
Remember me




Pre-Exposure Prophylaxis (PrEP) is a highly effective biomedical intervention for HIV prevention [1]. However, its population-level impact is contingent upon consistent adherence and persistence, with discontinuation posing a significant challenge [1]. In Brazil, PrEP has been available free of charge through the Unified Health System (Sistema Único de Saúde, SUS) since 2017, targeting key populations at higher vulnerability to HIV acquisition [1]. Despite this access, PrEP interruption rates remain a concern [1]. This study aimed to identify factors associated with PrEP discontinuation among users within the Brazilian SUS, utilizing data from a national registry.
This case-control study used retrospective data from PrEP users monitored between 2018 and 2020 in Brazil. Data were extracted from the Medicines Logistics Control System (SICLOM), the national database for antiretroviral drugs which also facilitates clinical and dispensing monitoring for PrEP users [2]. Participants were PrEP users within the SUS, which provides PrEP following national guidelines primarily to gay men and other men who have sex with men (MSM), transgender people, sex workers, and individuals in serodiscordant partnerships who report specific risk behaviors [3].Clinics providing PrEP are public health facilities integrated into the SUS network. While PrEP is provided without direct cost to the user, it is important to acknowledge that broader socioeconomic factors, such as education level, income, and regional disparities, significantly influence HIV vulnerability, healthcare-seeking behaviors, and potentially engagement with PrEP services across Brazil [4]. This study examines factors among a cohort already initiated on PrEP and registered in SICLOM, thus having navigated initial access barriers.
Cases were defined as users who discontinued PrEP at least once due to reasons recorded in SICLOM, including reactive HIV test, changes in other laboratory tests, poor medication adherence, adverse events, user’s decision, or suspicion of acute viral infection. Controls were users who maintained PrEP during the study period. A total of 629 cases were matched 1:10 by sex at birth and age to 6290 controls, selected from a population of 34,000 PrEP users. Variables collected included baseline sociodemographic characteristics, sexual behaviors, clinical history, and follow-up data on adverse events, self-reported adherence, and laboratory tests. Logistic regression was used to calculate adjusted odds ratios (aOR) with 95% confidence intervals (CI) for factors associated with PrEP discontinuation; variables with p < 0.05 in univariate analysis were included in the multivariate model. Statistical significance was set at a two-sided p < 0.05. The study received ethical approval from the Faculty of Medicine of the University of Brasilia (CAAE: 07448818.0.1001.5558), and all data were anonymized.
The total sample comprised 6,919 individuals. Cases had a median follow-up of 8 months (Interquartile Range 4–12), significantly shorter than controls at 13 months (IQR 7–20) (p < 0.001). The overall sample was predominantly composed of individuals assigned male at birth (83%), self-identifying as homosexual (72%), aged 30–39 years (34%), white (55%), and with 12 or more years of schooling (69%). There were no statistically significant differences (p > 0.05) between cases and controls at baseline regarding age group, sexual orientation, gender identity, race/color, and schooling level.
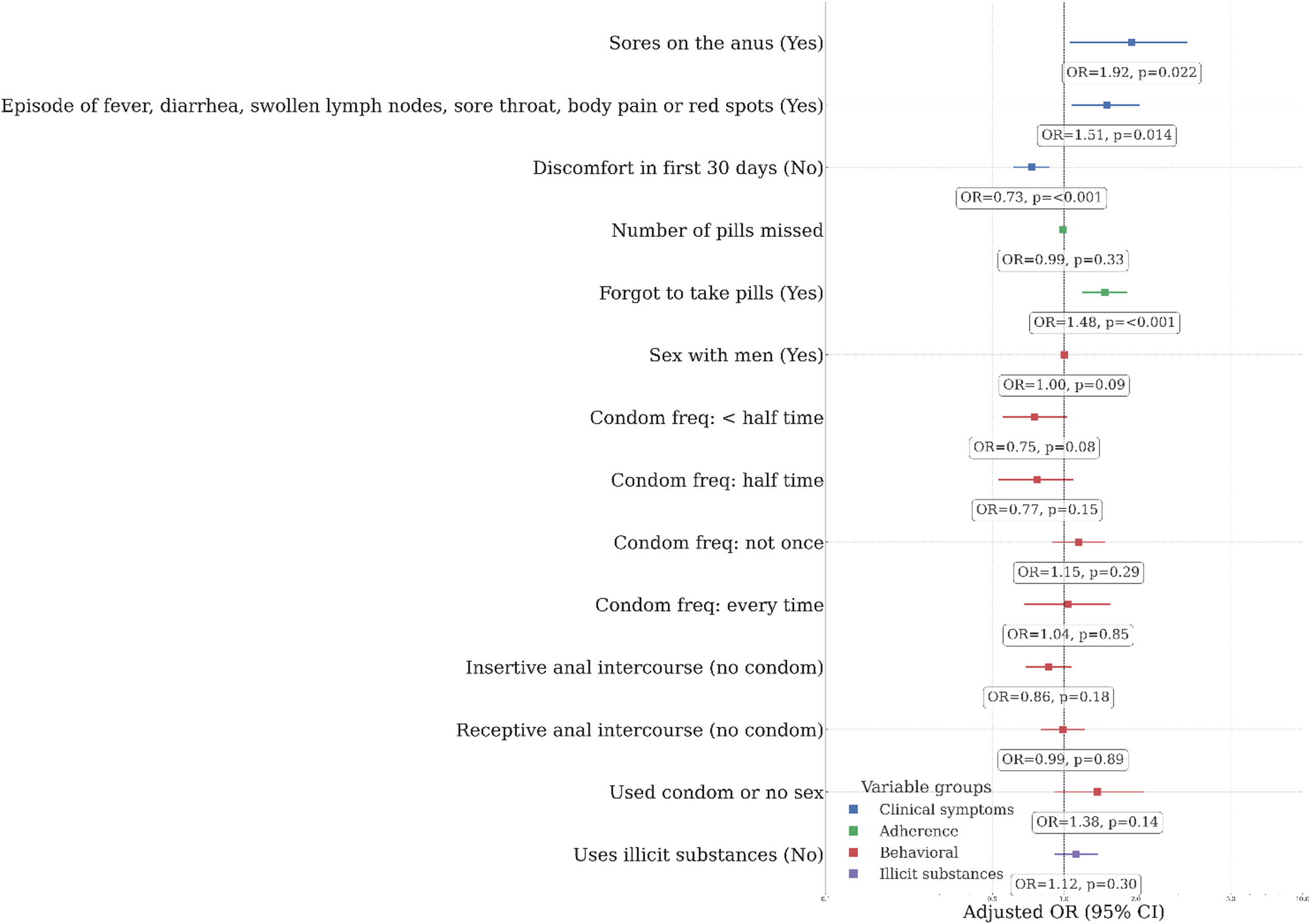
Multivariate logistic regression analysis (Fig. 1) identified several factors significantly associated with PrEP discontinuation. Users reporting anal lesions up to 6 months before PrEP initiation had nearly twice the odds of discontinuing PrEP (aOR: 1.92; 95% CI 1.06–3.28; p = 0.022). Experiencing symptoms suggestive of active infection (e.g., fever, diarrhea, swollen lymph nodes, sore throat, body aches, or skin rashes) within the first 30 days of starting PrEP was also associated with increased odds of discontinuation (aOR: 1.51; 95% CI 1.07–2.07; p = 0.014). Frequent medication forgetfulness, reported as the primary reason for missing doses in the first 30 days, was a strong predictor of interruption (aOR: 1.48; 95% CI 1.19–1.84; p < 0.001). Conversely, users who did not experience any adverse effects during the first month of PrEP were less likely to discontinue (aOR: 0.73; 95% CI 0.61–0.87; p < 0.001).
Fig. 1
Multivariate logistic regression analysis of factors associated with interrupted PrEP among users in Brazil (N = 6,919). Figure 1 displays adjusted odds ratios (aOR) with 95% confidence intervals (CI) and p-values from a multivariate logistic regression model examining factors associated with PrEP discontinuation. Cases (n = 629) were users who interrupted PrEP; Controls (n = 6,290) were users who maintained PrEP, matched by sex at birth and age. The model was adjusted for variables significant in univariate analysis. Factors shown are: Previous anal lesions (Yes vs. No), Active infections in first 30 days (Yes vs. No), Medication forgetfulness as main reason for missed doses (Yes vs. No), and No adverse effects in first month (Yes vs. No [i.e., experienced adverse effects]). The vertical line at aOR = 1.0 indicates no effect
This study identified that early clinical experiences, specifically the occurrence of active infections or the absence of adverse events within the first 30 days of PrEP initiation, and adherence-related behavior, such as medication forgetfulness, are significant predictors of PrEP discontinuation in a large cohort of Brazilian SUS users. The presence of previous anal lesions also emerged as a risk factor. The median time to discontinuation of 8 months is relatively short compared to some international reports, which have found average discontinuation times closer to 1.5 years or 15 months [5]. This discrepancy may reflect differences in study methodologies, definitions of discontinuation, or specific characteristics of the Brazilian PrEP program and its users.
The findings underscore the critical importance of the initial period after PrEP initiation. The association between active infections in the first 30 days and discontinuation suggests that users might misinterpret these symptoms as severe side effects or become discouraged. Conversely, the protective effect of not experiencing adverse events highlights that a smoother initial experience likely fosters continued use. Medication forgetfulness, a common challenge in chronic medication adherence [6], directly impacts PrEP effectiveness and continuation. While often unintentional, “forgetfulness” can also be a manifestation of deeper issues such as waning motivation, unacknowledged side effects, or changes in life circumstances that impact routine, suggesting that interventions may need to go beyond simple reminders to address these underlying complexities.
The context of PrEP provision within the SUS, free at the point of care, is essential. It indicates that even when direct medication costs are removed, other barriers to persistence, particularly those related to early tolerability and behavioral aspects of adherence, remain significant. While this study focused on individual and clinical factors among those already engaged in PrEP care, it is important to recognize that broader social determinants of health—including education, poverty, and race—are known to create significant inequalities in HIV risk, access to prevention, and healthcare engagement in Brazil [7].These wider societal factors likely influence who initiates PrEP and may also indirectly affect long-term persistence, even if not directly measured as reasons for discontinuation in this specific cohort. The individuals in this study, by being registered in SICLOM, have already overcome initial access barriers that are often socioeconomically patterned [8].
Comments (0)