody (green). Inset of a presynaptic Aβ aggregate (D,H). Quantification analysis of 3 plaques per condition show similar SYPH densities and colocalization between NAB61 and SYPH in the samples treated following the standard AT protocol compared with those treated following the modified AT protocol (I).
Table S1. Neuropathological data of cases included in the study.

Comments (0)