
Remember me
Acute ST-elevation myocardial infarction (STEMI) is associated with changes in left ventricular (LV) functional parameters where STEMI patients experience states of stunned LV and LV dilatation.1,2 These states are accompanied with dyssynchronous LV contractions, which could form the basis for associated myocardial stunning and LV dysfunction.3–4
These changes are primarily the result of acute ischemic insults and ongoing infarction process. It has been postulated that restoring blood flow in infarction related artery would restore LV synchronicity and alleviate LV stunning and dilatation conditions.5
Assessment of LV mechanical dyssynchrony has been a matter of study, using a variety of imaging techniques. Majority of conducted studies examined LV dyssynchrony in heart failure and old myocardial infarction patients.6–10
Left ventricular dyssynchrony is also evident in various cardiac conditions, for example, acute myocardial infarction, intraventricular conduction abnormalities, and severe valvular dysfunction.4,10–12
Previous studies documented a temporary condition of stunned myocardium and LV dilatation that accompanies STEMI, which has been accompanied by LV dyssynchrony and regional wall motion abnormalities.1–4
This state of LV dyssynchrony has been examined in the context of STEMI using transthoracic echocardiography evaluation.13 There have been recent articles using advanced modalities, for example, strain analysis and 3-D techniques to examine LV dyssynchrony in STEMI patients but still these techniques are not widely available with limited reproducibility and operator-dependent issues.14–15
Phase analysis of gated single-photon emission computed tomography (SPECT) MPI was introduced by Chen et al.16 This triggered further research, utilizing LV phase analysis to study LV dyssynchrony.17–18 Phase analysis offers a feasible, reproducible, method of quantifying LV dyssynchrony.19 Chen has demonstrated that stress-induced myocardial ischemia was associated with LV mechanical dyssynchrony.20 Abdelbary et al. have also concluded that LV dyssynchrony may be acquired acutely very early in STEMI and may have a negative impact on LV ejection fraction.4
The aim of our work was to evaluate LV functional parameters and dyssynchrony, shortly after primary percutaneous coronary intervention (PCI) and 5–7 days later in the setting of STEMI and documents temporal changes in LV functional parameters and dyssynchrony indices, examines the relationship between stunned myocardium, LV dilatation and LV dyssynchrony, and 28-days mortality.
2 MethodsThis was a prospective non-randomized observational study. All patients signed written consent and the study was approved by the research council in Cairo University. This study was performed at critical care department, Cairo University, from January 2018 to December 2019. A nuclear cardiology laboratory is integrated into our critical care department that could serve for acute imaging protocols. Inclusion criteria were first onset acute STEMI patients who were eligible for primary PCI, admitted to the critical care department Cairo University. We excluded STEMI Patients with a history or ECG evidence of old myocardial infarction (9), cardiomyopathy (5), left bundle branch block (7), patients who are not eligible for primary PCI or unstable for interdepartmental transfer (11), ECG evidence of topographic location of other than an exclusive anterior or inferior STEMI (6), dysrhythmias that precluded gating artefacts (12) and the refusal of myocardial perfusion imaging (10). Six patients died before completion of study protocol and were not included in analysis.
STEMI diagnosis was based upon the European Society of Cardiology/ACCF/AHA/World Heart Federation Task Force for the Universal Definition of Myocardial Infarction which includes characteristic symptoms of myocardial ischemia associated with ST segment elevation and subsequent rise in serum biomarkers.21
Rest gated Technitium99m Sestamibi Myocardial perfusion study was performed. First, Myocardial Perfusion images were acquired using the 17-segment scoring system. Second, LV functional parameters were derived (LV end-diastolic volume LVEDv, LV end-systolic volume LVESv and LV ejection fraction LVEF). Third, Phase images were examined for LV dyssynchrony parameters; the latter included the histogram bandwidth and histogram standard deviation (SD).16
The “Step and shoot” protocol was used (180° elliptical orbit with 32 projections). Images were acquired, using dual head gamma camera with high resolution, low energy collimator (Symbia E, Siemens Medical Solutions USA, Inc., IL), and utilizing Cedars-Sinai software, USA, 2009 (8 frames per cycle). Images were gated to the R-wave of the ECG, and image acquisition was interrupted for one beat if the R–R interval varied by 15% of the preceding R–R interval.22 The images were reviewed and interpreted by 2 senior operators, blinded to the ECG and PCI data.
Five to seven days later, patients were re-injected with 20–30 mCi Tc-99mSestamibi intravenously to acquire the second set of gated SPECT images; Processing of both sets of images could reflect myocardial perfusion indices (MAR: Myocardium at risk and IS: infarction size).22
The LV functional parameters (volumes and EF) were measured from the rest gated images based on the method described by Germano et al. Perfusion defects were interpreted and quantified using the 17 segments scoring system available in the Cedars-Sinai QPS package 2009.23 Phase analysis of gated SPECT was done as described by Chen, to document histogram bandwidth (HBW) and histogram standard deviation (HSD).16 We used the methodology described by Boogers et al. for phase analysis and distribution using the Cedars-Sinai QGS software.23
2.1 Statistical methodsNumerical variables were described as Mean ± standard deviation (SD). Median values were stated for non-normally distributed data. Categorical variables were described as proportions. Comparisons were done using Mann–Whitney test and “U” values were reported. Chi-square test was used for comparison of categorical variables. Wilcoxon Signed Ranks Test was used for paired comparisons. P value was considered significant if ≤.05. Delta changes, that is, percent of change was calculated as the difference between second reading and first reading, divided by first reading. Statistics were calculated using SPSS 21 package.24
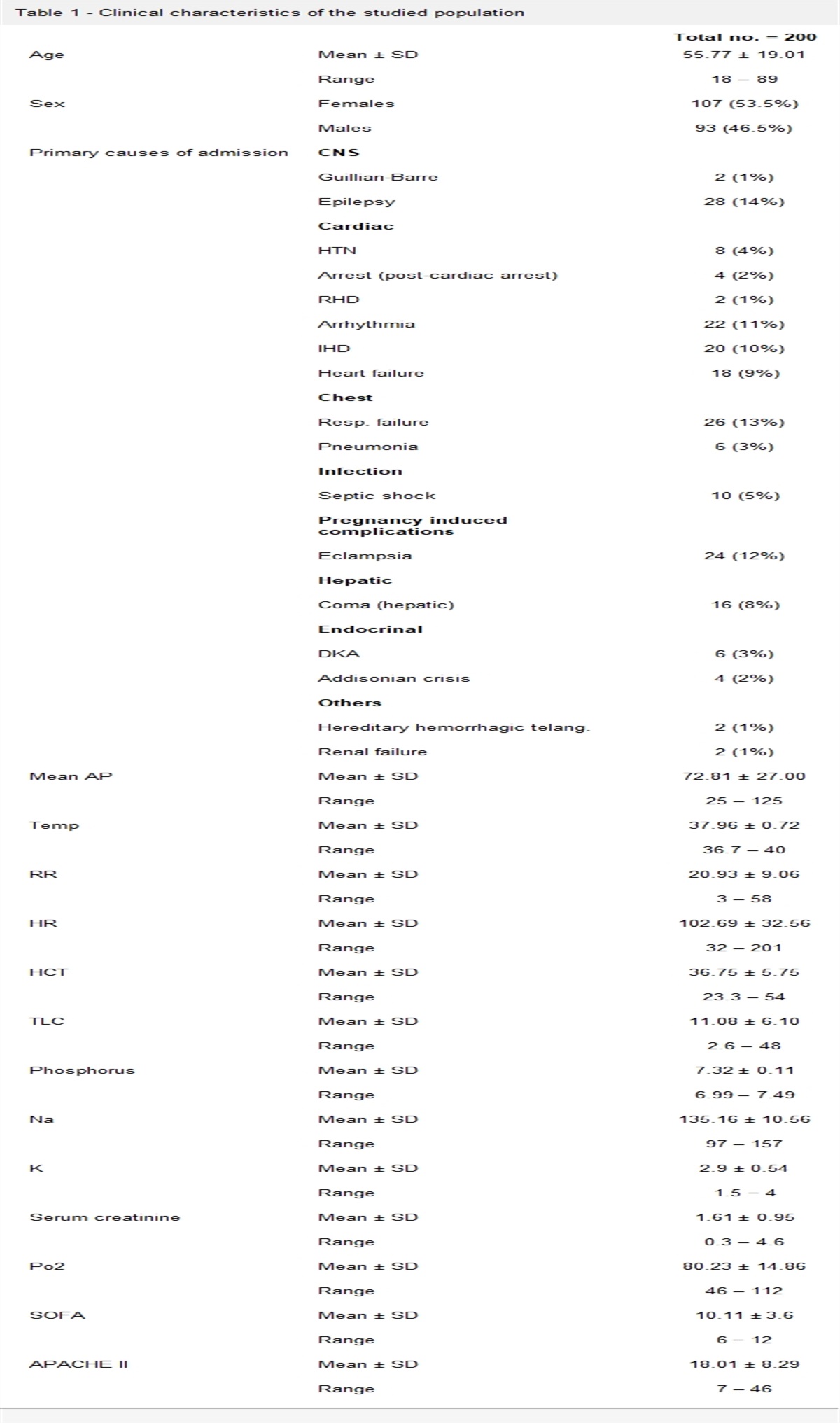
3 ResultsSixty patients were recruited in our study. Average age was 54.0 ± 10.4 years old with average length of stay of 6.8 ± 3.4 days. Males comprised 90.0% of our study population. Mortality was 11.7%. Table 1 showed our STEMI patients data for myocardial perfusion indices, LV functional parameters and LV dyssynchrony parameters. Survivors showed significant improvement in LVED and LVES (P .001 and .02, respectively) but no significant change in LVEF. However, non-survivors showed non-significant changes in LV volumes and significant worsening of LVEF (P .018). Changes in HSD was significant in both survivors (P .001) and non-survivors (P .018).
Table 1 - Myocardial perfusion indices, functional parameters, and dyssynchrony parameters for all patients and for survivors vs non-survivors ALL (N. 60) Survivors (N. 53) Non-survivors (N. 7) P Myocardial perfusion indices MAR 33.0 ± 16.0 (36.0) 31.6 ± 16.0 (35.0) 43.9 ± 11.3 (43.0) .065 IS 21.2 ± 16.4 (22.5) 20.1 ± 15.2 (22.0) 29.6 ± 23.7 (30.0) .402 LV functional parameters First set of images LVED 133.0 ± 88.7 (112.5) 122.5 ± 77.6 (109.0) 212.4 ± 129.6 (183.0) .016 LVES 89.7 ± 82.1 (68.5) 80.4 ± 73.6 (61.0) 160.1 ± 112.7 (121.0) .013 LVEF 39.0 ± 16.8 (36.0) 40.5 ± 17.1 (36.4) 27.9 ± 9.0 (26.4) .041 Second set of images LVED 115.3 ± 64.9 (92.0) 105.8 ± 48.1 (89.0) 187.4 ± 120.2 (187.0) .030 LVES 75.1 ± 60.1 (54.5) 64.8 ± 41.8 (48.0) 153.0 ± 111.4 (143.0) .009 LVEF 40.2 ± 14.1 (37.2) 42.7 ± 12.9 (39.5) 21.9 ± 7.2 (22.4) .001 LV dyssynchrony parameters First set of images HBW 77.4 ± 54.1 (60.0) 70.2 ± 50.8 (54.0) 132.0 ± 49.5 (150.0) .004 HSD 21.1 ± 15.0 (17.3) 19.3 ± 14.4 (14.5) 34.5 ± 13.7 (37.5) .009 Second set of images HBW 72.0 ± 51.9 (48.0) 61.2 ± 42.1 (42.0) 153.6 ± 48.4 (158.0) <.001 HSD 17.9 ± 13.9 (11.4) 15.0 ± 11.0 (11.1) 39.4 ± 15.8 (46.4) .002HBW, histogram bandwidth; HSD, histogram standard deviation; IS, infarction size; LV, left ventricular; LVEF, left ventricular ejection fraction; MAR: myocardium at risk.
Multiple regression model with bootstrapping technique showed that LVEF, changes in LVEF, histogram SD (second image) were significant predictors of 28-days mortality as seen in Table 2 (Nagelkerke R2 0.917 and goodness of fit statistics 1.891). Multivariate regression analysis showed also that changes in LV dyssynchrony was a significant predictor of changes in both LVES and LVEF as seen in Table 3. Disconcordance between direction of changes in LVEF and direction of changes in histogram SD was 75.0%. Concordance between direction of changes in LVES and direction of changes in histogram SD was 73.3%.
Table 2 - Multiple regression analysis (Bootstrapping technique) to determine contributing LV functional and dyssynchrony parameters to predict 28-days mortalityMortality 95% CI B P Bias Lower Upper LVEF (second reading) –0.154 .004 –1.133 –4.519 –0.094 LVEF delta change –8.525 .002 –43.350 –166.639 –5.087 HSD (second reading) 0.086 .013 0.734 0.024 2.938HSD, histogram standard deviation; LV, left ventricular; LVEF, left ventricular ejection fraction.
HSD, histogram standard deviation; LVEF, left ventricular ejection fraction.
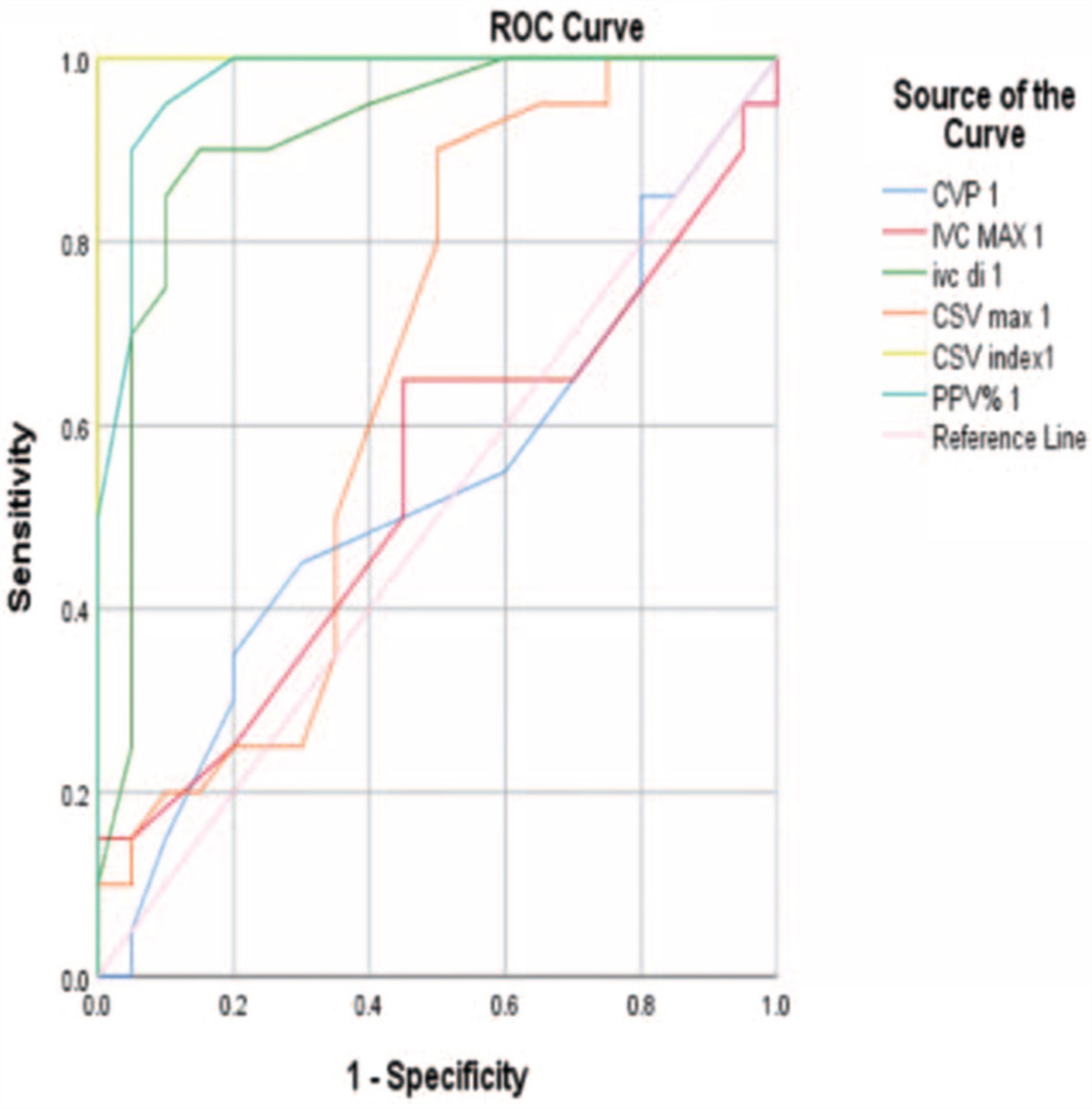
Receiver operating curve was examined for cut-offs for LVEF and histogram SD. LVEF ≤ 25% showed sensitivity 85.7% and specificity 96.2% to predict 28-days mortality (Area under curve 0.737). Histogram SD ≥ 34∘ showed sensitivity 85.7% and specificity 88.7% to predict 28-days mortality (Area under curve 0.798). Kaplan–Meier analysis was done for impact of LVEF and histogram SD upon mortality with Log Rank test reported in Figures 1 and 2.
 Figure 1:
Figure 1: Kaplan–Meier curve to examine survival in those with HSD < 34° (interrupted line) vs those with HSD ≥ 34° (solid line). Log Rank test reported (P .001). HSD values are those of second image readings.
 Figure 2:
Figure 2: Kaplan–Meier curve to examine survival in those with LVEF > 25% (interrupted line) vs those with LVEF ≤ 25% (solid line). Log Rank test reported (P < .001). LVEF values are those of second image readings.
Recruited patients in our study included 39 patients with anterior STEMI (32 patients survived, and 7 patients died) and 21 patients with inferior STEMI (all survived). There was no significant difference in age or prevalence of risk factors for coronary artery disease (CAD) between anterior and non-anterior STEMI. Anterior STEMI patients showed substantially higher perfusion defects with impaired functional and dyssynchrony parameters, compared to inferior infarcts as illustrated in Table 4. Inferior STEMI group showed within-normal LV functional parameters and better synchronization parameters with no significant change during the hospital course of STEMI patients. Anterior STEMI group who survived showed significant improvement in LVED, LVES, and HSD (P .001, .001, and .002, respectively). Anterior STEMI group who died showed significant worsening in LVEF and HSD (P .018 both). LV phase analysis for both anterior (non-survivor) and inferior (survivor) STEMI were included for illustrative purposes in Figures 3 and 4.
Table 4 - Myocardial perfusion indices, functional parameters and dyssynchrony parameters for inferior infarcts vs anterior infarcts (survivors) vs anterior infarcts (non-survivors) STEMI Inferior infarcts (survivors) Anterior infarcts (survivors) Anterior infarcts (non-survivors) Myocardial perfusion indices MAR 24.7 ± 15.7 (22.0) 36.1 ± 14.8 (39.5) 43.9 ± 11.3 (43.0) Infarction size 14.1 ± 13.8 (9.0) 24.0 ± 15.0 (26.5) 29.6 ± 23.7 (30.0) LV functional parameters First set of images LVED 87.4 ± 36.9 (80.0) 145.6 ± 88.5 (117.5) 212.4 ± 129.6 (183.0) LVES 49.3 ± 31.9 (37.0) 100.8 ± 85.7 (78.0) 160.1 ± 112.7 (121.0) LVEF 46.7 ± 15.6 (48.6) 36.4 ± 17.0 (30.1) 27.9 ± 9.0 (26.4) Second set of images LVED 84.5 ± 38.4 (81.0) 119.7 ± 49.3 (109.5) 187.4 ± 120.2 (187.0) LVES 47.8 ± 36.1 (40.0) 76.0 ± 42.0 (72.5) 153.0 ± 111.4 (143.0) LVEF 47.2 ± 12.9 (44.4) 39.7 ± 12.3 (35.9) 21.9 ± 7.2 (22.4) LV dyssynchrony parameters First set of images HBW 54.3 ± 38.2 (36.0) 80.6 ± 55.7 (75.0) 132.0 ± 49.5 (150.0) HSD 15.1 ± 11.3 (9.6) 22.1 ± 15.6 (19.5) 34.5 ± 13.7 (37.5) Second set of images HBW 48.8 ± 36.8 (34.0) 69.4 ± 43.9 (51.0) 153.6 ± 48.4 (158.0) HSD 12.6 ± 9.6 (8.6) 16.6 ± 11.7 (11.7) 39.4 ± 15.8 (46.4)HBW, histogram bandwidth; HSD, histogram standard deviation; LV, left ventricular; LVEF, left ventricular ejection fraction; MAR: myocardium at risk.
 Figure 3:
Figure 3: Left ventricular gated SPECT phase analysis of patient, presenting with anterior STEMI. His phase analysis show marked decrease in count amplitudes afecting mainly apex, the anterior wall and septum. First set of images showed histogram BW: 223.0 ms (84.8°) and histogram SD: 67.0 ms (25.5°). Second set of images showed histogram BW: 158.0 ms (60.1°) and histogram SD: 35.0 ms (13.3°). R-R 946 ms (360°). Anterior STEMI data showed increased dispersion of dyssysnchrony parameters, denoting dyssynchronous LV contractions. This improved partially in the coming days, following primary PCI.
 Figure 4:
Figure 4: Left ventricular gated SPECT phase analysis of patient, presenting with inferior STEMI. His phase analysis show marked decrease in count amplitudes afecting mainly the posterior segment. First set of images showed histogram BW: 49.0 ms (28.9°) and histogram SD: 10.0 ms (4.9°). Second set of images showed histogram BW: 32.0 ms (15.6°) and histogram SD: 8.0 ms (3.9°). R-R 739 ms (360°). Inferior STEMI data showed near-normal dyssynchrony parameters and these parameters did not change dramatically in the coming days, following primary PCI.
4 DiscussionSeveral studies have shown that LV dyssynchrony can occur early after acute MI. (4) Others have shown that LV dyssynchrony was related to long-term LV contractile performance and LV remodeling.
Dyssynchrony affects both systolic and diastolic functions. Fornwalt proposed a method of quantifying internal flow to examine LV dyssynchrony using cardiac magnetic resonance (CMR) cine images. He examined heart failure patients (candidate for CRT) and reported that internal flow could occur up to 9.9% ± 5.0% versus 1.5% ± 0.5% in normal controls. Dyssynchrony could be associated with internal flow loss which might explain further decline in stroke volume with systolic dysfunction and subsequent increase in LVED pressures and volumes.25
Nucifora examined 129 patients with acute STEMI and concluded that LV dyssynchrony is related to LVEF and has an additional detrimental effect on LV function, beyond infarct size and the anterior location of AMI.26 Mollema also examined 178 patients with acute MI and concluded that LV dyssynchrony immediately after acute myocardial infarction predicts LV remodeling at 6-month follow-up.10
Our results suggested that myocardial stunning, temporary LV dilatation and dyssynchronous LV contractions were same flips of one coin. Multivariate regression showed that changes in LV dyssynchrony, notably histogram SD was a closely related to changes in dilated and stunned LV conditions. Similar findings were reported by Nucifora where he examined changes in LV systolic functions and synchronicity in acute myocardial infarction settings and concluded that the reduction in LV dyssynchrony independently influenced LV functional recovery in these patients.27–28
Our analysis also showed that myocardium at risk, quantified using Gated SPECT technique, could affect changes in histogram SD. Closely, Manka showed in the acute phase of infarction, LV dyssynchrony is closely related to the extent of edema revealed by CMR technique and was suggested that LV dyssynchrony might be a transitory phenomenon.29
In our study, we tried to explore temporal pattern of LV dyssynchrony and its relation to cardiovascular 28-days mortality. We could trace significant improvement in survivors, regarding LV functional parameters and synchronization profiles. Non-survivors showed no significant changes, regarding their functional and dyssynchrony parameters. Temporal changes could be explained by the restoration of myocardial blood flow and reduction in the perfusion defect which was followed by functional recovery of the infarct zone, counteracting the deleterious effects of myocardial stunning and reversing temporary LV dilatation and dyssynchrony. Lack of temporal improvements in LV functional and dyssynchrony parameters could signify higher risk status.
Multiple regression analysis was run to determine possible contributing LV functional and dyssynchrony parameters to predict mortality, showing that LVEF, changes in LVEF and histogram SD were significant contributors. LV contractile performance is recognized for its prognostication in STEMI settings.30 LV dyssynchrony is also recognized a risk factor for cardiovascular mortality in acute and chronic myocardial infarction. Shin has examined LV dyssynchrony in acute MI settings and concluded that LV dyssynchrony is independently associated with increased risk of death. However, he mentioned several technical limitations in his study including poor data quality in 37% of his patients that might have affected his results.31
Our study explored LV functional and dyssynchrony parameters in both anterior and inferior STEMIs. Anterior STEMI showed worse functional parameters with higher dispersion in dyssynchrony parameters. LV volumes and HSD improved significantly in anterior STEMI group. On the contrary, inferior STEMI group showed within-normal LV functional parameters and better synchronization parameters with no significant change during the hospital course of STEMI patients. An association between myocardial perfusion indices, stunning myocardium, dilated LV dimensions, LV dyssynchrony and infarction characteristics (size and location), has been confirmed in previous studies.32–34 Possibly, our method of Gated SPECT examines LV dyssynchrony and that inferior myocardial infarctions are usually accompanied by right ventricular stunning.35–36
Comparing different subgroups showed that inferior STEMI group showed within-normal LV functional parameters and better synchronization parameters with no significant change during the hospital course of STEMI patients. Anterior STEMI group who survived showed significant improvement in LV volumes and LV dyssynchrony parameters. Anterior STEMI group who died showed significant worsening in LVEF and dyssynchrony parameters.
What we observed along analyzing our data, contractile performance showed an excellent relation to adverse outcomes in STEMI. Dyssynchrony profile and temporal changes could add to the prediction of adverse outcomes as well.
In chronic MI conditions, complicated with HF, regaining synchronicity has been targeted in HF using CRT to alleviate LV dyssynchrony. This has been associated with improvement in contractile performances.37 Similarly, could biventricular pacing play a role in alleviating LV dyssynchrony in STEMI patients? Would alleviating LV dyssynchrony be associated with improvements in LV functional parameters? How would biventricular pacing affect patients’ outcome? This warrants further studies.
4.1 LimitationsOur study was a single center study with relatively small number of recruited patients. Besides, overestimation of infarct size due to early imaging protocols. In addition, underreporting of ischemic time (pain to door time) and time to intervention (door to balloon time) might have confounding effect on comparing perfusion indices in both groups. Lack of long-term follow-up data and no control group to confirm role of revascularization on improvements in LV functional and dyssynchrony parameters.
5 ConclusionChanges in dyssynchronous LV contraction patterns were coupled with changes in LV functional parameters. LV contractility and dyssynchrony parameters could predict 28-days mortality in STEMI patients as well.
AcknowledgmentAlaa Abdelhay BSc (Faculty of science, physics Department, Cairo University) has participated in data collection.
References [1]. Bhave PD, Hoffmayer KS, Armstrong EJ, et al. Predictors of depressed left ventricular function in patients presenting with ST-elevation myocardial infarction. Am J Cardiol 2012;109(3):327–331. doi: 10.1016/j.amjcard.2011.09.015. [2]. Mateus PS, Dias CC, Betrencourt N, et al. Left ventricular dysfunction after acute myocardial infarction--the impact of cardiovascular risk factors. Rev Port Cardiol 2005;24(5):727–734. [3]. Zhang Y, Chan AK, Yu CM, et al. Left ventricular systolic asynchrony after acute myocardial infarction in patients with narrow QRS complexes. Am Heart J 2005;149(3):497–503. [4]. Abdelbary A, Abdelhay A, Khedr MH, Emam M, Tohamy K. Early left ventricular dyssynchrony in acute ST elevation myocardial infarction: a gated single photon emission computed tomography study. EJCCM 2016;4:85–95. [5]. Ahmed W, Samy W, Tayeh O, Behairy N, Abd El Fattah A. Left ventricular scar impact on left ventricular synchronization parameters and outcomes of cardiac resynchronization therapy. Int J Cardiol 2016;222:665–670. doi: 10.1016/j.ijcard.2016.07.158. [6]. Yu CM, Chau E, Sanderson JE, et al. Tissue Doppler echocardiographic evidence of reverse remodeling and improved synchronicity by simultaneously delaying regional contraction after biventricular pacing therapy in heart failure. Circulation 2002;105(4):438–445. [7]. Wang J, Wang Y, Zhang X, Zhou R, Niu R, Lu P. Left ventricular systolic synchrony assessed by phase analysis of gated myocardial perfusion imaging in patients with old myocardial infarction. Zhonghua Xin Xue Guan Bing Za Zhi 2015;43(7):599–604. [8]. Chalil S, Stegemann B, Muhyaldeen S, et al. Intraventricular dyssynchrony predicts mortality and morbidity following cardiac resynchronization therapy: a study using cardiovascular magnetic resonance tissue synchronization imaging. J Am Coll Cardiol 2007;50:243–252. [9]. Ahmed W, Samy W, Tayeh O, Behairy N, Fattah A. Temporal changes of left ventricular synchronization parameters and outcomes of cardiac resynchronization therapy. EJCCM 2016;4(2):105–112. doi: 10.1016/j.ejccm.2016.04.00. [10]. Mollema SA, Liem SS, Suffoletto MS, et al. Left ventricular dyssynchrony acutely after myocardial infarction predicts left ventricular remodeling. J Am Coll Cardiol 2007;50(16):1532–1540. [11]. Trimble MA, Borges-Neto S, Smallheiser S, et al. Evaluation of left ventricular mechanical dyssynchrony as determined by phase analysis of ECG-gated SPECT myocardial perfusion imaging in patients with left ventricular dysfunction and conduction disturbances. J Nucl Cardiol 2007;14(3):298–307. [12]. Bax JJ, Poldermans D. Mitral regurgitation and left ventricular dyssynchrony: implications for treatment. Heart 2006;92(10):1363–1364. doi:10.1136/hrt.2006.089805. [13]. Azazy AS, Soliman M, Yaseen R, Mena M, Sakr H. Left ventricular dyssynchrony assessment using tissue synchronization imaging in acute myocardial infarction. Avicenna J Med 2019;9(2):48–54. doi:10.4103/ajm.AJM_168_18. [14]. Moon J. Prognostic implication of strain analysis in patients with ST-segment elevation myocardial infarction: one more evidence for ever-debatable topic. J Cardiovasc Ultrasound 2016;24(2):108–109. doi:10.4250/jcu.2016.24.2.108. [15]. Alam I, Haque T, Badiuzzaman M, Masud AA, Kaiser A, Moniruzzaman M. Left ventricular dyssynchrony in acute ST elevated myocardial infarction in patients with normal QRS duration. Bangladesh Heart J 2015;30(1):13–21. [16]. Chen J, Garcia EV, Folks RD, et al. Onset of left ventricular mechanical contraction as determined by phase-analysis of ECG gated myocardial perfusion SPECT imaging: development of a diagnostic tool for assessment of mechanical dyssynchrony. J Nucl Cardiol 2005;12(6):687–695. [17]. Boogers MM, Chen J, Bax JJ. Myocardial perfusion single photon emission computed tomography for the assessment of mechanical dyssynchrony. Curr Opin Cardiol 2008;23(5):431–439. [18]. Henneman MM, Chen J, Dibbets P, et al. Can LV dyssynchrony as assessed with phase analysis on gated myocardial perfusion SPECT predicts response to CRT? J Nucl Med 2007;48:1104–1111. [19]. Trimble MA, Velazquez EJ, Adams GL, et al. Repeatability and reproducibility of phase analysis of gated SPECT myocardial perfusion imaging used to quantify cardiac dyssynchrony. Nucl Med Commun 2008;29:374–381. [20]. Chen CC, Shen TY, Chang MC, et al. Stress-induced myocardial ischemia is associated with early post-stress left ventricular mechanical dyssynchrony as assessed by phase analysis of Tl-201 gated SPECT myocardial perfusion imaging. Eur J Nucl Med Mol Imaging 2012;39:1904–1909. [21]. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction: on behalf of the joint ESC/ACCF/AHA/WHF task force for the redefinition of myocardial infarction. Eur Heart J 2007;28(20):2525–2538. [22]. Hesse B, Lindhardt TB, Acampa W, et al. EANM/ESC guidelines for radionuclide imaging of cardiac function. Eur J Nucl Med Mol Imag 2008;35(4):851–885. [23]. Germano G, Kiat H, Kavanagh P, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36:2138–2147. [24]. IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp. [25]. Fornwalt BK, Gonzales PC, Delfino JG, Eisner R, Leon AR, Oshinski JN. Quantification of left ventricular internal flow from cardiac magnetic resonance images in patients with dyssynchronous heart failure. J Magn Reson Imaging 2008;28(2):375–381. [26]. Nucifora G, Bertini M, Marsan NA, et al. Impact of left ventricular dyssynchrony early on left ventricular function after first acute myocardial infarction. Am J Cardiol 2010;105(3):306–311. doi: 10.1016/j.amjcard.2009.09.028. [27]. Nucifora G, Bertini M, Ajmone Marsan N, et al. Temporal evolution of left ventricular dyssynchrony after myocardial infarction: relation with changes in left ventricular systolic function. Eur Heart J Cardiovasc Imaging 2012;13(12):1041–1046. doi:10.1093/ehjci/jes095. [28]. Ng AC, Tran da T, Allman C, Vidaic J, Leung DY. Prognostic implications of left ventricular dyssynchrony early after non-ST elevation myocardial infarction without congestive heart failure. Eur Heart J 2010;31(3):298–308. doi:10.1093/eurheartj/ehp488. [29]. Manka R, Kozerke S, Rutz AK, Stoeck CT, Boesiger P, Schwitter J. A CMR study of the effects of tissue edema and necrosis on left ventricular dyssynchrony in acute myocardial infarction: implications for cardiac resynchronization therapy. J Cardiovasc Magn Reson 2012;14(1):47. doi:10.1186/1532-429X-14-47. [30]. Chehab O, Qannus AS, Eldirani M, Hassan H, Tamim H, Dakik HA. Predictors of in-hospital mortality in patients admitted with acute myocardial infarction in a developing country. Cardiol Res 2018;9(5):293–299. doi:10.14740/cr772w. [31]. Shin SH, Hung CL, Uno H, et al. Mechanical dyssynchrony after myocardial infarction in patients with left ventricular dysfunction, heart failure, or both. Circulation 2010;121(9):1096–1103. doi:10.1161/CIRCULATIONAHA.109.863795. [32]. Sciagrà R, Imperiale A, Antoniucci D, et al. Relationship of infarct size and severity versus left ventricular ejection fraction and volumes obtained from 99mTc-sestamibi gated single-photon emission computed tomography in patients treated with primary percutaneous coronary intervention. Eur J Nucl Med Mol Imaging 2004;31:969. doi:10.1007/s00259-004-1482-4. [33]. Christian TF, Gibbons RJ, Gersh BJ. Effect of infarct location on myocardial salvage assessed by technetium-99m isonitrile. J Am Coll Cardiol 1991;17(6):1303–1308. [34]. Nakai H, Takeuchi M, Otani K, et al. Assessment of left ventricular dyssynchrony in myocardial infarction using 2D speckle tracking imaging. J Echocardiogr 2008;6:109–118. [35]. Alam M, Wardell J, Andersson E, Samad BA, Nordlander R. Right ventricular function in patients with first inferior myocardial infarction: assessment by tricuspid annular motion and tricuspid annular velocity. Am Heart J 2000;139(4):710–715. [36]. Ramzy IS, O'Sullivan CA, Lam YY, Dancy M, Tei C, Henein MY. Right ventricular stunning in inferior myocardial infarction. Int J Cardiol 2009;136(3):294–299. doi: 10.1016/j.ijcard.2008.05.021. [37]. Pouleur AC, Knappe D, Shah AM, et al. Relationship between improvement in left ventricular dyssynchrony and contractile function and clinical outcome with cardiac resynchronization therapy: the MADIT-CRT trial. Eur Heart J 2011;32(14):1720–1729. doi: 10.1093/eurheartj/ehr185
Comments (0)