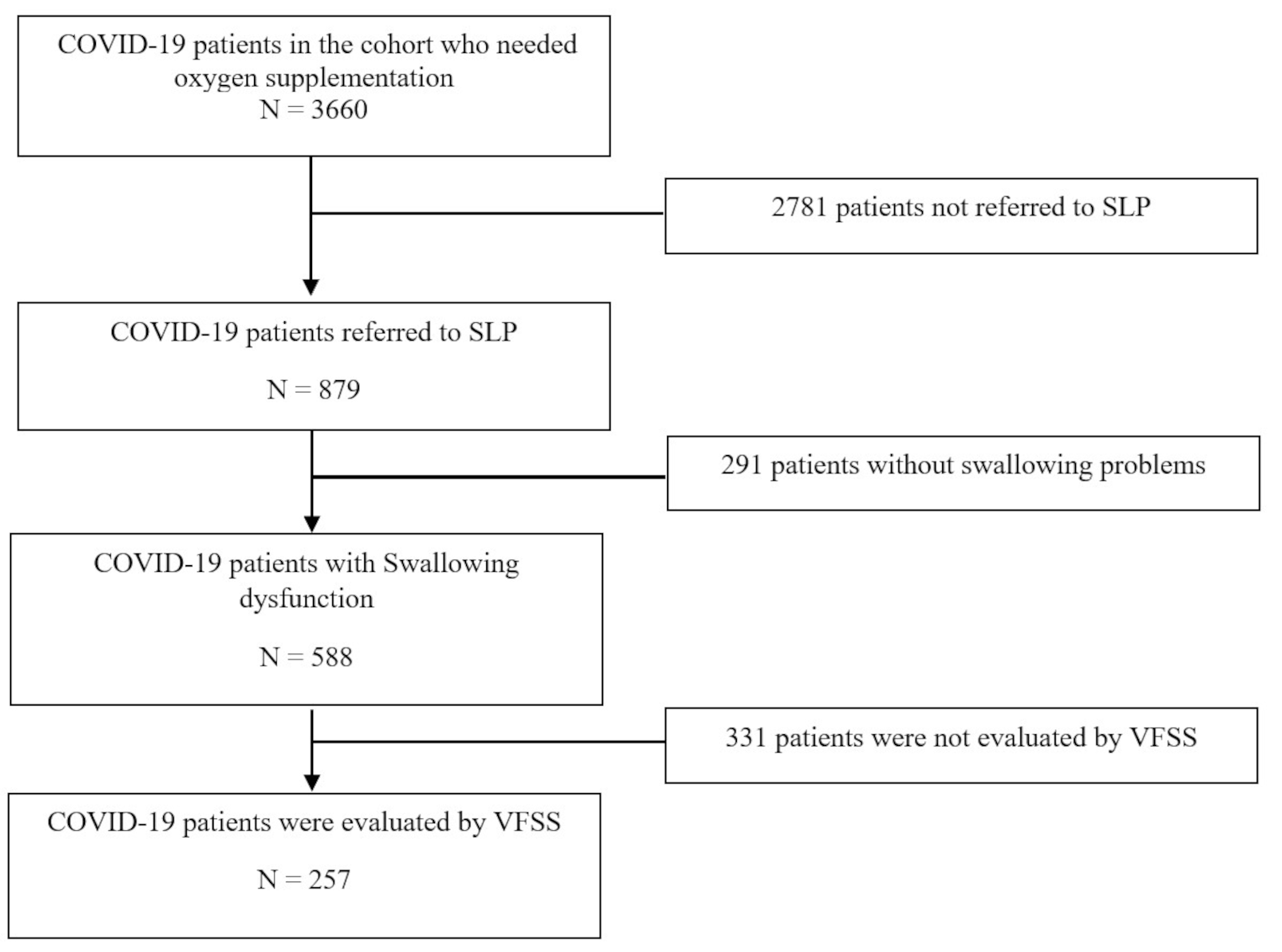
The search yielded 12,674 articles after de-duplication. 3,108 articles’ titles and abstracts (25%) were screened by both reviewers; 12,366 were excluded. 308 articles advanced to full text screening. Due to heterogeneity of definitions in the articles, 33% (n = 101) of abstracts were screened by both reviewers, with a high level of agreement (K = 0.75) [25]. Two members of the reviewing team were listed authors of included articles, for these, the third reviewer (who was not a listed author) completed the screening to reduce bias. Citation mining with full text review identified a further 25 articles, most frequently due to swallowing assessment not being explicitly described in the title or abstract. Following all stages of screening, 117 articles were included in the review.
Study Characteristics
Reporting of the co-occurrence between PLA and oropharyngeal dysphagia has exponentially increased in the last 15 years (75% of all papers included in this review). Most articles were from Europe (34%) and North America (32%). 95% of primary authors were Ear, Nose and Throat physicians/surgeons and/or Speech Pathologists. Patients were across a range of medical and surgical specialties and the age range was 18–97 years. Details have been reported in Online Resource 4 - Included articles organized alphabetically by author. Study designs were predominantly observational or case studies. Of the articles which included statistical analyses, there were ten cross-sectional, one cohort, two case-control studies, as well as and three case series.
Included articles reported ≥ 1 PLAs co-occurring with oropharyngeal dysphagia. Most articles reported motion impairment (n = 78), followed by obstruction to bolus flow or airflow (n = 31), mucosal abnormalities (n = 29), glottal insufficiency (n = 18), change of shape (n = 19), and abnormal movement pattern (n = 7). Oropharyngeal dysphagia was reported differently across articles using: validated swallowing outcome measures/scoring systems (n = 101), validated patient reported symptom tools (n = 18), unvalidated measures and/or patient reported symptoms (n = 13), sensory tests (including laryngeal adductor reflex testing or flexible endoscopic evaluation of swallowing with sensory testing (FEESST) (n = 37) as well as binary classifications of presence of oropharyngeal dysphagia (n = 33), secretion accumulation (n = 33), pre-swallow pooling (n = 18), aspiration (n = 94), residue (n = 41) and regurgitation (n = 4).
Identification of Pharyngolaryngeal Abnormalities Seen Via Nasoendoscopy
59 different terms were used to label and report endoscopic PLAs impacting swallowing function. These were synthesized into 32 unique terms in six defined subgroups. Subgroup classification was motion impairment, glottal insufficiency, obstruction to bolus flow or airflow, mucosal abnormalities, change of shape, and abnormal movement pattern (see Table 1 and Online Resource 3 – All listed terminology).
Table 1 Categorization into subgroups and summary of nasoenndoscopic pharyngolaryngeal abnormalitiesFrequency of co-occurrence with Oropharyngeal Dysphagia and Statistical Analysis by Subgroup
Across the 117 articles included, there was variation in reporting due to available data. 99 articles were reported using frequency of PLAs co-occurring with oropharyngeal dysphagia alone, the remaining 18 articles included frequency of co-occurrence in addition to p- values to analyze the relationships between individual PLA and oropharyngeal dysphagia. Specific data are available in Online Resource 5 - Frequency counts of co-occurrence and statistical analysis.
Motion Impairment
Motion impairment was reported in 78/117 articles. In the motion impairment subgroup, the reported symptoms of oropharyngeal dysphagia included sensory impairment, secretion accumulation, and/or pre-swallow pooling, and/or aspiration and/or residue.
Three of the eight abnormalities (UVFMI, velopharyngeal insufficiency, arytenoid motion impairment) had statistical analysis completed indicating an association with oropharyngeal dysphagia. In addition to these, two other abnormalities (bilateral vocal fold motion impairment - not in midline); reduced pharyngeal wall movement) also had a frequency count ≥ 5 articles or ≥ 50 participants co-occurring with oropharyngeal dysphagia. Three abnormalities (arytenoid prolapse/collapse; subluxation/ankylosis of cricoarytenoid joint; laterofixation of vocal fold) did not have statistical analysis or required frequency count for reporting.
Specifically, for UVFMI, meta-analysis indicated an association between UVFMI and aspiration (RR 1.49, 95% CI, 1.15–1.92) with low heterogeneity (I2 = 21%) [27,28,29,30,31,32,33]. Prevalence data indicated 80% (95% CI 0.65–0.90) of participants with UVFMI had residue [30] and 41% (95% CI, 0.35–0.47) had aspiration or a weak cough [27,28,29,30,31,32,33].
Glottic Insufficiency
Glottic insufficiency was reported in 20/117 articles. Across glottic insufficiency symptoms of oropharyngeal dysphagia include sensory impairment, secretion accumulation, and/or pre-swallow pooling and/or aspiration and/or residue.
Incomplete glottic closure (unspecified) and vocal fold atrophy/bowing both had statistical analysis completed indicating an association with oropharyngeal dysphagia as well as frequency count of co-occurrence ≥ 5 articles or ≥ 50 participants pooled across all the available literature. Phonatory gap/chink did not have statistical analysis or required frequency count for reporting.
Prevalence data demonstrated 84% (95% CI, 0.77–0.90) of participants with incomplete glottic closure had secretion accumulation [34] and 63% (95% CI, 0.38–0.84) were reported to aspirate [27].
Obstruction to Bolus Flow or Airflow
Obstruction was reported in 31/117 articles with various symptoms of oropharyngeal dysphagia including sensory impairment, secretion accumulation, and/or pre-swallow pooling and/or aspiration and/or residue. No articles commented on severity of obstruction to bolus flow or airflow across reported PLAs.
Edema had statistical analysis and frequency count with association/co-occurrence to oropharyngeal dysphagia. One article reported association between edema of unspecified location (RR 2.46, 95% CI, 1.53–3.96) [27] and arytenoid edema (RR 1.67, 95% CI, 0.13–20.88) [18] and oropharyngeal dysphagia. Bilateral true vocal fold motion impairment (in midline position) had one article reporting no association with aspiration [35], this was the only article to show negative association.
Glottic, subglottic, and infraglottic airway obstruction only had required frequency count, and the remaining two in this subgroup (cricopharyngeal prominence; midline protrusion) had neither statistical analysis nor frequency count.
Prevalence data indicated 45% (95% CI, 0.35–0.54) of participants with edema - unspecified location [27], 32% (95% CI, 0.17–0.51/0.16–0.50) of participants with arytenoid/interarytenoid edema [36], 36% (95% CI, 0.18-0.0.57) of participants with true vocal fold edema [36] and 20% (95% CI, 0.01–0.72) of participants with subglottic edema/stenosis [36] had reported aspiration. There was also prevalence of 85% (95% CI, 0.72–0.93) interarytenoid +/- arytenoid edema [18] with sensory impairment.
Mucosal Abnormalities
Mucosal abnormalities were reported in 29/117 articles with all reporting symptoms of oropharyngeal dysphagia including sensory impairment, secretion accumulation, and/or pre-swallow pooling and/or aspiration and/or residue.
Of the seven PLAs in this subgroup, only hematoma had one article reporting an association with sensory impairment [37]. Erythema and ulceration/granulation/granuloma had no statistical analysis completed; however, they did have the required frequency count for reporting. There was evidence from single articles, with rate ratio estimated by our team from summary statistics, for association of vocal fold erythema (RR 1.61, 95% CI, 0.26–10.06) [31] and vocal process granuloma (RR 1.11, 95% CI, 0.38–3.19) [31] with aspiration.
The remaining four PLAs in this subgroup (sloughing; cyst; scarring/synechiae/adhesions; laryngeal lesion) did not have statistical analysis or required frequency count for reporting.
Individual prevalence data indicated 32% (95% CI, 0.16–0.52) risk of aspiration for both arytenoid and vocal fold erythema [36]. Also, a 9% (95% CI, 0.00-0.41) and 32% (95% CI, 0.13–0.57) respective risk of aspiration with vocal process ulceration and granuloma [36].
Change of Shape
Change of shape was reported in 19/117 articles, none of which included statistical analysis to demonstrate association with oropharyngeal dysphagia.
Frequency of co-occurrence in change of shape has been reported for; partial/complete removal of; epiglottis, base of tongue, true vocal folds, arytenoids and false vocal folds resulting pre swallow pooling and/or secretion accumulation and/or aspiration and/or residue.
PLAs without required frequency count included partial removal or absence of arytenoids; aryepiglottic folds; pyriform sinus and lateral wall; supraglottis, as well as upright epiglottic/epiglottis stump and supracricoid laryngectomy.
Abnormal Movement Pattern
Abnormal movement patterns were reported in 7/117 articles across the pharyngolarynx. There were no articles with statistical analysis and ≤ 5 articles or ≤ 50 participants across articles for tremulous movements of the laryngopharynx to indicate an association with oropharyngeal dysphagia.
Mixed Pharyngo-Laryngeal Abnormalities
One article reported a statistical association between grouped laryngeal abnormalities (edema, ulceration, prolapse and unilateral vocal fold motion impairment) and aspiration [38]. Whilst another article reported one or more abnormal laryngeal findings (vocal fold edema, mucosal changes, subglottic stenosis, or motion impairment) were not associated with aspiration [1] (Table 2).
Table 2 Clinician’s Guide: Strength of evidence by subgroup



Comments (0)