The purpose of this study was to test criterion validity of the Dynamic Imagine Grade of Swallowing Toxicity (DIGESTV2, Version 2) for use in post-stroke populations against validated measures of swallowing impairment (MBSImP) and oral intake (FOIS). DIGESTV2 applied in a post-stroke cohort demonstrated grade differentiation in the expected direction for both MBSImP Pharyngeal Total (PT) scores and FOIS (Figs. 2 and 3). However, there was some overlap between mild and moderate grades (1–2) and moderate to severe grades (2–3) in this dataset.
Criterion validity established between DIGESTV2 grade and MSBImP PT scores in this post-stroke cohort was similar to the original validation study in cancer [10]. In this study, inter-rater reliability for post-stroke dysphagia DIGESTV2 grades were highly similar to the initial validation study for the DIGESTV2 method [10] (ƙ = 0.69 vs. 0.67, respectively), along with inter-rater reliability for safety (ƙ = 0.70 vs. 0.67). Inter-rater reliability for efficiency was lower in this study, as compared to the initial validation study (ƙ = 0.52 vs. 0.81). This could be due to population differences between stroke and head and neck cancer, particularly related to oral inefficiencies known to occur in post-stroke dysphagia [16,17,18]. It is possible that oral-phase impairments made pharyngeal residue ratings more difficult to reliably grade across raters due to aberrant patterns of bolus movement, or piecemeal swallowing.
The DIGESTV2 results here were derived from patients tested using the MBSImP bolus protocol. This widely used and validated bolus protocol shares common IDDSI 0, IDDSI 4, and IDDSI 7 bolus trials with the bolus protocol used in the development of DIGEST (V1 and V2) at MD Anderson Cancer Center. However, the bolus protocols differ in several ways (shown in Table 7): more IDDSI 0 thin liquid boluses were used in the MD Anderson bolus protocol (6 boluses in DIGESTV2 vs. only 4 in MBSImP), and thicker boluses (IDDSI 2 and 3) are used as part of standard in MBSImP bolus protocol but are used only as clinically indicated at MD Anderson. To our knowledge, this is the first investigation to evaluate the psychometrics of DIGESTV2 in a population tested using the MBSImP bolus protocol with results suggesting DIGESTV2 is feasible using the MBSImP bolus protocol and may offer a valid overall DIGESTV2 result. This conclusion requires further testing in a larger sample representing diverse clinical populations, which is currently underway in an ongoing clinical trial.
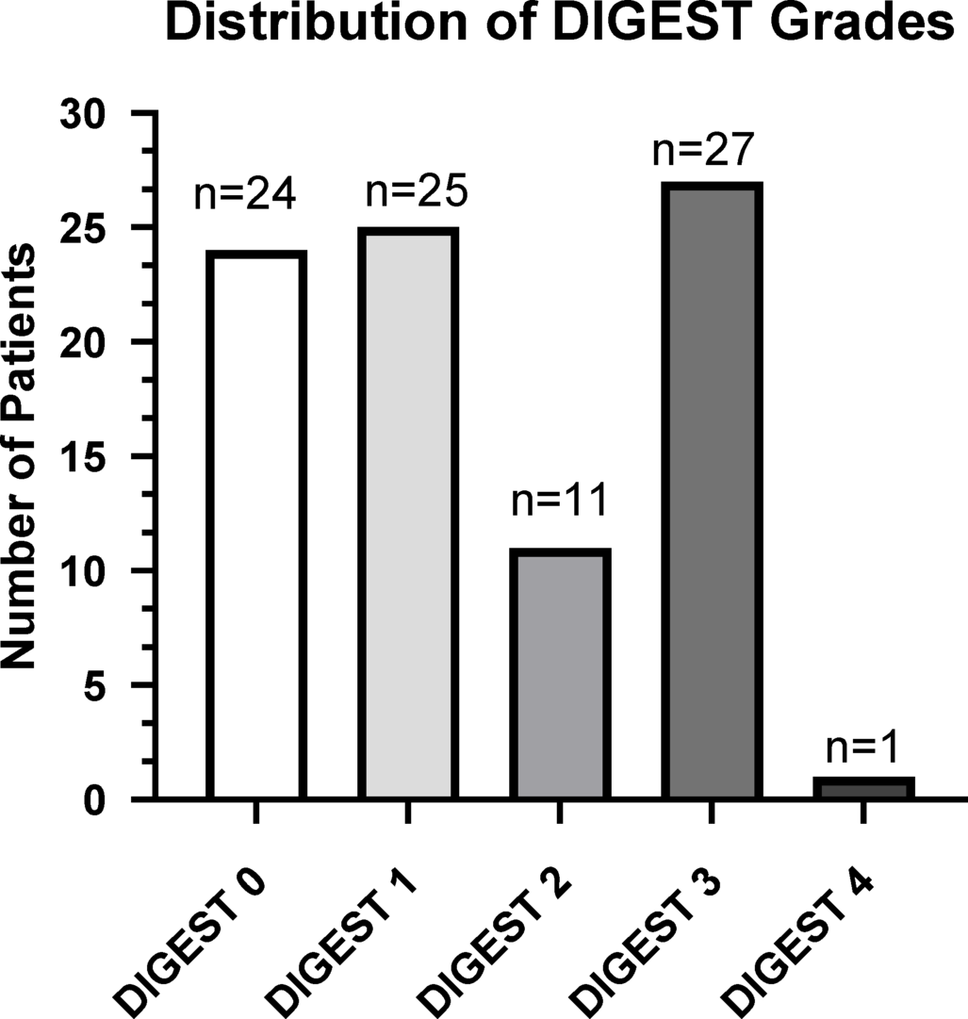
Table 7 MD Anderson Bolus Protocol (used in DIGESTV2 Validation) compared to MBSImP Bolus ProtocolTwo of the analyses fell short of desired results. First, we failed to demonstrate ordinality for mid-grades. There are several possible explanations for the overlap in grades. There was an uneven distribution of DIGESTV2 grades in this convenience sample with limited representation of Grades 2 and 4 DIGESTV2 results in the dataset: n = 11 for Grade 2 and n = 1 for Grade 4, compared to n = 25 for Grade 1, and n = 27 for Grade 3. This presents a limited and uneven representation which lowered the number of patients per bin, which could have resulted in overlap of these grades. Differences between bolus administration protocols could also be contributing to this overlap. The underlying logic of DIGESTsafety decision tree makes it more difficult to catch moderate safety impairment (S2 Grade) when there are less than 5 thin liquid bolus trials in the standard protocol [10, 12] Further, given that this clinical dataset was acquired using the MBSImP protocol, including standard thicker consistencies, the DIGESTV2 grades could have been shifted away from more mild-to-moderate Grade 2 to a more moderate Grade 3. However, DIGESTV2 grade shift by standard inclusion of thick liquids is rare (< 5% rate) based on recent data [34].
Another possible contributing factor to grade overlap found in this study is the high number of skipped IDDSI 7 trials in this sample (n = 32 patients). The cracker bolus is often skipped for many stroke patients with severe oral inefficiencies, which is at the discretion of the administering SLP to determine safety of the cracker bolus trial. However, without the cracker trial it is impossible to derive moderate efficiency grade (E2 Grade) using DIGESTV2; as a result, there was only a single grade of Efficiency 2 in the whole sample (Table 2). The high frequency of skipped cracker trials in this data set provides an explanation for the low number of E2 Grades. This inequity could have contributed to an underpowered analysis, resulting in grade overlap. Even with the statistical overlap in grades, likely due to one or all of the factors discussed, the DIGESTV2 grades for this post-stroke cohort still followed an expected psychometric pattern of increasing severity in grade with worsening MBSImP Pharyngeal Total score (Fig. 2).
Finally, it is important to consider the clinical differences between a post-stroke and a head and neck cancer population that may be influential in grade distribution, and the limitations in what Pharyngeal Total scores are capturing. DIGESTV2 ratings account for only pharyngeal swallowing impairments in safety and efficiency, thus, it is unsurprising that there was no correlation between OT scores and DIGESTV2. Specific to population, patients with post-stroke dysphagia are known to have significant oral-phase swallowing deficits [22, 23, 27, 35], and to what degree oral impairments impact or influence overall pharyngeal swallowing is not known. One recent statistical model suggests some correlation between oral and pharyngeal domains, but a weak correlation at best [11]. However, there are physiologic links between oral and pharyngeal domains– for example, initiation of pharyngeal swallow (MBSImP component 6) is considered as a part of the oral domain as tongue movement is closely related to swallow initiation [36]. In this current study, there was no relationship between oral phase deficits (MBSImP OT) and overall DIGESTV2 grade (Fig. 2). Interestingly, the average OT scores are very similar amongst grades (except for n = 1 of Grade 4).
Statistical modeling further supports the notion that Pharyngeal Total scores could be influenced by disease specific impairments in swallowing [11]. Large statistical models have demonstrated that, since the summative Oral Total and Pharyngeal Total scores are made up of individual component scores, they are influenced by the degree of impairment reflected within the individual component scores. These component scores likely vary depending on population-specific impairments, resulting in a higher or lower pharyngeal total based on the clinical population [11]. This is evident in the data shown here as well: when comparing Pharyngeal Total scores amongst DIGESTV2 grades in this study (Fig. 2) to the original DIGESTV2 validation study, we see that Pharyngeal Total scores by DIGESTV2 grade are slightly lower in stroke as compared to the original head and neck cancer population (see Fig. 3 in Hutcheson et al. 2016). Expected clinical differences in swallow physiology after stroke versus HNC fit this finding, and importantly the data show similar differentiation of DIGESTV2 grades in an expected direction suggesting promise that DIGESTV2 ratings are adaptable to other patient populations outside of head and neck cancer.
Limitations and Future Directions
This was a retrospective study, thus, we were limited to only data available in the database, which did not include exact time post-stroke, lesion profiling, or stroke severity. This post-stroke cohort was limited to those with acute dysphagia post-CVA; as a result, some boluses were not administered given the acuity and clinical nature of the modified barium swallow studies, namely the cracker bolus was skipped for roughly 1/3 of the cohort (n = 32). Repeating this work in a larger post-stroke cohort, across the continuum of stroke recovery, would allow for better representation of all safety and efficiency profiles to determine if grade overlap still exits, and to capture a broader range of more severe impairment (i.e. more Efficiency Grade 2, and more Grade 4) and a more even distribution of DIGESTV2 grades. It is possible that oral-phase issues could have impacted boluses administered during this clinical study, for example skipping of cracker bolus due to mastication impairment and concerns of patient safety, which could have impacted grading distribution as well. More data in these domains will help either confirm preliminary evidence of use of DIGESTV2 in post-stroke populations or indicate need for refining the protocol to better suit specific patient populations. Based on findings of this study, it is likely that a larger sample with more even grade distribution would further differentiate the mild-moderate grades and further strengthen evidence for the validity of the tool in a post-stroke population. Finally, as discussed, there are differences in bolus protocols between MBSImP and the original boluses used in the DIGEST and DIGESTV2 validation studies with the main differences being the addition of thickened liquids. While preliminary data suggest that the DIGESTV2 protocol is flexible when a variety of boluses are administered [34, 37], potential differences between bolus administration approaches are being addressed by ongoing investigations.



Comments (0)