
Remember me







From January 2011 to December 2024, 147 children had a diagnosis of pyelonephritis noted in the CT report. 43 children were excluded for the following reasons. In 10 children CT was not performed in the emergency department, and they were not admitted to the hospital for acute symptoms related to pyelonephritis. On retrospective review of the CT there was no evidence of pyelonephritis in eight children, three of whom had renal scarring and none of them had clinical diagnosis of UTI or pyelonephritis. Eight children had severe developmental delay due to cerebral palsy (n = 4) or chromosomal abnormalities (n = 4). Six children had tumors and were treated with chemotherapy. Five children had prior surgery for urologic anomalies. Two children had a history of recent trauma. One child had Henoch Schoenlein purpura. One child had Aport syndrome. One child who presented with malignant hypertension had acute renal ischemic changes secondary to renal artery stenosis due to fibromuscular dysplasia. One child had history of a myelomeningocele with neurogenic bladder (Fig. 1).
Fig. 1
Flow chart of children accepted to the study
The final study group included 104 children (79 females and 25 males) younger than seven years with an average age of 4.8 years.
19 children had a history of prematurity (gestational age range from 30 to 36 weeks). 12 children had a history of UTI, and two had VUR.
Clinical presentation and physical examination findingsThe most common presenting symptoms were fever (91/104, 87.5%), abdominal pain (82/104, 78.8%), and vomiting (59/104, 56.7%). Only five of the 104 children had flank or back pain (4.8%) and 34 children (32.7%) had one or more of the following urinary symptoms: dysuria (n = 17, 16.3%), urinary frequency (n = 6, 5.8%), urinary incontinence (n = 5, 4.8%), decreased urine output (n = 3, 2.9%), odorous urine (n = 1) and penile pain (n = 1). Ten of the 104 children (9.6%) had diarrhea, three (2.9%) had cough, three (2.9%) had headaches, and three (2.9%) had hip pain.
On physical examination, the most common findings were right lower quadrant tenderness (47/104, 45.2%) and diffuse abdominal tenderness (13/104,12.5%). Flank, back, or suprapubic tenderness was found in 21 of the 104 children (20.2%); flank or back tenderness were found in 13 (12.5%) and nine (8.7%) had suprapubic tenderness.
In 33/104 children (31.7%), US was performed to evaluate for appendicitis before the CT scan.
In 34/104 (32.7%) the primary indication for the CT was to evaluate for pyelonephritis. In 17/104 (16.3%) children the diagnosis of appendicitis and either UTI or pyelonephritis were considered before the CT scan.
In 53/104 children (51.0%), a diagnosis of UTI or pyelonephritis was not in the differential diagnosis before the CT scan (Figs. 1 and 2). In 38 of these 49 (77.6%), appendicitis was the primary indication. In the other 14 children, the indication for CT scan was related to symptoms and no specific diagnosis was indicated in the medical records: generalized abdominal pain with fever (n = 8), right lower quadrant pian (n = 3), fever and vomiting (n = 1), fever and rectal pain (n = 1), and bloody stool (n = 1). In one child CT was performed to evaluate for a false diagnosis of pelvic cystic mass by US. Most children (73/104, 70.2%) were admitted for treatment of pyelonephritis ranging from 1 to 13 days (average 3.5 days).
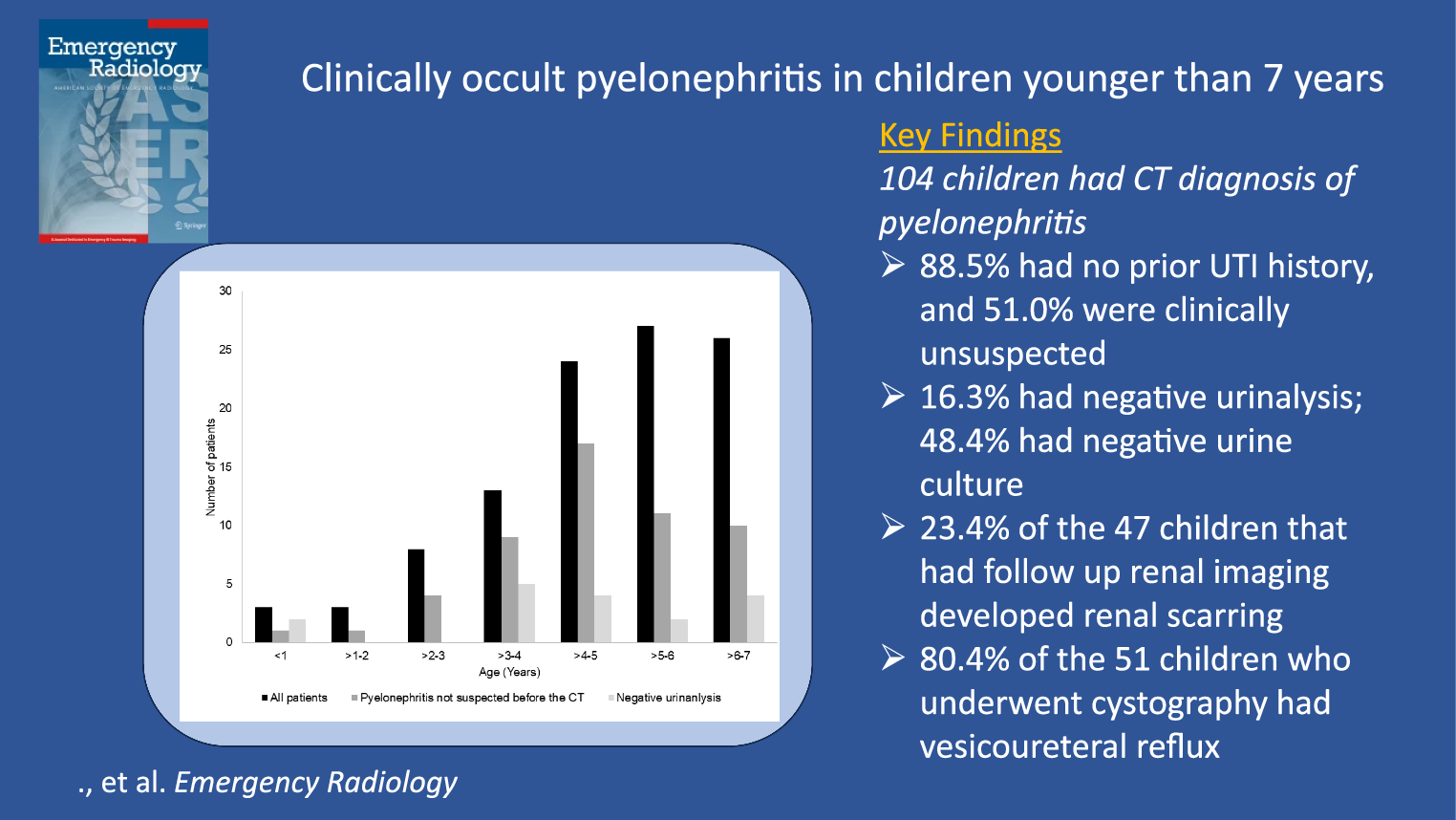
Fig. 2
Cases of pyelonephritis not suspected clinically and with negative urinalysis in the different age groups
Laboratory resultsMost (81/104, 77.9%) of the children had leukocytosis. Urinalysis was negative in 17/104 children (16.3%). Urine culture was obtained in 96 of the 104 children (92.3%) and in 46 (48.4%) of the children, urine culture was either negative (n = 34), showed colony counts < 50,000 CFU/mL (n = 4), or was contaminated (n = 8) and positive with colony counts > 50,000 CFU/mL in 43 (51.6%). Escherichia coli was the most common pathogen (36/49, 87.8%). Other pathogens included Enterococcus sp. (n = 4), Proteus mirabilis (n = 1) and Klebsiella sp. (n = 1), Staphylococcus aureus (n = 1).
In four of the 49 children with positive cultures, the urinalysis was normal. Thus, per American Academy of Pediatrics (AAP) criteria, in only 45/104 patients (43.3%) did the lab results confirm the diagnosis of UTI. In four other children (4/104, 3.8%), the culture was less than 50,000 CFUs per mL and in eight children (8/104, 7.7%) the urine was contaminated.
Negative urinalysis (p = 0.182) and negative urine culture (p = 0.638) were not significantly associated with age.
26 children received antibiotics before the urinalysis and urine culture. Urinalysis was positive in 21 children and urine culture was positive in 14 children. Only 12/26 (46.2%) had both positive urinalysis and urine culture.
CT findingsPyelonephritis was found in 126 kidneys: right (n = 48), left (n = 34), and bilateral (n = 22). The most common findings were hypodensity (n = 109), striated nephogram (n = 89), urothelial enhancement (n = 50), perirenal stranding (n = 46), and renal abscesses (n = 7, Figs. 3 and 4). Other findings included hydronephrosis (n = 13) and renal scarring (n = 12). Only three children with renal scarring had a prior history of UTIs. One child had a solitary kidney. In one child, in addition to pyelonephritis, tip appendicitis was diagnosed and confirmed by surgery.
Fig. 3
A 3 year-old female presented with fever, cough, vomiting, diarrhea, and leukocytosis (14,900 WBC/mL). Urinalysis and culture obtained from bladder catheterization were negative. A CT abdomen was obtained, due to concern for appendicitis, that demonstrated right-sided pyelonephritis. Coronal post-contrast CT demonstrates multifocal wedge-shaped hypodensities with striated nephrogram, and diffuse swelling of the right kidney
Fig. 4
A 6 month-old boy who presented with fever, intermittent fussiness, and leukocytosis (39,000 WBC/mL) was initially evaluated with US for intussusception. Urinalysis was negative on admission and later urine culture was positive for E. coli. CT of the abdomen was obtained to evaluate for a mass or inflammatory process; a diagnosis of pyelonephritis was not considered. Axial post-contrast CT (A) shows diffuse swelling and multifocal hypodensities in the left mid-pole kidney, and a round hypodensity in the anterior cortex with wall enhancement compatible with an abscess (arrowhead). A voiding cystourethrogram (B) demonstrates left grade 5 vesicoureteral reflux with a droopy lily sign compatible with a reflux to a lower pole of a duplex kidney. Due to recurrence of UTIs, he subsequently had circumcision and was placed on daily antibiotics. A left ureteral reimplantation was performed after he developed recurrent pyelonephritis
There was no significant association (p = 0.579) between age and clinical occult pyelonephritis.
Follow-upClinical follow-up records of at least four weeks were available in 77 of 104 children (74.0%) with an average of 2.9 years (range 28 days to 10.9 years). 12/104 children (11.5%) with no history before the admission of prior UTI had recurrent UTI, 16 (15.4%) had functional bladder abnormality, and 5 (4.8%) had recurrent pyelonephritis.
Follow-up renal imaging was performed at least four weeks after the initial CT scan in 47 of 104 children (45.2%). Of these, 30 underwent only renal ultrasound, 10 had ultrasound plus either follow-up CT (n = 4), DMSA (n = 5), or both (n = 1), and 7 underwent only follow-up CT. Ultrasound (n = 40) revealed new renal scarring in five kidneys. Additional imaging confirmed scarring in two patients (one by DMSA and one by both DMSA and CT) and detected new scarring in four others (one by DMSA and three by CT). Among the seven children who had only CT follow-up, scarring was identified in two additional patients. Overall, 11 of 47 children (23.4%) had new renal scarring on follow-up imaging.
Seven follow up CT scans on other patients demonstrate renal scarring in 2 additional patients. Overall, 11 of the 47 children (23.4%) had new renal scarring on follow-up imaging studies.
VCUG was performed in 51 of the 104 children (49.0%), of whom 41 had VUR (80.4%); 26 of them had dilated (grade 3 to 5) VUR (63.4%). In addition, one child had bilateral Hutch diverticula, and another child had a small right periureteral diverticula. Six female children had spinning top urethra indicating functional bladder abnormality, and one child had trabeculated bladder secondary to bladder functional abnormality. Two children had duplex kidneys with reflux to the lower moieties (Fig. 2).
There was no significant difference between degree of renal involvement and renal scarring (p = 0.978) or dilated VUR (p = 0.751).
18 children were treated with either unilateral (n = 7) or bilateral (n = 11) ureteral reimplantation, and four children were treated with bilateral Deflux injection. One child had an incision of a small posterior urethral valve.
Comments (0)