
Remember me
Several groups of inflammatory markers have been identified including cytokines/chemokines, acute phase proteins [C-reactive protein (CRP) and serum amyloid A], reactive oxygen and nitrogen species, prostaglandins and cyclo-oxygenase related factors, and mediators such as transcription factors and growth factors.1–3
During the immediate postoperative phase, biological markers such as CRP, albumin, and blood lactate levels correlate with the degree of inflammation and may be used as independent predictors for the prognosis.4–7 However, the use of infection markers can show test results that are apparently normal in sepsis, especially in patients with deprimed immune response.
The prognostic indices can be used to analyze a cohort or group of specific diseases, and can guide health strategies. Between them, acute physiology and chronic health evaluation (APACHE) and sequential organ failure assessment (SOFA) scores have been commonly used to predict the outcome of critically ill surgical patients. Owing to the use of several physiological variables from various organic systems, these scores are more comprehensive.8,9
In addition, the use of prognostic indices can be used not only to predict which patients are likely to develop sepsis, but also to predict which patient may or may not survive sepsis. Prompt identification of patients at risk of developing sepsis allows for an informed approach to ICU admission, which can enhance outcomes.
Researchers have therefore been looking for a primary prognosticator for critically ill surgical patients for decades.10 However, none of these indices have a sensitivity of 100 percent or a precision of 100 percent.
2 Aim of workTo study the prognostic value of CRP/albumin ratio, as a marker of infection, in postoperative abdominal septic patients admitted to the ICU in the immediate postoperative phase and its correlation with SOFA score.
3 Patient and methodsThis prospective observational study was conducted in a general adult ICU of critical care department, Cairo University Hospitals, Egypt. The study protocol was approved by the local Research Ethics Committee.
The study included 80 adult surgical patients (age > 18 years old) admitted to ICU during the immediate postoperative phase after major abdominal surgeries between 2018 and 2019. These patients were included due to high probability of developing abdominal sepsis.
We excluded patients under 19 years and patients with chronic hepatitis, liver cirrhosis, and chronic kidney disease due to a possible effect on albumin levels.
Data concerning the diagnosis upon ICU arrival, comorbidities, and demographic profile were documented. Biological markers: CRP (immunoluminometric assay, reference range = 0–10 mg/L), albumin (colorimetric assay, reference range = 3.5–5.5 g/dL), and SOFA score were recorded every 48 hours. CRP/albumin ratio was mathematically measured by dividing the CRP level (mg/L) by the serum albumin level (g/L).11
The diagnosis of sepsis was defined as life-threatening organ dysfunction caused by a dysregulated host response to infection and managed according to sepsis-3 guidelines.12–14
Follow-up of patients for 7 days, 28 days, and 3 months included: surgical complications, need for hemodynamic support or mechanical ventilation, ICU stay, ICU survival, in-hospital mortality, and 3-months survival (Table 1).
Table 1 - Demographic and clinical data of the studied population Number 80 (100%) Gender Male 57 (71.3%) Female 23 (28.7%) Age (y) 43.7 ± 17.4 Comorbidities HTN 10 (12.5%) DM 5 (6.25%) IHD 13 (16.25%) Types of operations Oesophago-gastrectomy 29 (36.25%) Repair of intestinal obstruction 26 (32.5%) Pancreatico-dudenectomy 25 (31.25%) APACHE II score 12 ± 5.6 SOFA score Day 1 3.3 ± 2.7 Day 3 2.9 ± 1.8 Day 5 3.0 ± 1.9 Day 7 3.1 ± 2.2APACHE, acute physiology and chronic health evaluation; SOFA, sequential organ failure assessment.
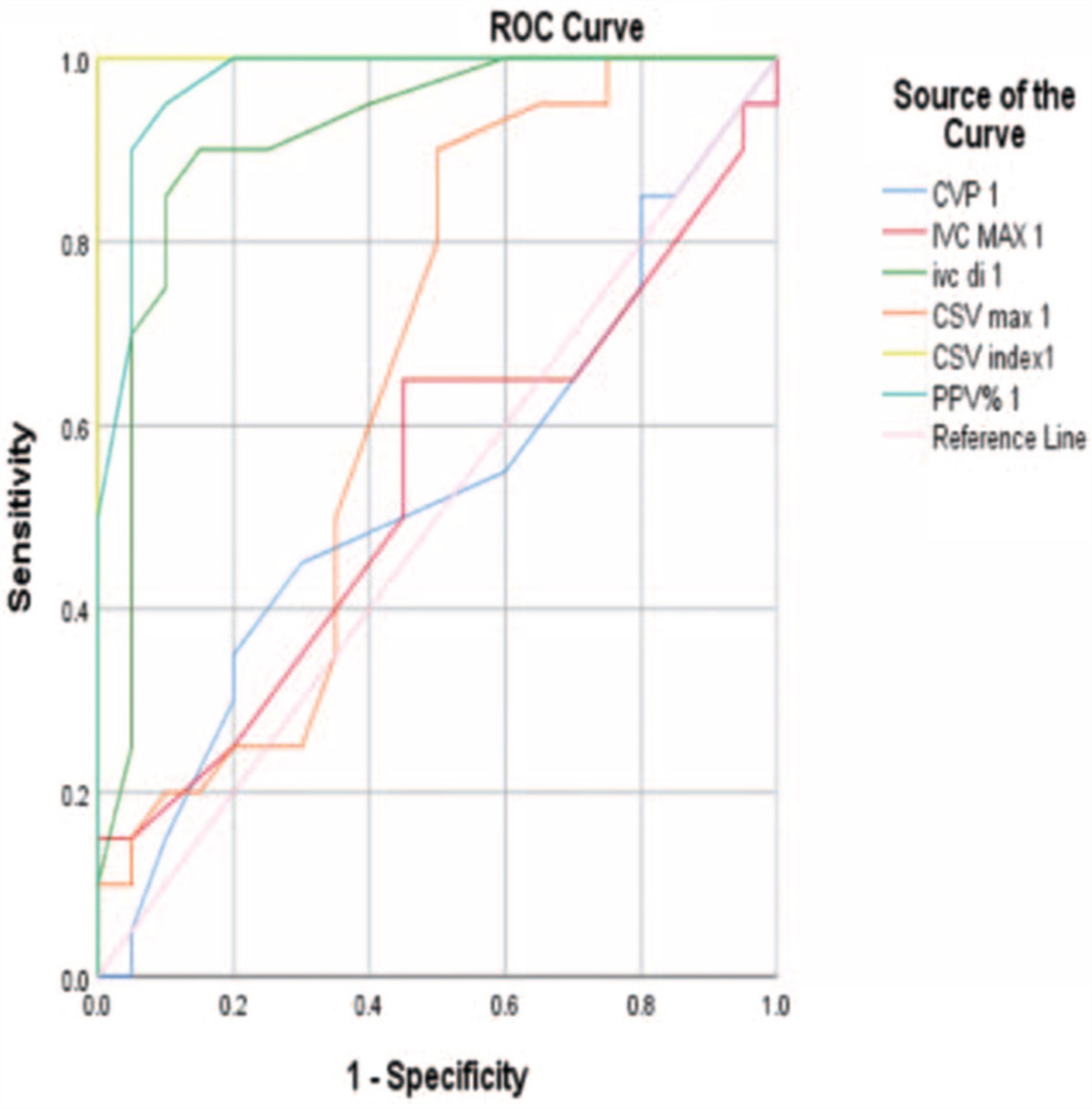
Demographic and clinical data of the studied population showed 80 patients, males = 57 (71.3%), mean age 43.7 ± 17.4 years, oesophago-gastrectomy 29 (36.25%), repair of intestinal obstruction 26 (32.5%), pancreatico-dudenectomy 25 (31.25%) as shown in Figure 1.
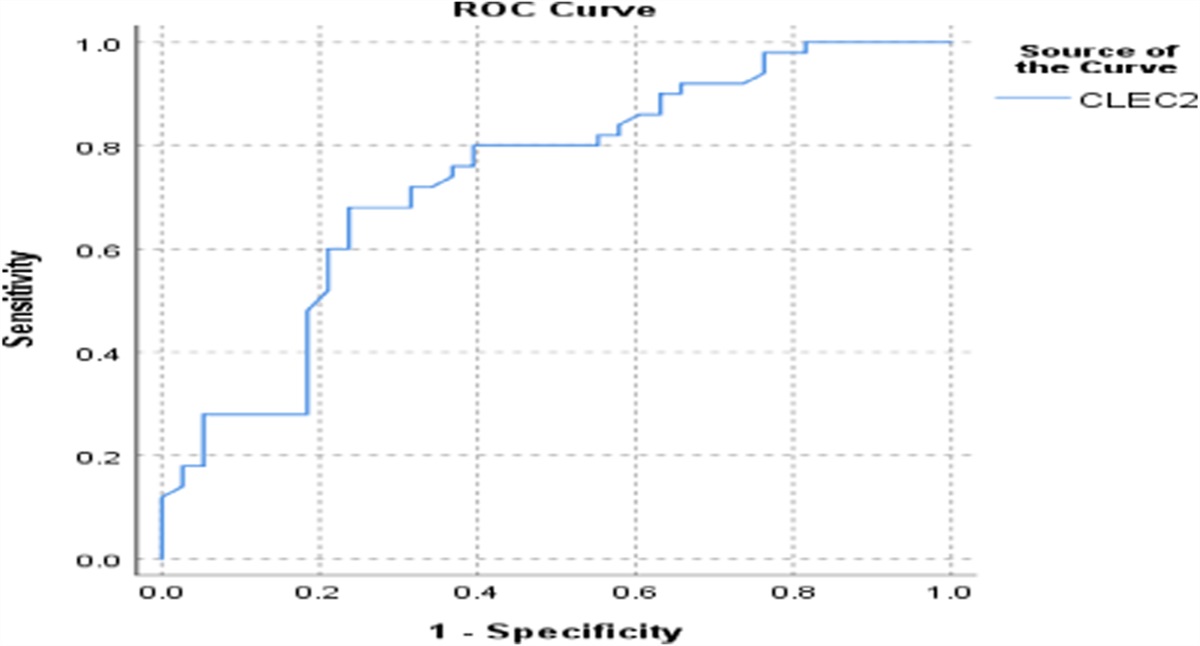
 Figure 1:
Figure 1: ROC curve analysis for the whole group day 1 and day 3 after surgery.
Laboratory data are shown in Table 2.
Table 2 - Laboratory data of the study population Day 1 Day 3 Day 5 Day 7 Serum albumin (g/dL) 2.4 ± 0.46 2.6 ± 0.55 2.57 ± 0.48 2.39 ± 0.28 CRP level (mg/L) 78.9 ± 20.7 59.7 ± 26.2 54.9 ± 22.9 53.3 ± 16.6 WBC count (×103) 15.8 ± 9.0 14.1 ± 6.8 12.9 ± 5.1 9.7 ± 4.2 CRP/albumin ratio 0.34 ± 11.1 0.24 ± 13.7 0.22 ± 11.8 0.22 ± 9.4To inspect the predictive value of CRP/albumin ratio for early postoperative infection, ROC curve analysis showed that:
The AUC of CRP/albumin ratio at POD1 for the study group was 0.662, sensitivity was 65.4%, specificity was 55.6%, positive predictive value was 41.5%, negative predictive value was 76.9%, and the cut-off point was 0.319.
The AUC of CRP/albumin ratio at POD3 for the study group was 0.452, sensitivity was 70.2%, specificity was 88.2%, positive predictive value was 86.4%, negative predictive value was 82.6%, and the cut-off point was 0.23.
Patients with values more than 0.23 had more infection rate (P = 0.05), WBC count (P = 0.01), and ICU stay (P = 0.047).
In the multivariate analysis, adjusted for age, sex, underlying disease, and APACHE II score, CRP/albumin ratio (OR = 1.02, 95% CI = 1.01–1.03, P = 0.01) was an independent predictor of 28-day mortality.
4.1.1 Correlation between CRP/albumin ratio and SOFA scoreThere was a positive significant correlation between CRP/albumin ratio and SOFA score at first, third, and fifth postoperative days with (r = 0.573, P = 0.023), (r = 0.728, P > 0.001), and (r = 0.351, P = 0.001), respectively.
4.1.2 Follow-up data of patients for 7 days, 28 days, and 3 monthsSurgical complications included wound infection 13 (16.25%), wound leakage 13 (16.25%), and paralytic ileus 1 (1.25%). Mean ICU stay 5.16 ± 2.56 days, ICU survival = 67 (83.8%), in-hospital mortality = 13 (16.25%) as in Table 3.
Surgical complications Wound infection 13 (16.25%) Wound leakage 13 (16.25%) Paralytic ileus 1 (1.25%) Clinical data Need for MV 35 (43.75%) Need for inotropes 16 (20%) ICU outcome ICU stay (d) 5.16 ± 2.56 ICU survival 67 (83.8%) 28 d mortality 13 (16.25%) 90 d survival 53 (66.25%)Biological markers (CRP, albumin, and lactate) may play a significant role as independent predictors of mortality in critically ill patients. CRP is the most commonly available vector for detecting postoperative inflammation following major abdominal surgery and the most commonly used biomarker of infection in ICU patients.17
The CRP level is known to increase in response to initial surgical stress due to tissue damage, to reach a peak in the postoperative period of 48 to 72 hours, and to decrease shortly thereafter.18,19 In addition, CRP appears to normalize in patients without postoperative complications due to a half-life of 19 hours.
However, its rates can remain high if complications persist. Several research studies have attempted to reach the CRP cut-off point for postoperative complications or sepsis.20–22
Meyer et al.23 stated that an increase in CRP is a poor parameter for early detection of complications in critically ill surgical patients (odds ratio = 0.983, 95% CI = 0.932–1.036). The authors had found that CRP is not a satisfactory predictor of survival in the ICU during the early course of admission and there is no significant relationship between increased levels and surgical complications.
Serum albumin is a negative acute phase reactant that is rapidly down-regulated by inflammatory signals.5,24 After major surgery, postoperative serum albumin decreases can be used as a marker of surgical stress response and early predictor in the clinical outcome.25
Labgaa et al.26 demonstrated in a cohort of 138 patients after major abdominal surgery that a serum albumin drop greater than 2 g/L in the first postoperative days has an adverse outcome with [odds ratio: 6.89, 95% CI = 2.96–16.14].
The use of a ratio between CRP and albumin would provide a vector capable of combining the CRP and albumin information into an index that positively correlated with infection.27
The CRP to albumin ratio is used as a prognostic score for determining outcomes in cancer, inflammation, and sepsis patients. More recently, this ratio was used to predict postoperative abdominal surgical complications.28
In our study, the AUC of CRP/albumin ratio at POD1 for the study group was 0.662, sensitivity was 65.4%, specificity was 55.6%, positive predictive value was 41.5%, negative predictive value was 76.9%, and the cut-off point was 0.319.
The AUC of CRP/albumin ratio at POD3 for the study group was 0.452, sensitivity was 70.2%, specificity was 88.2%, positive predictive value was 86.4%, negative predictive value was 82.6%, and the cut-off point was 0.23.
Patients with values more than 0.23 had more infection rate (P = 0.05), WBC count (P = 0.01), and ICU stay (P = 0.047).
This is in agreement with Karayiannis et al. who evaluated the prognostic value of CRP/albumin in day 3 in 214 patients submitted to abdominal surgeries and showed that 33.6% of these patients had postoperative complications and patients with a CRP/albumin ratio > 2.0 suffered more (49.3% vs 22.1%, P < 0.05). Thus, the surgical site infections were 21.1 versus 4.85% of the patients (P < 0.001). It was concluded that the bigger the CRP/albumin ratio, the higher is the probability of postoperative complications.28
Also, Ge et al. found that AUC of CRP/albumin ratio in patients with postoperative removal of colorectal cancer was 0.764, with a sensitivity of 69.1%, and a specificity of 72.8%. The cut-off value was (2.3). Patients with CRP/albumin ratio ≥ 2.2 were found to have more postoperative infections than those with CRP/albumin ratio < 2.2 (60.8% vs 18.6%, P < 0.001). Moreover, patients with CRP/albumin ratio ≥ 2.2 were more likely to have a longer postoperative stay and surgical site infection (P < 0.001).30
Our study showed that patients with values more than 0.23 had higher sensitivity to predict 28- and 90-day mortality.
This is consistent with Ranzani et al.29 who examined CRP/albumin's ability to predict 90-day mortality in 334 patients. These authors found that the CRP/albumin ratio > 2 in patients with sepsis/septic shock provided the highest sensitivity and responsiveness in predicting 90-days mortality.
Also, Park et al.4 showed that APACHE II score, history of cancer, and CRP/albumin ratio were independent predictors of 28-day mortality.
In our study, there was a positive significant correlation between CRP/albumin ratio and SOFA score (P > 0.001). Interestingly, this correlation was not studied before and need further scientific research.
6 ConclusionWe support the evidence that C-reactive protein/albumin ratio is a significant predictor of early postoperative infection in postoperative abdominal surgeries.
There was a positive significant correlation between CRP/albumin ratio and SOFA score.
References [1]. Basile-Filho A, Menegueti MG, Auxiliadora-Martins M, et al. Why the surgical patients are so critical in their intensive care unit arrival. Acta Cir Bras 2013;28(Suppl 1):48–53. [2]. De la Plaza Llamas R, Ramia JM. Cost of postoperative complications: how to avoid calculation errors. World J Gastroenterol 2020;26(21):2682–2690. [3]. Brenner DR, Scherer D, Muir K, et al. A review of the application of inflammatory biomarkers in epidemiologic cancer research. Cancer Epidemiol Biomarkers Prev 2014;23:1729–1751. [4]. Park JE, Chung KS, Song JH, et al. The C-reactive protein/albumin ratio as a predictor of mortality in critically ill patients. J Clin Med 2018;7:333. DOI 10.3390/jcm7100333. [5]. Hübner M, Mantziari S, Demartines N, et al. Postoperative albumin drop is a marker for surgical stress and a predictor for clinical outcome: a pilot study. Gastroenterol Res Pract 2016;2016:8743187. [6]. Torres A, Artigas A, Ferrer R. Biomarkers in the ICU: less is more? No. Intensive Care Med 2021;47:97–100. [7]. Li S, Peng K, Liu F, et al. Changes in blood lactate levels after major elective abdominal surgery and the association with outcomes: a prospective observational study. J Surg Res 2013;184:1059–1069. [8]. Akavipat P, Thinkhamrop J, Thinkhamrop B, et al. Acute physiology and chronic health evaluation (APACHE) II score. The clinical predictor in neurosurgical intensive care unit. Acta Clin Croat 2019;58(1):50–56. [9]. Li Y, Yan C, Gan Z, et al. Prognostic values of SOFA score, qSOFA score, and LODS score for patients with sepsis. Ann Palliat Med 2020;9(3). DOI 10.21037/apm-20-984. [10]. Meyer ZC, Schreinemakers JM, de Waal RA, et al. Searching for predictors of surgical complications in critically ill surgery patients in the intensive care unit: a review. Surg Today 2015;45:1091–1101. [11]. Sun P, Chen C, Xia Y, et al. The ratio of C-reactive protein/albumin is a novel inflammatory predictor of overall survival in cisplatin-based treated patients with metastatic nasopharyngeal carcinoma. Dis Markers 2017;2017:6570808. DOI 10.1155/2017/6570808. Article ID 6570808, 9 pages. [12]. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016;315:801–810. [13]. Shankar-Hari M, Phillips GS, Levy ML, et al. Sepsis definitions task force: developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016;315:775–787. [14]. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 2016;315:762–774. [15]. Zhang Z. Model building strategy for logistic regression: purposeful selection. Ann Transl Med 2016;4:111–118. [CrossRef] [PubMed]. [16]. Zhang Z. Residuals and regression diagnostics: focusing on logistic regression. Ann Transl Med 2016;4:195–203. [CrossRef] [PubMed]. [17]. Lelubre C, Anselin S, Zouaoui Boudjeltia K, et al. Interpretation of C-reactive protein concentrations in critically ill patients. BioMed Res Int 2013;2013:124021. DOI 10.1155/2013/124021. Article ID 124021, 11 pages. [18]. González-Martínez S, Olona Tabueña N, Martín Baranera M, et al. Inflammatory markers as predictors of postoperative adverse outcome in octogenarian surgical patients: an observational prospective study. Cir Esp 2015;93(3):166–173. [19]. Ticinesi A, Lauretani F, Nouvenne A, et al. C-reactive protein (CRP) measurement in geriatric patients hospitalized for acute infection. Eur J Intern Med 2017;37:7–12. [20]. Welsch T, Frommhold K, Hinz U, et al. Persisting elevation of C-reactive protein after pancreatic resections can indicate developing inflammatory complications. Surgery 2008;143:20–28. [21]. Ranzani OT, Zampieri FG, Forte DN, et al. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One 2013;8:e59321. [22]. Kim MH, Ahn JY, Song JE, et al. The C-reactive protein/albumin ratio as an independent predictor of mortality in patients with severe sepsis or septic shock treated with early goal-directed therapy. PLoS One 2015;10:e0132109. [23]. Meyer ZC, Schreinemakers JM, Mulder PG, et al. The role of C-reactive protein and the SOFA score as parameter for clinical decision making in surgical patients during the intensive care unit course. PLoS One 2013;8:e55964. [24]. Sang BH, Bang JY, Song JG, et al. Hypoalbuminemia within two postoperative days is an independent risk factor for acute kidney injury following living donor liver transplantation: a propensity score analysis of 998 consecutive patients. Crit Care Med 2015;43:2552–2561. [25]. Soeters PB, Wolfe RR, Shenkin A. Hypoalbuminemia: pathogenesis and clinical significance. J Parenter Enteral Nutr 2019;43(2):181–193. [26]. Labgaa I, Joliat GR, Kefleyesus A, et al. Is postoperative decrease of serum albumin an early predictor of complications after major abdominal surgery? A prospective cohort study in a European centre. BMJ Open 2017;7:e013966. [27]. Fairclough E, Cairns E, Hamilton J, et al. Evaluation of a modified early warning system for acute medical admissions and comparison with C-reactive protein/albumin ratio as a predictor of patient outcome. Clin Med 2009;9:30–33. [28]. Karayiannis D, Bouloubasi Z, Baschali A, et al. Postoperative C-reactive protein to albumin ratio as a diagnostic tool for predicting complications after abdominal surgery. Clin Nutr ESPEN 2018;24:176. [29]. Ranzani OT, Zampieri FG, Forte DN, Azevedo LC, Park M. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One 2013;8(3):e59321. DOI 10.1371/journal.pone.0059321. [30]. Ge X, Cao Y, Wang H, et al. Diagnostic accuracy of the postoperative ratio of C-reactive protein to albumin for complications after colorectal surgery. World J Surg Oncol 2017;15:15. DOI 10.1186/s12957-016-1092-1.
Comments (0)