Novel use of Partial Diversion Stoma—Bishop Koop and Santulli Stoma in Adults
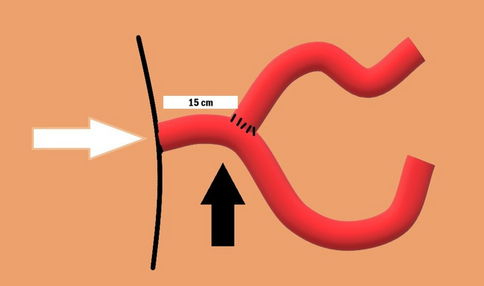
Diversion stomas are helpful in preventing anastomotic breakdown, but small bowel stomas are known for high output, resulting in fluid loss and electrolyte imbalances. In this study, we utilized the Bishop Koop and Santulli stomas to prevent high output, provide nutrition through faster re-establishment of enteral feeds, and early restoration of continuity of the GI tract. In this report, we present seven adult patients who were operated on for small bowel diseases under emergency settings, and stomas were fashioned. Bishop Koop and Santulli stomas were formerly used by pediatric surgeons, and we utilized the same in adults due to the hostile abdomen, sepsis, and disrupted physiology with a high possibility of a leak if primary anastomosis was attempted. Serial monitoring of stoma output, nutritional status, and the timing of initiation of enteral feeding were noted. Four patients had a linear and significant decrease in the stoma output over a period of 3 weeks and tolerated early enteral feeds. One patient developed a minor leak after stoma closure and settled with supportive measures. Two patients died postoperatively. We found both Bishop Koop and Santulli stomas beneficial in adult patients. In addition to the reduction of morbidity associated with high-output stomas, they were useful for assessment through contrast studies and enteroscopies. Therapeutically, we have used the distal loop for early feeding. We also noticed that the stoma behaves as a “partial continuity stoma,” thus reducing the dependency on total parenteral nutrition, thereby reducing the financial burden, especially in resource-poor establishments. This innovation of a pre-existing surgical method can be used for both diagnostic and therapeutic benefits, especially when the physiology is unfavorable.





Comments (0)