
Remember me
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection.1 Early diagnosis and stratification of sepsis severity play a central role in patient management by increasing the possibility of starting timely and specific treatment. If delayed antimicrobial treatment, sepsis dysfunction can lead to global tissue hypoxia, direct tissue damage, and ultimately to multiple organ failure.2
Development of a more useful tool for risk stratification and prognosis in sepsis is thus still essential. For this purpose, the predisposition, infection, response, and organ dysfunction (PIRO) concept was proposed. The 4 components of the PIRO system cover almost all of the factors that may influence the onset, development, and outcome of sepsis. The PIRO system is an ideal staging system that incorporates assessment of premorbid baseline susceptibility (predisposition), the specific disorder responsible for illness (infection), the response of the host to infection, and the resulting degree of organ dysfunction.3
There are many scoring systems to predict the outcome of the critically-ill patients in the intensive care unit (ICU), Acute Physiology and Chronic Health Evaluation (APACHE II) is found to be accurate in predicting hospital mortality in septic shock cases requiring ICU admission with good calibration.4 The predominant score in current use is the Sequential Organ Failure Assessment (SOFA).5 SOFA has been recommended (along with a less validated, more clinical tool called “quick SOFA” or qSOFA) for assessment of patients with sepsis by the 2016 Sepsis Definitions Consensus Statement. A higher SOFA score is associated with an increased probability of mortality.5 Serum lactate is a potentially useful biomarker that is widely investigated in critically-ill patients and gave good prognostic values. It can predict mortality and organ dysfunction.6
2 Aim of the studyThe aim of our study was to assess the predictive performance of the PIRO system for development of multiple organ dysfunction (MOD), 28-day mortality in sepsis in the ICU setting, days of ICU stay, and ICU readmission within 28 days. Also we aimed to compare PIRO scoring system with the APACHE II and SOFA scoring systems.
3 Materials and methodsWe conducted a prospective cohort study in the period between July 2015 and October 2016 on 50 adult patients who were admitted with a proven diagnosis of sepsis or developed septic shock during their ICU stay at El Helal Hospital (20 cases) and Egyptian Railway Medical Hospital (30 cases). The inclusion criteria were patients who have criteria of sepsis syndrome (according to the 2012 international guidelines for management of sever sepsis and septic shock) and age ≥ 18 years. The exclusion criterion was age <18 years.
3.1 Data collectionPatients basic information, including age, sex, and comorbidities were recorded at the time of enrollment. Vital signs (systolic blood pressure, mean arterial pressure, heart rate, respiratory rate, temperature, and urine output) and Glasgow coma scale (GCS) were evaluated at the day of admission, 2nd, and 3rd days. Routine laboratory investigation was withdrawn at 1st, 2nd, and 3rd days including complete blood count. Arterial blood gases: arterial blood gases sample was sent immediately after admission for analysis. Liver function tests, including bilirubin. Kidney function tests: creatinine and BUN; electrolyte: Na, K. Blood sample for lactate assay was withdrawn on 1st, 2nd, and 3rd days. The PIRO, APACHE II, and SOFA scores were calculated using data obtained on 1st, 2nd, and 3rd days of admission.
3.2 Outcome variablesAll patients were followed up for 28 days through medical records or by telephone. In-hospital mortality within 28 days, development of MOD, length of stay, and ICU readmission within 28 days were considered as the outcome criteria. The patients were classified as survivors and non-survivors.
3.3 Statistical analysisThe data was coded and entered using the statistical package SPSS 20.0. All quantitative data were expressed as mean and standard deviation. Qualitative data were expressed as frequencies and percentage. Independent t test was used to compare 2 groups for all continuous normally distributed data. Receiver operating characteristic curve analysis was used to find out the overall predictivity of parameter in and to find out the best cut-off value with detection of sensitivity and specificity at this cut-off value. Sensitivity is true positive rate while specificity is false positive rate. AUC which equals 100% for a perfect test and 50% for a completely uninformative test. Binary logistic regression: was used to predict the outcome of categorical variable based on one or more predictor variables. Spearman correlation coefficient test was used to test a positive or negative relationship between 2 variables probability (P-value). P-value ≤ .05 was considered significant.
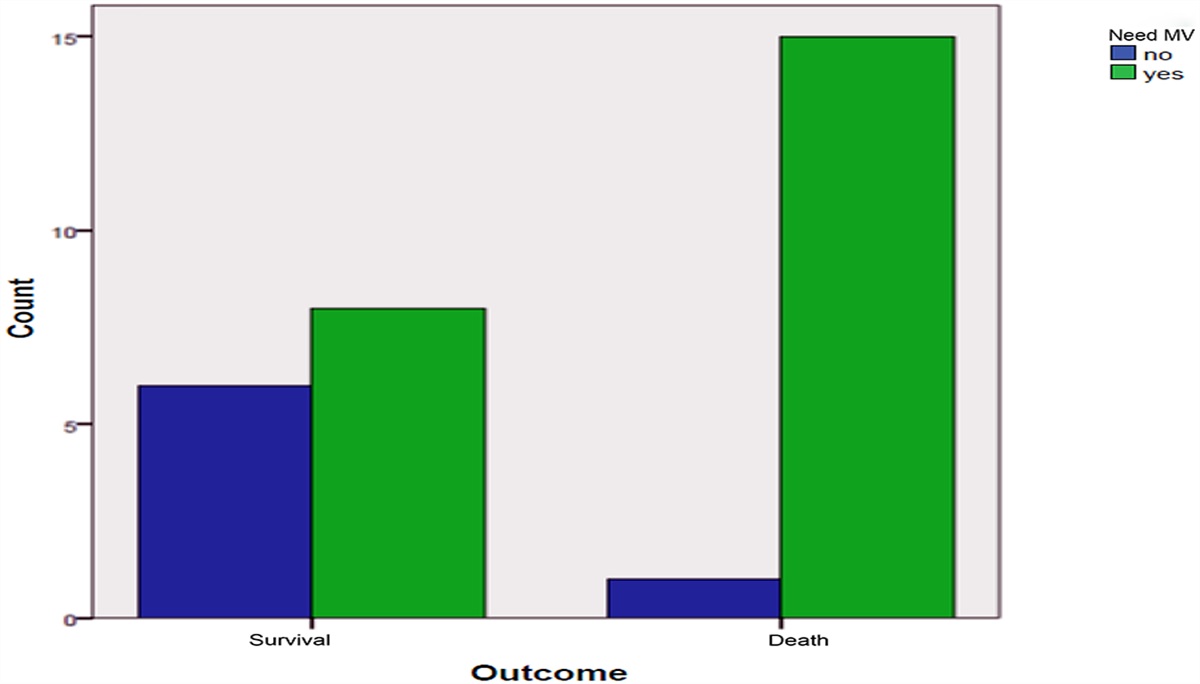
4 Results 4.1 Characteristics of the study cohortThe study included 41 (82%) males and 9 (18%) females. The mean age for the whole studied patients was 67.02 ± 13.13 years. The mean ICU stay was 17.24 ± 7.65 days. Twenty-eight patients (56%) did not survive, while 22 patients (44%) survived and were discharged. Three patients (6%) were readmitted to ICU within 28 days. The current study included 50 septic patients, 35patients had been diagnosed as septic shock. The remaining 15 patients had organ dysfunction (13 survivors and 2 non-survivors). Fifteen patients (53%) of the non-survivor group (28 patients) needed mechanical ventilation compared to only 8 patients (36%) from the survivor group (22 patients). Two patients (7%) of non-survivor group (28 patients) need dialysis in the first 3 days compared to no patients (0%) from the survivor group (22 patients).
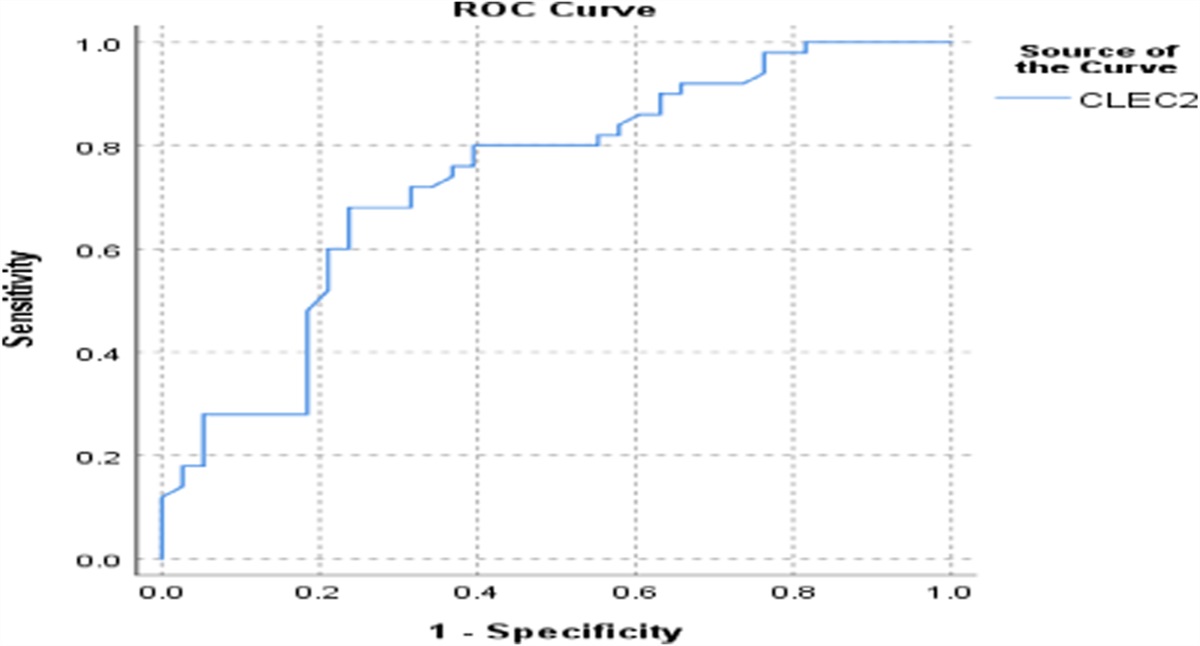
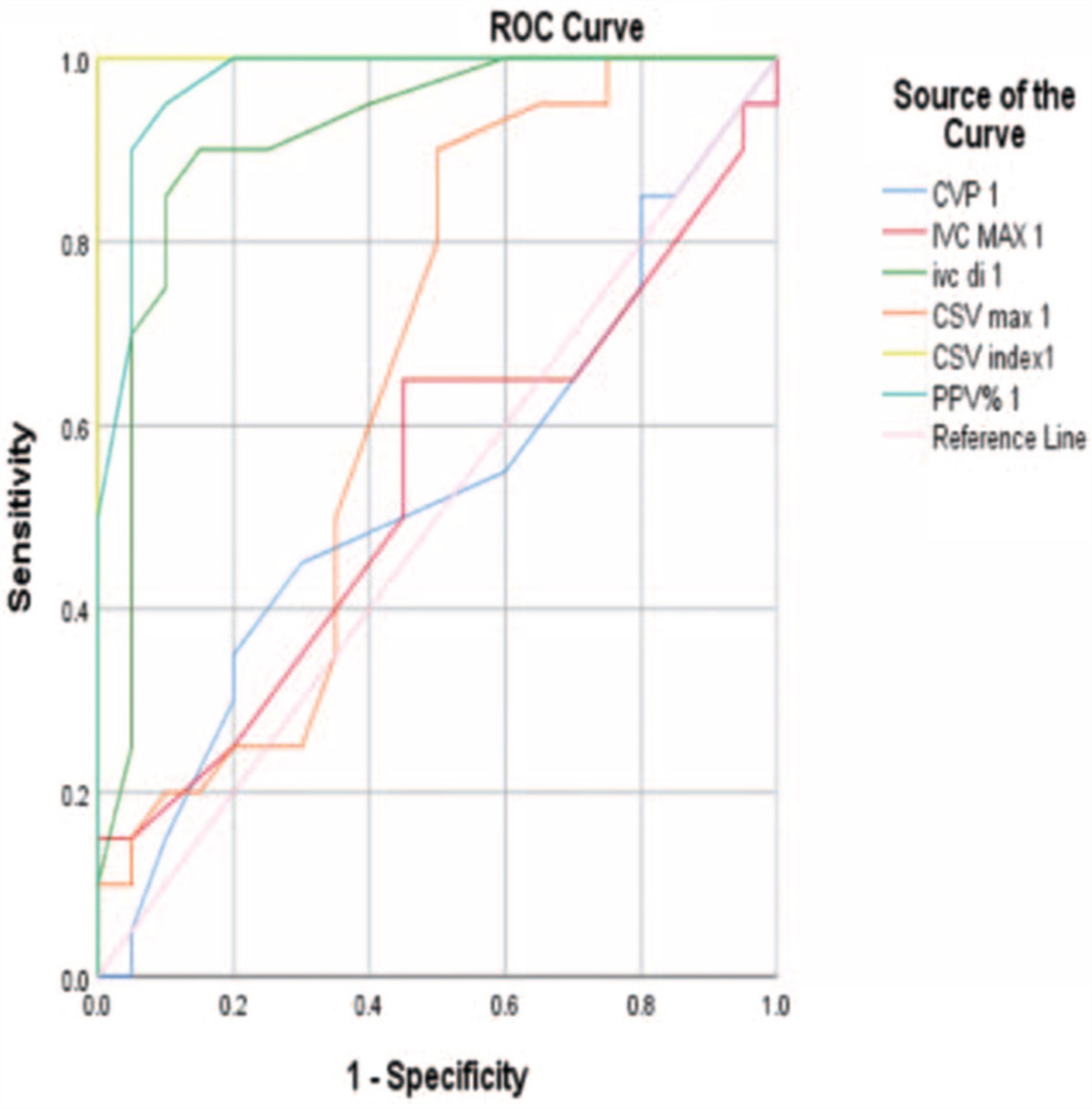
Risk stratification and prognostic performance of the PIRO, APACHE II, SOFA scores, and serum lactate (Figs. 1–3).
 Figure 1:
Figure 1: Receiver-operating characteristic (ROC) curve for APACHE II score, PIRO score, SOFA score, and serum lactate in discrimination of mortality in 1st day. APACHE, Acute Physiology and Chronic Health Evaluation; PIRO, predisposition, infection, response, and organ dysfunction; SOFA, Sequential Organ Failure Assessment.
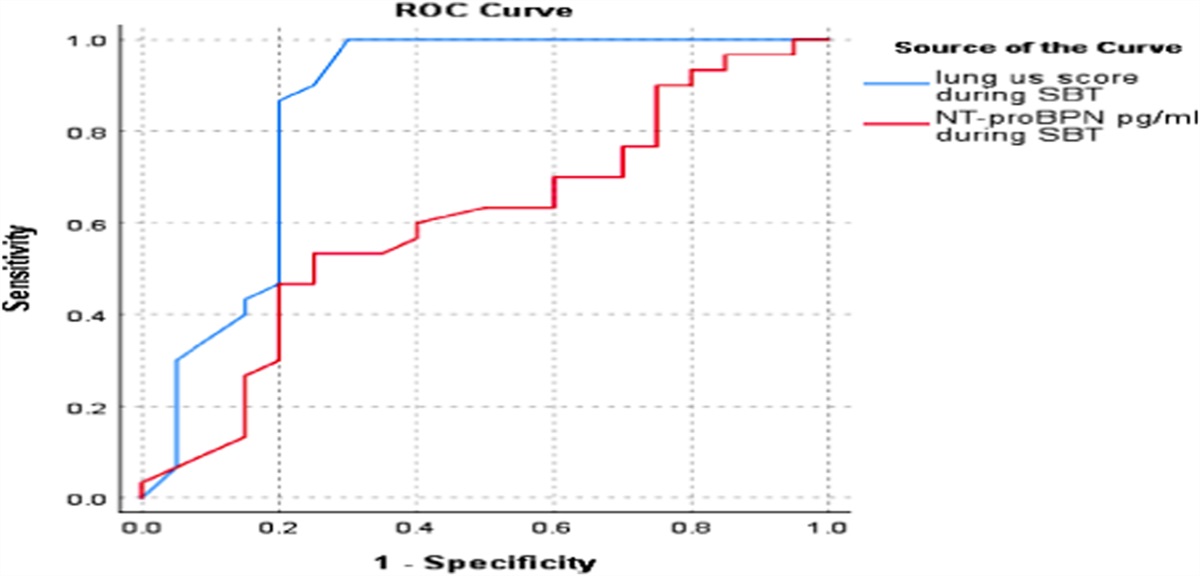
 Figure 2:
Figure 2: Receiver-operating characteristic (ROC) curve for APACHE II score, PIRO score, SOFA score, and serum lactate in discrimination of mortality in 2nd day. APACHE, Acute Physiology and Chronic Health Evaluation; PIRO, predisposition, infection, response, and organ dysfunction; SOFA, Sequential Organ Failure Assessment.
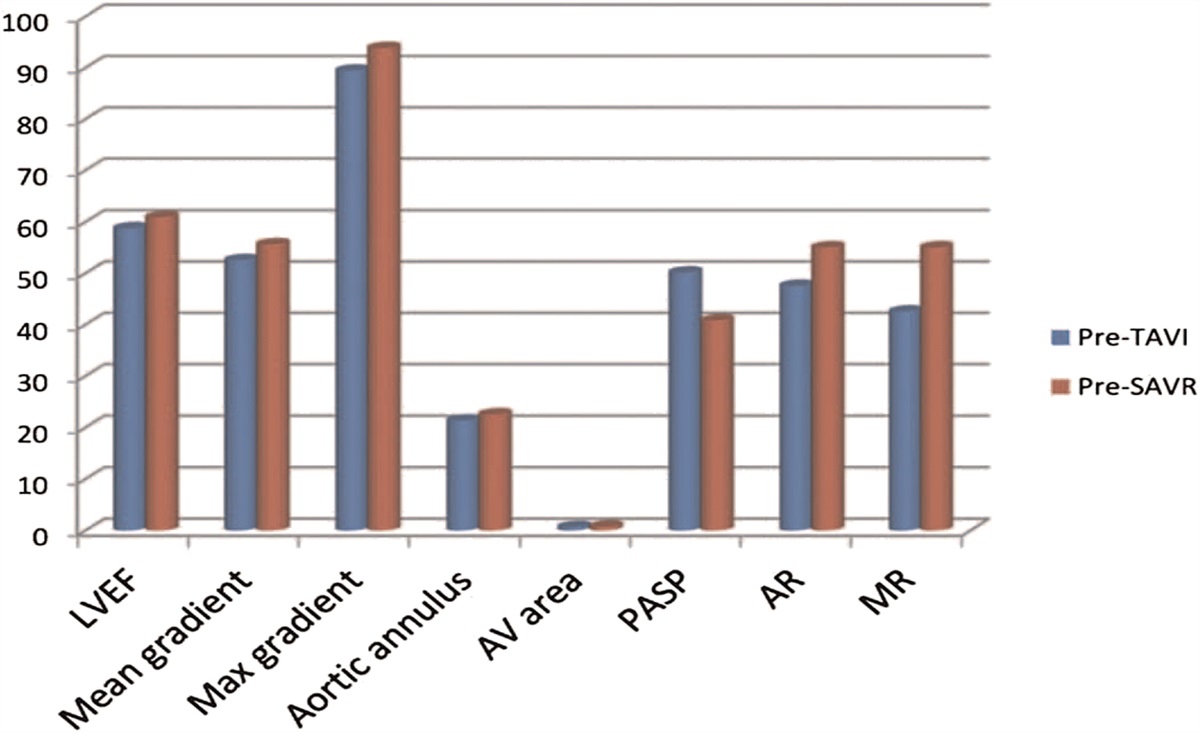
 Figure 3:
Figure 3: Receiver-operating characteristic (ROC) curve for APACHE II score, PIRO score, SOFA score, and serum lactate in discrimination of mortality in 3rd day. APACHE, Acute Physiology and Chronic Health Evaluation; PIRO, predisposition, infection, response, and organ dysfunction; SOFA, Sequential Organ Failure Assessment.
Mean PIRO score on admission was insignificantly lower in survivors (12.3 ± 4.5) compared to non-survivors (13.4 ± 3.7) (P value .279). Mean PIRO score in the 2nd day was significantly lower in survivors (11.2 ± 4.3) compared to non-survivors (13.0 ± 3.7) (P value .039). Mean PIRO score in the 3rd day was insignificantly lower in survivors (10.2 ± 3.6) compared to non-survivors (11.6 ± 4.6) (P value .236).
On admission to ICU, receiver operating characteristics curve was used to define the best cut-off value of APACHE II score that was >13, with sensitivity of 88.9%, specificity of 26%. Cut-off value of PIRO score was >10, with sensitivity of 81.5%, specificity of 43.5%. Cut-off value of SOFA score was >9, with sensitivity of 55.6%, specificity of 96%. Cut-off value of serum lactate was >22.1, with sensitivity of 77.8% specificity of 69.6%. SOFA score and serum lactate had a significant effect on mortality (P value .003 and .026, respectively), while APACHE II score and PIRO score did not have any significant mortality effect. In the 2nd day, cut-off value of APACHE II score was >21, with sensitivity of 37%, specificity of 91%. Cut-off value of PIRO score was >12, with sensitivity of 70.4% specificity of 65%. Cut-off value of SOFA score was >7, with sensitivity of 70.4%, specificity of 87%. Cut-off value of serum lactate was >23.1, with sensitivity of 81.5%, specificity of 69.6%. APACHE II score, PIRO score, SOFA score, and serum lactate had a significant effect on mortality (P value 0.038, 0.039, 0.002, 0.019, respectively). In the third day, cut-off value of APACHE II score was >19, with sensitivity of 32%, specificity of 95%. Cut-off value of PIRO score was >12, with sensitivity of 68% specificity of 73.9%. Cut-off value of SOFA score was >5, with sensitivity of 92% specificity of 69.6%. Cut-off value of serum lactate was >25.8, with sensitivity of 76%, specificity of 73.9%. APACHE II score, SOFA score, and serum lactate have a significant effect on mortality (P value .046, .003, and .030, respectively) while PIRO score had a non-significant effect.In our study, 75% of non-survivors showed increasing level of serum lactate, while 25% of non-survivors show decreasing level of serum lactate. Significant correlation was found between serum lactate level and mortality within 28 days (P value .04), organ dysfunction (P value .04), and days of ICU stay (P value .002) (Table 1).
Variable 0 1 2 3 4 Predisposition Age (yrs) <65 65–80 >80 COPD Yes Liver disease Yes Nursing home resident Yes Malignancy Without metastases With metastases Infection Skin/soft tissue infection Yes Any other infection Yes Pneumonia Yes Response Respiratory rate (bpm) >20 Bands >5% Heart rate (bpm) >120 Organ dysfunction SBP (mm Hg) >90 70–90 <70 BUN (mmol/L) >7.1 Respiratory failure/hypoxemia Yes Lactate (mmol/L) >4.0 Platelet count (×109/L) <150PIRO, predisposition, infection, response, and organ dysfunction.
Direct significant positive correlation was observed between PIRO score and APACHE II and SOFA scores in non-survivors (Fig. 4A and B).
 Figure 4:
Figure 4: (A) Correlation between PIRO score and APACHE II score in non-survivors. (B) Correlation between PIRO score and SOFA score in non-survivors. APACHE, Acute Physiology and Chronic Health Evaluation; PIRO, predisposition, infection, response, and organ dysfunction; SOFA, Sequential Organ Failure Assessment.
In the 1st day, mean arterial pressure, systolic blood pressure, hypoxemia, serum lactate, and total SOFA score were significant predictors of long ICU stay. Mean arterial pressure, systolic blood pressure, serum lactate, and total SOFA score in the 2nd day were significant predictors of long ICU stay. Serum lactate in the 3rd day was a significant predictor of long ICU stay.
5 Comparison of PIRO, APACHE II, SOFA scores, and serum lactate in survivors and non-survivorsAPACHE II score was significantly different between survivors and non-survivors in the 2nd day (14.4 ± 5.4 vs 18.7 ± 6.9) and 3rd day (12.4 ± 5.6 vs 15.3 ± 6.4) (P = .038 and P = .046, respectively). PIRO score was significantly lower in survivors in 2nd day (11.2 ± 4.3 vs 13.0 ± 3.7) (P value .039). SOFA score was significantly lower in survivors on admission, 2nd day, and 3rd day (5.8 ± 2.5 vs 9.8 ± 3.5), (5.1 ± 2.4 vs 9.3 ± 3.6), and (4.5 ± 2.0 vs 8.3 ± 4.1), respectively (P value .002, <.002, and <.003, respectively). So SOFA score had more significant correlation than APACHE II and PIRO scores.
In the current study we found that mean serum lactate on admission, on 2nd day, 3rd day were significantly lower in survivors compared to in non-survivors, respectively (22.2 ± 8.9) (33.2 ± 15.3) (P value .004), (21.1 ± 8.3) (33.9 ± 12.8) (P value .0002), and (21.7 ± 7.8) (33.7 ± 15.1) (P value .0002).
6 Comparison of PIRO, APACHE II, SOFA scores, and serum lactate in medical, surgical, and mixed medical surgical cases of sepsisNeither APACHE II nor PIRO score showed significant changes between survivors and non-survivors regarding the cause of sepsis whether medical or surgical or mixed medical surgical cases of sepsis; however, SOFA score was significantly higher in non-survivors in the medical (P value .009) and surgical cases (P value .02). Neither APACHE II nor PIRO score showed significant changes between survivors and non-survivors regarding the source of infection. However, SOFA score was significantly higher in non-survivors in those presented with chest infection (P value .009), urinary tract infection (P value .04), and post-operative infected wound (P value .05).
7 DiscussionIn the present study, 30 patients were admitted to the Critical Care unit Egyptian Railway Medical hospital and 20 patients were admitted to the Critical Care unit El Helal Hospitals with new diagnosis of sepsis during the period from July 2015 to October 2016. They included 41males (82%) and 9 females (18%) with mean age of 67.02 ± 13.13 years.
Twenty-four percent of patient had no comorbidity, while 76% of patients had at least 1 comorbidity in addition to sepsis. Regarding relationship of comorbidities and outcome, we found that gender and all types of associated comorbidities, like hypertension, diabetes mellitus, COPD, chronic kidney disease, chronic liver disease, or malignancies, did not have any statistical significant effect on the outcome of the studied group.
In concordance to our study, Gunes Ozaydin et al. demonstrated no significant difference in the mean age between the survivors and non-survivors.7 Chen and Li demonstrated that gender did not have an effect on the outcome of the studied group.8 In the current study we found that GCS (P = .008), systolic blood pressure (P = .0007), mean arterial pressure (P = .0004), and hematocrit value (P = .02) were significantly lower in the non-survivors compared to survivors and that respiratory rate (P = .02), BUN (P = .0002), bands (P = .02), and serum creatinine (P = .0001) were significantly higher in the non-survivors compared to survivors.
In concordance to our study, Houwink et al. observed that admission MAP and admission lactate were associated with mortality, 24-hour mean lactate, and 24-hour mean MAP are associated with ICU and hospital mortality and 24-hour mean lactate was the strongest predictor for ICU and hospital mortality.9 Juncal et al. observed that hematocrite level was the only variable that was a predictor of mortality risk in the patients diagnosed with sepsis.10
Tridente et al. documented thrombocytopenia, renal dysfunction, and total SOFA score were independently associated with poor outcomes over the first 3 days in the ICU. Higher SOFA score, lower GCS, low mean arterial pressure, and low ratio of partial pressure of arterial oxygen to fraction of inspired oxygen were independently associated with 28-day mortality.11
We found that the survivors had mean length of stay (14.9 ± 7.5) days shorter than the non-survivors, (20.1 ± 7.3) days (P value .01) yet according to Williams et al., ICU stay was not an independent risk factor for short-term mortality, but it had a small effect on long-term mortality after hospital discharge and after adjustment of other risk factors.12 Jain et al. demonstrated the duration of ICU stay did not correlate with the survival.13
The outcome of the studied patients was evaluated after ICU discharge. Twenty-eight patients (56%) did not survive, while 22 patients (44%) survived and were discharged. Three patients (6%) were readmitted to the ICU within 28 days.
The current study included 50 septic patients, 35 patients had been diagnosed as septic shock. The remaining 15 patients had organ dysfunction (13 survivors and 2 non-survivors). Fifteen patients (53%) of the non-survivor group (28 patients) need mechanical ventilation compared to only 8 patients (36%) from the survivor group (22 patients). Two patients (7%) of non-survivor group (28 patients) need dialysis in first 3 days compared to no patients (0%) from the survivor group (22 patients). Eighteen patients out of the non-survivors received inotropic support compared to only 3 patients out of the survivor group. According to Belletti et al., inotropic/vasopressor therapy was not associated with differences in mortality in the overall population.14
In concordance to our study, Sinkovic et al. documented that 30-day mortality of patients with severe sepsis and septic shock was 62.7%.15
In our prediction model for mortality, which was based on best predictors in comparison between survivors and non-survivors. The best predictors were Sofa score on admission, 2nd day, and 3rd days. Mean serum lactate on 1st day, 2nd day, and 3rd day. APACHE II score in 2nd day and 3rd day, PIRO score in 2nd day.
Chen and Li demonstrated that the PIRO system was an independent predictor of 28-mortality in concordance to their conclusion, we found in the present study that both PIRO and APACHE II scores independently predicted 28-day mortality.8 Jain et al. demonstrated that SOFA score is a simple, but effective prognostic indicator and evaluator for patient progress in ICU. Day 1 SOFA can triage the patients into risk categories. For further management, mean and maximum scores help determine the severity of illness and can act as a guide for the intensity of therapy required for each patient. Total SOFA scores of days 1, 3, and 5 correlated significantly with survival.13 Jones et al. demonstrated that the SOFA score demonstrated fair to good accuracy for predicting in-hospital mortality when applied to patients with severe sepsis with evidence of hypoperfusion at the time of ED presentation. The ΔSOFA over 72 hours has a significant positive relationship to in-hospital mortality.16 Khan et al. concluded that APACHE II, SAPS II, and SOFA scores were better when calculated at 48 hours rather than at 24 hours. A worsening APACHE II score at 48 hours after ICU admission may identify those patients at high risk of mortality.17
Macdonald et al. demonstrated that the predisposition, insult/infection, response, and organ dysfunction model performed better than the Sequential Organ Failure Assessment and Mortality in Emergency Department Sepsis scores for predicting mortality in ED patients with severe sepsis and septic shock.18
Houwink et al. demonstrated that admission MAP and lactate independently predicted ICU and hospital mortality. The 24-hour mean lactate, mean MAP independently predicted hospital mortality 24-hour mean lactate, 95% confidence interval.9
In contrast to our results, Chen and Li demonstrated that prognostic value of PIRO system was similar to that of APACHE II score.8 Khan et al. demonstrated that APACHE II scoring system to be the best for the prediction of outcome in ICU better than SOFA and SAPS II.17
Chen and Li demonstrated that the average APACHE II and PIRO scores were independent predictors of 28-day mortality and had similar AUC and mean diagnostic accuracy of 74.4%.8 Macdonald et al. demonstrated that the PIRO model performed better than the SOFA score for predicting mortality in ED patients with severe sepsis and septic shock.18
Jones et al. demonstrated that the area under the receiver operating characteristic curve of SOFA for predicting in-hospital mortality at T0 was 0.75 (95% confidence interval 0.68–0.83) and at T72 was 0.84 (95% confidence interval 0.77–0.90). The SOFA score demonstrated fair to good accuracy for predicting in-hospital mortality to patients with severe sepsis with evidence of hypoperfusion at the time of ED presentation. The ΔSOFA over 72 hours has a significant positive relationship to in-hospital mortality.16
We found that neither APACHE II score nor SOFA score was significantly different between medical, surgical, and mixed medical surgical cases in first 3 days. On the 1st day, PIRO score was significantly different between medical versus surgical cases (P value < .01) and between surgical versus mixed medical surgical cases (P value < .05). On the 2nd day, PIRO score was significantly different between medical versus surgical cases (P value < .01). Similarly, some authors concluded that, PIRO score performed well as an ICU mortality predictor tool for surgical related intra-abdominal sepsis.19 Tang et al. documented that there was no significant difference in sepsis prevalence, severe sepsis prevalence, and the 28-day death rate among the 3 groups (internal medicine, surgery, and trauma).20
8 Limitations of the studyWe tried to match the recruitment time to the time of the onset of sepsis. However this was nearly an impossible task mainly due to delays in the presentation to the ICU, ICU bed availability, referral patterns, and the presentation of symptoms. Also results need to be validated on a larger study population.
9 ConclusionsAPACHE II, PIRO, and SOFA scores were valuable in predicting 28-day mortality in septic patients. Comparing survivors and non-survivors, SOFA score was significantly lower on admission, 2nd day, and 3rd day; APACHE II score was significantly lower in 2nd day and 3rd day; PIRO score was significantly lower in 2nd day. Serum lactate can predict short-term outcome in septic patient and a significant correlation was found between lactate level and mortality within 28 days, organ dysfunction, and days of ICU stay. Direct significant relationship between PIRO score (in non-survivors and patients with organ dysfunction) and APACHE II score and SOFA scores was found.
References [1]. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016;315(8):801–810. [2]. Grolimund E, Kutz A, Marlowe RJ, et al. Long term prognosis in COPD exacerbation: role of biomarkers, clinical variables and exacerbation type. COPD 2014;12:295–305. [3]. Moreno RP, Metnitz B, Adler L, Hoechtl A, Bauer P, Metnitz PG. Sepsis mortality prediction based on predisposition, infection and response. Intensive Care Med 2008;34:496–504. [4]. Khwannimit B, Bhurayanontachai R. Validity of six prognostic scoring systems for septic shock patients admitted to a medical ICU. Crit Care 2012;16(Suppl 1):416. [5]. Vincent JL, de Mendonca A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working Group On (Sepsis-Related Problems) Of The European Society Of Intensive Care Medicine. Crit Care Med 1998;26(11):1793–1800. [6]. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med 2013;39(2):165–228. [7]. Gunes Ozaydin M, Guneysel O, Saridogan F, Ozaydin V. Are scoring systems sufficient for predicting mortality due to sepsis in the emergency department? Turk J Emerg Med 2016;17(1):25–28. [8]. Chen YX, Li CS. Prognostic value of adrenomedullin in septic patients in the ED. Am J Emerg Med 2013;31:1017–1021. [9]. Houwink API, Rijkenberg S, Bosman RJ, van Der Voort PHJ. The association between lactate, mean arterial pressure, central venous oxygen saturation and peripheral temperature and mortality in severe sepsis: a retrospective cohort analysis. Crit Care 2016;20:56. [10]. Juncal VR, Britto Neto LA, Camelier AA, Coelho Messeder OH, de Carvalho Farias AM. Clinical impact of sepsis at admission to the ICU of a private hospital in Salvador. Brazil J Bras Pneumol 2011;37(1):85–92. [11]. Tridente A, Clarke GM, Walden A, et al. Gen O Sept Investigators. Association between trends in clinical variables and outcome in intensive care patients with faecal peritonitis: analysis of the GenOSept cohort. Crit Care 2015;19(8):210. [12]. Williams M, McPherson D, Griffiths C, Baker A. Sepsis-associated mortality in England: an analysis of multiple cause of death data from 2001 to 2010. BMJ Open 2013;3(8):86. [13]. Jain A, Palta S, Saroa R, Palta A, Sama S, Gombar S. Sequential organ failure assessment scoring and prediction of patient's outcome in Intensive Care Unit of a tertiary care hospital. J Anaesthesiol Clin Pharmacol 2016;32(3):364–368. [14]. Belletti A, Castro ML, Silvetti S, et al. The effect of inotropes and vasopressors on mortality: a meta-analysis of randomized clinical trials. Br J Anaesth 2015;115(5):656–675. [15]. Sinkovic A, Markota A, Fluher J, Rehar D. Predictors of 30-day mortality in medical patients with severe sepsis or septic shock. Signa Vitae: journal of intensive care and emergency medicine 2014;9(2):47–52. [16]. Jones AE, Trzeciak S, Kline JA. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Crit Care Med 2009;37(5):1649–1654. [17]. Khan MS, Maitree P, Radhika A. Evaluation and comparison of the three scoring systems at 24 and 48 h of admission for prediction of mortality in an Indian ICU: a prospective cohort study. Ain Shams J Anesthesiol 2015;8(3):294–300. [18]. Macdonald SPJ, Williams JM, Shetty A, et al. Review article: sepsis in the emergency department – Part 1: definitions and outcomes. Emerg Med Australas 2017;29:619–625. [19]. Bratzler DW, Dellinger EP, Olsen KM, et al. An analysis of a cohort of surgical-related intra-abdominal sepsis with PIRO. Surg Infect 2020;14(1):73. [20]. Tang H, Liu D, Zhang H-Y, et al. Epidemiology of sepsis in ICUs of Western China. J Acute Dis 2016;5(3):210–215.
Comments (0)