
Remember me
Cardiovascular disease and myocardial infarction are the largest cause of death worldwide. According to WHO records, 17.3 million deaths in 2008 were attributable to cardiovascular disease, with 7.3 million (42% of all cardiovascular deaths) being due to myocardial infarction. In 2009, approximately one sixth of people in the United States died of coronary heart disease.1
The preferred reperfusion strategy in patients with acute ST elevation myocardial infarction (STEMI) is primary percutaneous coronary intervention (PCI). Randomized clinical trials comparing timely primary PCI with in-hospital fibrinolytic therapy in high-volume, experienced centers have repeatedly shown that primary PCI was superior to hospital fibrinolysis with more effective restoration of patency, less reocclusion, improved residual left ventricular (LV) function, and better clinical outcome with primary PCI.2,3
Iodinated contrast media (CM) are utilized in an estimated 80 million diagnostic and interventional cardiovascular and non- cardiovascular procedures worldwide, annually. This growth in diagnostic and interventional cardiac angiography has posed contrast-induced acute kidney injury (CI-AKI) as a major health concern associated with administration of iodinated CM in these procedures.4
The reported incidence of CI-AKI varies widely across the literature, depending on the patient population and the baseline risk factors. The frequency of CI-AKI has decreased over the past decade from a general incidence of 15%–7% of patients.5 This is due to a greater awareness of the problem, better risk prevention measures, and improved iodinated CM with less renal toxicity. However, many cases of CI-AKI continue to occur because of the ever-increasing numbers of procedures requiring contrast. Nash et al.6 reported that radiographic CM were the third most common cause of hospital-acquired renal failure (after decreased renal perfusion and nephrotoxic medications) and were responsible for 11% of cases.
In this study, we aimed to compare the effect of ionic versus nonionic CM on the development of CI-AKI in patients undergoing primary PCI.
2 Methods 2.1 Inclusion and exclusion criteriaIn our study, we included 102 patients who were admitted to the Critical Care Department, Cairo University Hospital and who presented with STEMI and had primary PCI. We excluded patients with end-stage kidney disease on dialysis and patients who died within less than 72 hours from admission. Informed consent was taken from all patients for participation in the study.
2.2 Data collectionPatients’ data included demographics and baseline characteristics, serial serum creatinine (SCr; Fig. 1), electrocardiogram, LV function assessment with transthoracic echocardiography (within 12 hours of PCI), hemodynamics, and need for inotropic support or intra-aortic balloon pump (IABP). The details of the procedure were recorded including type and volume of CM used, type of the procedure, culprit lesion, and stenting, also the outcome data including the development of AKI, the need for dialysis, and mortality.
 Figure 1:
Figure 1: Creatinine levels in CI-AKI patients, both ionic and nonionic groups.
Patients were divided into 2 groups according to the type of CM received during the intervention. We used CM that are available in the Egyptian market and that are routinely used for cardiac interventions in the Critical Care Department, Cairo University Hospital. The CM used was either the ionic hyperosmolar CM ioxitalamate (Telebrix) or the nonionic low- osmolar CM iohexol (Omnipaque). Choice of the CM was according to the operators’ discretion. We used the CI-AKI definition recommended by the 2012 kidney disease improving global outcomes (KDIGO) workgroup7 that defined AKI as increase in SCr by >0.3 mg/dL within 48 hours, or increase in SCr to >1.5 times baseline, or urine volume < 0.5 mL/kg/h for 6 hours.
We also used a 3-day window period to monitor the development of CI-AKI, this is in concordance with the Society of Urogenital Radiology8 and the Contrast-Induced Nephropathy Consensus Panel.9
2.3 Statistical analysisData were collected and coded prior to analysis using the professional Statistical Package for Social Science 21 (SPSS 21) Data were expressed as mean and standard deviation. Categorical data were expressed as percentages. Student t test and Mann- Whitney test were used for comparing data. Chi-square test was used for all categorical data to test for the presence of an association. P value < .05 was considered significant.
3 ResultsA total number of 102 patients were enrolled in the current study. A total of53 patients (52.0%) received the ionic CM ioxitalamate (Telebrix), whereas 49 patients (48.0%) received the nonionic CM iohexol (Omnipaque). The study included 79 males (77.5%) and 23 females (22.5%) with a mean age of 55.5 ± 10.4 years. Average length of stay was 4.3 ± 0.8 days (range: 4–7). Of all patients, 50% were smokers, 45% had diabetics, 44% were hypertensive, 30.9% had family history of coronary artery disease, and 19.6% of them were dyslipidemic. Only 7.8% of the patients had preexisting renal dysfunction (SCr > 1.5 mg/dL). Around half of the patients (49%) had ejection fraction < 55%. Patients had a mean body mass index of 26.5 ± 3.
As for the hemodynamic profile, 78 patients (76.5%) were hemodynamically stable (mean arterial blood pressure > 65 mm Hg without inotropic or vasopressor support), whereas 24 patients (23.5%) were hemodynamically unstable (mean arterial blood pressure < 65 mmHg or requiring inotropic or vasopressor support or use of IABP). Four patients needed IABP support (3.9%).
Primary PCI was done in all patients with stenting in 82 patients (80.4%) and percutaneous transluminal coronary angioplasty in 20 patients (19.6%). Culprit vessel was the left anterior descending in 63 patients (61.8%), the right coronary artery in 28 patients (27.5%), and the left circumflex in 11 patients (10.8%). Of targeted lesions, 52 patients had proximal lesions (51.0%), 46 patients had mid-segment lesions (45.1%), and 4 patients had distal lesions (3.9%). Complete revascularization was achieved in 12 patients (11.8%) and culprit-only intervention was performed in 90 patients (88.2%). The mean volume of contrast used for all patients was 250.0 ± 59.3 mL. Eleven patients received contrast volume exceeding the maximum allowed contrast dose (MACD) as defined by Ciagorra et al.10 by this equation [5 mL x body weight (kg)/baseline SCr (mg/dL)]. Seventeen patients (16.7%) experienced acute kidney injury. Only 1 patient in the ionic group showed decreased urine output (urine output < 0.5 mL/kg/h for 6 hours), he had progressive rise in creatinine values, and was the only patient who needed renal replacement therapy.
In comparison (Table 1), there were no significant differences between both groups concerning the demographics and baseline characteristics or hemodynamic instability. There were also no significant differences between the 2 groups in regard to the type of intervention (stenting versus percutaneous transluminal coronary angioplasty) or revascularization approach (culprit- only versus complete). Although the mean volume of contrast medium received was significantly higher in patients who received the nonionic contrast (262.2 ± 38.9 mL for the nonionic group versus 238.7 ± 71.8 mL for the ionic group; P = .044), yet when the volume of contrast was adjusted to the patients’ weight and baseline SCr for each patient, there was no significant difference between the number of patients who exceeded the MACD in both groups (P = .323).
Table 1 - Clinical, procedural variables, and outcome in both groups. Ionic contrast media Nonionic contrast media P value Age 55.2 ± 10.2 55.9 ± 10.7 .767 Gender (male) 44 (83.0%) 35 (71.4%) .123 Diabetes mellitus 25 (47.2%) 21 (41.9%) .406 Hypertension 25 (47.2%) 20 (40.8%) .328 Smoking 25 (47.2%) 2 (53.1%) .346 Dyslipidemia 10 (18.9%) 10 (20.4%) .521 Previous renal impairment 4 (7.5%) 4 (8.2%) .597 LVEF < 55% 30 (56.6%) 20 (40.8%) .081 Hemodynamic instability 11 (20.8%) 13 (26.5%) .325 Complete revascularization 6 (11.3%) 6 (12.2%) .444 Stenting 42 (.79.2%) 40 (81.6%) .382 Contrast volume 238.7 ± 71.8 262.2 ± 38.9 .044 Patients exceeding MACD 5 6 .323 AKI 10 (18.9%) 7 (14.3%) .363 Mortality 2 (0.03%) 2 (0.04%) .66LVEF, left ventricular ejection fraction.
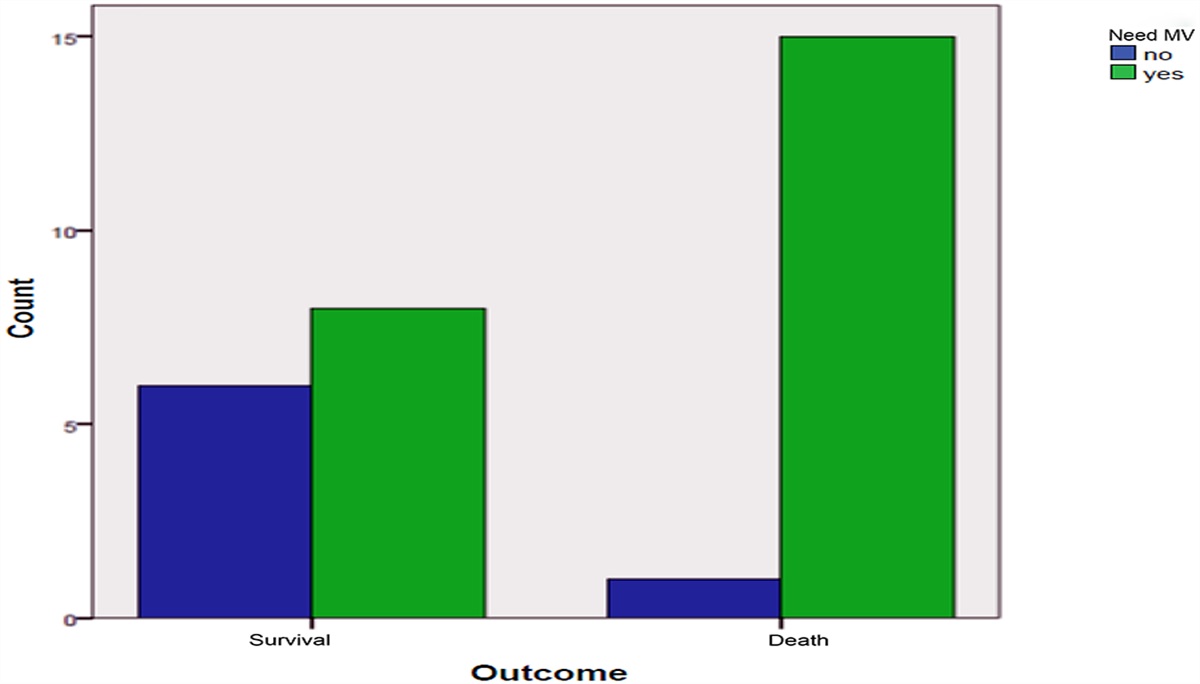
CI-AKI was recorded in 10 of the 53 patients in the ionic group (18.9%), and in 7 of the 49 patients in the nonionic group (14.3%). So, no significant difference could be observed between the 2 groups in the incidence of CI-AKI and P value was .36. Four patients passed away (3.9%). They suffered cardiogenic shock and needed inotropic support. No significant difference in mortality was observed between the 2 groups (2 patients died in each group) (P = .66).
In this study, 17 of 102 patients developed CI-AKI (16.7%). Older age (61.8 ± 8.0 years), hypertension, and preexisting renal dysfunction were significantly associated with development of CI-AKI with P values of .006, .016, and .025, respectively. Multivariable regression analysis showed that older age and hypertension are independent predictors of CI-AKI (Table 2). Our results showed a potentially protective effect of smoking upon occurrence of AKI but univariate regression failed to show a statistical significance for this input. No significant differences were found in baseline SCr or other routine laboratory test results between those who developed CI-AKI and those who did not.
Table 2 - Clinical, procedural variables, and outcome in patients with and without CI-AKI. AKI No AKI P value Age 61.8 ± 8.0 54.3 ± 10.4 .006 BMI 26.1 ± 2.6 26.6 ± 3.1 .560 Gender (male) 4 (23.5%) 19 (22.4%) .568 Diabetes mellitus 9 (52.9%) 37 (43.5%) .327 Hypertension 12 (70.6%) 33 (38.8%) .016 Smoking 3 (17.6%) 48 (56.5%) .003 Dyslipidemia 4 (23.5%) 16 (18.8%) .438 Previous renal impairment 4 (23.5%) 4 (4.7%) .025 LVEF < 55% 8 (47.1%) 42 (49.4%) .536 Baseline serum creatinine 1.2 ± 0.3 1.1 ± 0.3 .064 Contrast volume 258.8 ± 50.7 248.2 ± 61.0 .504 Patients exceeding MACD 4 (23.5%) 7 (8.2%) .031 Hemodynamic instability 7 (41.2%) 17 (20.0%) .03 Complete revascularization 5 (29.4%) 7 (8.2%) .027 Stenting 13 (76.5%) 69 (81.2%) .438 Mortality 4 (23.5%) 0 <.001BMI, body mass index; LVEF, left ventricular ejection fraction.
Although there was no significant difference in the mean volume of contrast given between patients who developed AKI (258.8 ± 50.7 mL) and those who did not (248.2 ± 61.0 mL) with a P value of .504, yet CI-AKI developed more frequently in patients who received contrast volume exceeding the MACD (23.5% versus 8.2%) with a significant P value of .03.
The incidence of CI-AKI was significantly higher in the hemodynamically unstable group: 41.2% versus 20% in the hemodynamically stable group, with a significant P value of .03. Patients who had complete revascularization approach were more likely to develop CI-AKI. Five of 17 patients who developed AKI had complete revascularization (29.4%), whereas only 7 of 85 patients who did not develop AKI had complete revascularization (8.2%) with a significant P value of .027. In patients who had complete revascularization, there was a nonsignificant trend of being more hemodynamically unstable compared to patients who had culprit-only revascularization (P = .299).
In our study, 4 of 102 patients died (3.9%), all of whom developed AKI, making a significant relation between CI-AKI and mortality as 23.5% of the patients who developed CI-AKI eventually died (P < .001). Of the 4 mortality, 2 were males, 2 were females, 3 had diabetics, 3 were hypertensive, 3 had anterior myocardial infarction, and 1 had inferior myocardial infarction. All were in the hemodynamically unstable group and had no preexisting renal dysfunction. All suffered from cardiogenic shock with noradrenaline support.
4 DiscussionCI-AKI is a frequent complication in acute myocardial infarction following primary PCI, even in patients with a normal baseline renal function, that may be explained by LV dysfunction and hemodynamic instability resulting in impaired systemic perfusion and the impossibility to implement renal prophylactic measures before exposure to contrast medium in this setting.11 A study performed by Rihal et al.12 showed that acute myocardial infarction within 24 hours before administration of the CM is a risk factor for CI-AKI (P = .0006). The incidence of CI-AKI with Primary PCI varies widely across the literature depending partially on the study-population risk factors, procedural variations, and the thresholds used to define CI-AKI.
In our study, 17 of 102 patients (16.7%) experienced CI-AKI after Primary PCI. Other studies showing comparable results included incidence rates of 19%,13 28%,14 16.1%,15 and 20%.16
Regarding the difference in the incidence of CI-AKI between the ionic and nonionic CM, in our study, CI-AKI was recorded in 10 of the 53 patients in the ionic group (18.9%), and in 7 of the 49 patients in the nonionic group (14.3%). This difference between the 2 groups was found to be statistically insignificant (P = .36). Similarly, other studies comparing different types of ionic and nonionic CM on the incidence of CI-AKI found comparable results. In 1989, Schwab et al.17 studied 443 patients who were randomized to receive either the ionic CM diatrizoate or the nonionic CM iopamidol during cardiac catheterization. They were unable to demonstrate a difference in the incidence of nephrotoxicity between both groups.
Even in high-risk patients, that is, those with diabetes mellitus (DM), heart failure, or preexisting renal insufficiency, there was no significant difference in the incidence of CI-AKI between both groups (17% in the ionic versus 15% in the nonionic). The study concluded that there was no advantage in using a nonionic contrast agent to prevent renal injury mediated by contrast material.17 In the same year, in a study on 347 high-risk patients, Gomes et al.18 compared the effect of an ionic CM versus the nonionic CM iohexol on the development of AKI in angiography patients, and found no statistically significant difference between the 2 groups (10% for ionic versus 5.5% for the nonionic group) and this was although the ionic group had greater number of patients who were of advanced age, had greater volume of contrast, and had preexisting renal dysfunction.18
Other studies found a relative benefit of the nonionic CM over the ionic CM in some high-risk groups. In 1991, in a study on 307 patients with renal impairment, Taliercio et al.19 compared the nephrotoxic effects of the ionic hyperosmolar CM diatrizoate and the nonionic low-osmolar CM iopamidol. They found that iopamidol is less nephrotoxic than diatrizoate in high-risk patients at cardiac angiography. However, the difference in nephrotoxicity was of no major clinical significance in the majority of high-risk patients and could not be documented in insulin-using diabetic patients.19 Similarly, Rudnick et al.20 compared the incidence of nephrotoxicity occurring with the nonionic contrast agent, iohexol, and the ionic contrast agent, meglumine/sodium diatrizoate, in a prospective, randomized, double-blind multicenter trial on 1196 patients undergoing cardiac angiography. The study concluded that those with preexisting renal insufficiency alone or combined with DM are at higher risk for acute contrast nephrotoxicity, and that the incidence of acute nephrotoxicity in these high-risk patients is significantly less with the nonionic CM iohexol compared to the ionic contrast agent diatrizoate.20 Moreover, the ICON (Ionic versus non-ionic Contrast to Obviate worsening Nephropathy after angioplasty in chronic renal failure patients) study by Mehran et al.21 compared nephrotoxicity of the nonionic iso- osmolar CM iodixanol versus the ionic low-osmolar CM ioxaglate in patients with chronic renal insufficiency undergoing coronary angiography. The study concluded that in high-risk patients undergoing coronary angiographic procedures, use of the nonionic iso-osmolar CM iodixanol does not reduce renal deterioration in patients with renal impairment, compared with the ionic low-osmolar CM ioxaglate.21
In our study, we examined the role of various risk factors on the development of CI-AKI. The study showed that older age is significantly related to CI-AKI in PPCI. Patients who developed AKI had a mean age of 61.8 ± 8.0 years compared to a mean age of 54.3 ± 10.4 years for those who did not develop AKI (P = .006), and on multivariable regression analysis, older age was found to be an independent predictor of CI-AKI. Similarly, this was shown in other studies.13,22–24 Levy et al.,22 in a study on 208 patients with acute myocardial infarction who underwent PCI, found that an age of 75 years or more was an independent risk factor for Contrast induced nephropathy (odds ratio = 5.28, P = .0009).22 Mehran et al.,23 in their study to develop a risk score for CIN, found that old age > 75 years was one of the independent predictors of CI-AKI (P < .0001). The high incidence of CI-AKI in elderly patients may be attributed to age-related changes such as dominance of renal vasoconstrictive forces over vasodilator forces due to defective prostaglandin synthesis, more difficult vascular access because of tortuosity, calcification of vessels requiring greater amounts of CM, and the presence of renovascular diseases.25–27
In our study, there was no significant difference in the incidence of CI-AKI among patients with and without DM. Diabetic patients constituted 52.9% of patients who developed CI-AKI compared to 43.5% of those who did not develop CI-AKI (P = .327). In contrast to our study, most studies found that DM alone or combined with preexisting renal insufficiency was associated with increased risk of CI-AKI.12,22,28–32 Mehran et al.,23 in their study to develop a risk score for CIN, found that DM was one of the independent predictors of CI-AKI (P < .0001). Similar to our study, other investigators found no significant correlation between DM and CI- AKI, for example, in 2004, Marenzi et al.13 in their study on 179 patients undergoing primary PCI found that there was no significant correlation between DM and CI-AKI. In this study, 7% of the patients who developed AKI were diabetic compared to 12% of patients who did not develop CI-AKI (P = .58).13 Also in 2006, Valente et al.,24 in a study on 194 patients undergoing urgent PCI, found that there was no significant relation between DM and CI-AKI (P = .11).24
Our study showed that hypertension is significantly related to CI-AKI in PPCI; 70.6% of patients who developed AKI were hypertensive compared to 38.8% of those who did not develop AKI (P = .016), and on multivariable regression analysis, hypertension was found to be an independent predictor of CI- AKI. In the study to develop a risk score for CIN, Mehran et al.,23 found that hypertension significantly increased the risk of CI-AKI on univariate analysis (P < .0001). However, in contrast to our study, other investigators studying the primary PCI population found no significant correlation between hypertension and developing CI-AKI.13,15,24
Our study showed that patients with preexisting renal dysfunction had significantly increased risk of developing CI- AKI. Preexisting renal dysfunction was present in 23.5% of patients who developed CI-AKI versus only 4.7% of those without CI-AKI (P = .025). Other studies showed comparable results.13,15,24,28 In Mehran risk score for CIN, CKD was one of the independent predictors of CI-AKI (P < .0001).23
Our study showed that patients with hemodynamic instability had significantly increased risk of developing CI-AKI. Hemodynamic instability was present in 41.2% of patients who developed CI-AKI versus 20% of those without CI-AKI (P = .03). This correlation has been repeatedly shown in previous studies.15,23,29
The volume of contrast used has been repeatedly shown to have a significant correlation with the development of CI-AKI. Marenzi et al.,13 in their study on 179 patients undergoing primary PCI, showed that there was significantly increased risk of developing CI-AKI with higher contrast volumes (378 ± 200 mL for patients who developed AKI compared to 286 ± 125 mL for patients who did not develop CI-AKI; P = .008). They also calculated the significance of exceeding a contrast volume limit of 300 mL in relation to development of CI-AKI and found that it was significant.13 In the former study as in other studies,15,28 the correlation was made between developing CI-AKI and the total or the mean volume of contrast. In 2002, Freeman et al.30 demonstrated that CM doses above 5 cc x body weight (kg)/SCr were associated with a need for dialysis, whereas unadjusted CM dose was not a univariate predictor of contrast-induced dialysis. Other investigators showed similar results.31 In our study, there was no significant difference in the mean volume of contrast given between patients who developed CI-AKI (258.8 ± 50.7 mL) and those who did not (248.2 ± 61.0) (P = .504). However, we found that there was a significant increase in the risk of CI-AKI in patients who received contrast volume exceeding the MACD [5 cc x body weight (kg)/SCr (23.5% versus 8.2%; P = .031].
In our study, patients who had complete revascularization approach had significantly higher risk of developing CI-AKI. Complete revascularization was achieved in 29.4% of patients who developed CI-AKI compared to 8.2% of patients who did not develop AKI (P = .027). In patients who had complete revascularization, there was a nonsignificant trend of being more hemodynamically unstable compared to patients who had culprit-only revascularization (P = .299). In contrast to our findings, a meta-analysis compared the risk of CI-AKI during complete revascularization versus Infarct related artery revascularization in STEMI patients. They found no significant difference in the risk of CI-AKI between the 2 groups (1.3% in complete revascularization versus 1.9% in IRA revascularization; P = .4). There was a nonsignificant reduced trend of CI-AKI in the complete revascularization group despite increased contrast volume used when compared to IRA revascularization group.32 Similar finding was found on other studies such as the PRAMI trial in 2013 (P = .84)33 and the CVLPRIT trial in 2013.34
5 ConclusionsCI-AKI frequently complicates primary PCI and is associated with higher incidence of mortality. The incidence of CI-AKI seems to be comparable between ionic and nonionic CM postprimary PCI. Optimizing periprocedural hemodynamic stability and using the least possible volume of CM can minimize the risk of CI-AKI.
References [1]. Go AS, Mozaffarian D, Roger VL, et al. American Heart Association Statistics Committee and Stroke Statistics SubcommitteeExecutive summary: heart disease and stroke statistics 2013 update: a report from the American Heart Association. Circulation 2013;127(1):143–152. [2]. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003;361(9351):13–20. [3]. Zijlstra F, Hoorntje JCA, de Boer MJ, et al. Long-term benefit of primary angioplasty as compared with thrombolytic therapy for acute myocardial infarction. N Engl J Med 1999;341(19):1413–1419. [4]. Takii T, Yasuda S, Takahashi J, et al. MIYAGI-AMI Study InvestigatorsTrends in acute myocardial infarction incidence and mortality over 30 years in Japan: report from the MIYAGI-AMI Registry Study. Circ J 2010;74:93–100. [5]. Bartholomew BA, Harjai KJ, Dukkipati S, et al. Impact of nephropathy after percutaneous coronary intervention and a method for risk stratification. Am J Cardiol 2004;93(12):1515–1519. [6]. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis 2002;39(5):930–936. [7]. Kellum JA, Lameire N, Aspelin P, et al. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl 2012;2(1):1–138. [8]. Morcos SK, Thomsen HS. European Society of Urogenital Radiol- ogyEuropean Society of Urogenital Radiology guidelines on administering contrast media. Abdom Imaging 2003;28:187–190. [9]. Solomon R, Deray G. Consensus Panel for CINHow to prevent contrast- induced nephropathy and manage risk patients: practical recommendations. Kidney Int Suppl 2006;69:S51–S53. [10]. Cigarroa RG, Lange RA, Williams RH, Hillis D. Dosing of contrast material to prevent contrast nephropathy in patients with renal disease. Am J Med 1989;86(C):649–652. [11]. Marenzi G, Assanelli E, Marana I, et al. N-acetylcysteine and contrast- induced nephropathy in primary angioplasty. N Engl J Med 2006;354(26):2773–2782. [12]. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation 2002;105(19):2259–2264. [13]. Marenzi G, Lauri G, Assanelli E, et al. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 2004;44(9):1780–1785. [14]. Senoo T, Motohiro M, Kamihata H, et al. Contrast-induced nephropathy in patients undergoing emergency percutaneous coronary intervention for acute coronary syndrome. Am J Cardiol 2010;105(5):624–628. [15]. Narula A, Mehran R, Weisz G, et al. Contrast-induced acute kidney injury after primary percutaneous coronary intervention: results from the HORIZONS-AMI substudy. Eur Heart J 2014;35(23):1533–1540. [16]. Kobalava ZD, Villevalde SV, Gaskina AA, Mayskov VV, Moiseev VS. Contrast-induced acute kidney injury after primary percutaneous coronary interventions: prevalence, predictive factors, and outcomes [in Russian]. Ter Arkh 2015;87(6):50–55. [17]. Schwab SJ, Hlatky MA, Pieper KS, et al. Contrast nephrotoxicity: a randomized controlled trial of a nonionic and an ionic radiographic contrast agent. N Engl J Med 1989;320(3):149–153. [18]. Gomes AS, Lois JF, Baker JD, McGlade CT, Bunnell DH, Hartzman S. Acute renal dysfunction in high-risk patients after angiography: comparison of ionic and nonionic contrast media. Radiology 1989;170(1 Pt 1):65–68. [19]. Taliercio CP, Vlietstra RE, Ilstrup DM, et al. A randomized comparison of the nephrotoxicity of iopamidol and diatrizoate in high risk patients undergoing cardiac angiography. J Am Coll Cardiol 1991;17(2):384–390. [20]. Rudnick MR, Goldfarb S, Wexler L, et al. Nephrotoxicity of ionic and nonionic contrast media in 1196 patients: a randomized trial. The Iohexol Cooperative Study. Kidney Int 1995;47(1):254–261. [21]. Mehran R, Nikolsky E, Kirtane AJ, et al. Ionic low-osmolar versus nonionic iso-osmolar contrast media to obviate worsening nephropathy after angioplasty in chronic renal failure patients: the ICON (Ionic versus non-ionic Contrast to Obviate worsening Nephropathy after angioplasty in chronic rena. JACC Cardiovasc Interv 2009;2(5):415–421. [22]. Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality: a cohort analysis. JAMA 1996;275(19):1489–1494. [23]. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol 2004;44(7):1393–1399. [24]. Valente S, Lazzeri C, Giglioli C, et al. Contrast-induced nephropathy in urgent coronary interventions. J Cardiovasc Med (Hagerstown) 2006;7(10):737–741. [25]. Rich MW, Crecelius CA. Incidence, risk factors, and clinical course of acute renal insufficiency after cardiac catheterization in patients 70 years of age or older: a prospective study. Arch Intern Med 1990;150(6):1237–1242. [26]. Gleeson TG, Bulugahapitiya S. Contrast-induced nephropathy. Am J Roentgenol 2004;183(6):1673–1689. [27]. Detrenis S, Meschi M, Musini S, Savazzi G. Lights and shadows on the pathogenesis of contrast-induced nephropathy: state of the art. Nephrol Dial Transplant 2005;20(8):1542–1550. [28]. Evola S, Lunetta M, Macaione F, et al. Risk factors for contrast induced nephropathy: a study among Italian patients. Indian Heart J 2012;64(5):484–491. [29]. Dangas G, Iakovou I, Nikolsky E, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol 2005;95(1):13–19. [30]. Freeman RV, O’Donnell M, Share D, et al. Nephropathy requiring dialysis after percutaneous coronary intervention and the critical role of an adjusted contrast dose. Am J Cardiol 2002;90(10):1068–1073. [31]. Brown JR, Robb JF, Block CA, et al. Does safe dosing of iodinated contrast prevent contrast-induced acute kidney injury? Circ Cardiovasc Interv 2010;3(4):346–350. [32]. Mukete BN, Riehl R, Mogabgab O, et al. Risk of contrast induced nephropathy during complete revascularization compared to infarct- related artery revascularization in the setting of ST-segment elevation myocardial infarction: a meta-analysis. J Am Coll Cardiol 2016;67(13 Suppl):104. [33]. Wald DS, Morris JK, Wald NJ, et al. Randomized trial of preventive angioplasty in myocardial infarction. N Engl J Med 2013;369(12):1115–1123. [34]. Kelly DJ, McCann GP, Blackman D, et al. Complete Versus culpritLesion only PRimary PCI Trial (CVLPRIT): a multicentre trial testing management strategies when multivessel disease is detected at the time of primary PCI: rationale and design. EuroIntervention 2013;8(10):1190–1198.
Comments (0)